Int J Legal Med (2004) 118 : 163–169DOI 10.1007/s00414-004-0433-8
M. Findeisen · M. Vennemann · B. Brinkmann · C. Ortmann · I. Röse · W. Köpcke · G. Jorch · T. Bajanowski
German study on sudden infant death (GeSID): design, epidemiological and pathological profile
Received: 15 February 2003 / Accepted: 22 August 2003 / Published online: 24 March 2004
Abstract The German study on sudden infant death
age, gender and region (n=1,118). The response rate of the
(GeSID) is a multi-centre case-control study aiming at the
controls was 58.7%. Data were linked with medical records
assessment of etiological factors and risk factors of SIDS.
obtained from obstetrics departments, the children’s hos-
This report describes the study design and the methods
pitals, and general practitioners. Death scene investigation
applied and presents some general findings. Between
was performed in 4 study areas (cases: n=64, controls:
1998 and 2001, 455 cases of sudden and unexpected death
n=191). All cases were classified into one of 4 categories
of infants aged between 8 and 365 days were recruited
using defined criteria: 7.3% of the children were assigned
into the study. The study comprised at least 11 out of the
to category 1 (no pathological findings: SIDS), 61.1% to
16 German states with 18 centres involved. In 1999 and
category 2 (minor findings: SIDS+), 20.4% to category 3
2000, 75% of all SIDS cases registered with the Federal
(severe findings: SIDS+) and 11.2% to category 4 (find-
Office of Statistics (ICD 10/R95, n=384) in the study area
ings which explained the death: non-SIDS). In case con-
were recruited into the study (n=286). A standardised au-
ferences the previous history and circumstantial factors
topsy including extended histology, microbiology, virol-
were included and an extended category (E-cat.) was de-
ogy, toxicology and neuropathology investigations was
fined. The consideration of these factors for the final clas-
carried out. Of the parents 82% (n=373) agreed to fill in
sification is of great importance in the causal explanation
an extensive questionnaire containing 120 questions re-
of some cases. An analysis of 18 main variables in cases
flecting all important aspects of the infant’s development.
of categories 1–3 (SIDS) compared to the cases of cate-
For each SIDS case, the parents of three living control in-
gory 4 (non-SIDS) showed significant differences for the
fants were interviewed. These controls were matched for
sleeping position, coughing the day before death and breast-feeding indicating that the cases of both groups should be separated for further analyses. Electronic Supplementary Material Supplementary ma- terial is available in the online version of this article at
A list of the collaborating authors and institutes is given in theappendix.
http://dx.doi.org/10.1007/s00414-004-0433-8
Keywords Sudden infant death syndrome (SIDS) ·
Study centre “Studie Plötzlicher Säuglingstod”,
Standardised investigation protocol · Pathological and
University of Münster, Münster, Germany
extended categories · Case-control study
B. Brinkmann (✉) · T. BajanowskiInstitute of Legal Medicine, Röntgenstrasse 23, 48149 Münster, GermanyTel.: +49-251-8355160, Fax: +49-251-8355158,
In Germany, sudden infant death syndrome (SIDS) is still
Institut for Legal Medicine, University of Jena
the leading cause of death in infancy after the neonatal pe-
riod. While the incidence dropped in the 1990s from 1.4
Institute for Pathology, University of Magdeburg
per 1,000 live births (n=1,283) to 0.6 in the year 2000(n=482), the SIDS mortality rate is still much higher in
W. KöpckeDepartment of Medical Informatics and Biomathematics,
Germany, than for example in the Netherlands (0.17‰)
In various international studies as well as in the West-
G. JorchChildren’s Hospital, University of Magdeburg
falian Cot Death Study [3, 4], risk factors such as the
prone sleeping position, smoking of the mother during
pregnancy and overheating of the infant were identified
Two local registry offices in the area where the infant had died
[5, 6, 7, 8, 9] and highlighted in prevention campaigns
were approached and each was asked to select five control infants
leading to a significant decrease in the SIDS incidence [1,
matched for age, gender and the geographical region. These con-
trol infants had been born 4–6 weeks after the case infant, so by the
Based on these results, the German Federal Ministry
time the interview was done they had the same age as the index
for Science and Education supported the GeSID (German
case. From these controls the first 3 giving informed consent andwho did not fulfil the following exclusion criteria were selected:
study on sudden infant death) to investigate SIDS in Ger-many. This interdisciplinary project started with a pilot
– Age less than 8 days or more than 1 year– Infant admitted to hospital prior to the time of interview
study in 1996/1997 and the data collection period for the
main study was performed from November 1998 to Octo-
ber 2001 as a multi-centre case-control study in 11 federal
– Informed consent could not be obtained.
The questionnaire consisted of 106 questions dealing with majortopics such as family and child history, socio-demographic factors,sleeping situation, feeding of the infant, cigarette and alcohol con-
sumption of the parents during pregnancy and after birth. In an an-nex data on antenatal obstetrician visits of the mother, vaccinations
Initially 13 forensic pathology institutes co-operated with the study
received by the infant, and so-called well-baby check-ups are given.
centre. Because of the decreasing SIDS incidence the area was ex-
The socio-economic questions were based on “MONICA” (Moni-
tended in mid-2000 to 18 centres in 11 states (Table 1). This area
toring Trends and Determinants in Cardiovascular Diseases, Augs-
covered about 50% of Germany as well as 50% of all births.
burg Cohort Study 1984–1995) [13] and social status was calcu-
All 18 centres obtained the approval of their local medical
lated according to the modified “Scheuch Index” [14]. The ques-
ethics committees and the control recruitment in each state was ac-
tionnaire was filled in by trained interviewers who visited the par-
cepted by the state data protection officer.
ents at their homes. For quality control, interviews were recordedon tape with the consent of the parents and every 10th interviewwas checked for accuracy.
All infants who seemed to die suddenly and unexpectedly from the
results of necropsy were to be reported to the study centre by theemergency doctor, the pediatrician, the general practitioner or by
The physician who made the well-baby check-ups filled in a ques-
police officers. Exclusion criteria were:
tionnaire containing 20 questions relating to health status and
– Death prior to 8 days or later than 12 months after birth
threatment, vaccination status, and suspected child abuse and/or
– Cases where death was expected due to known diseases
neglect. The delivery clinic was asked to provide the discharge
documents, containing information about previous pregnancies,
– Parents had insufficient knowledge of the German language so
delivery mode of the index case and the Apgar score. If a child had
that informed consent could not be obtained.
been admitted to hospital, the related records were also evaluated. Table 1 Institutes of Legal
project, cases examined and re-sponse rate for interviews
aDeath scene investigation per-formed.
A 10-point questionnaire was applied if a child had been previ-
Table 2 Pathology categories and criteria for diagnoses
Without pathological findings from autopsy and
A standardised autopsy protocol (SAP) was introduced to all study
centers involved (ESM Tables. I–IV, Fig. 1). This SAP is in accor-dance with the European guidelines for medico-legal autopsies
With minor pathological findings in autopsy and
[15] and closely reflects the international standardised autopsy
protocol [16] as well as protocols used in other studies on SIDS [5,
Minor infections of the respiratory tract
17, 18]. The autopsy included a thorough external examination, a
Rhinitis, otitis media, pharyngitis, tracheitis
complete internal examination (ESM Table I), extensive histology(ESM Table II, Fig. 1), a full analytical toxicology scheme (ESM
Table III), and microbiology and virology (ESM Table IV).
peribronchitis Mild/intermediate forms of bronchiolitis and of interstitial pneumonia
Tonsillitis Mild abnormalities and congenital deformations
A total of 20 samples were taken from defined organs and tissuesand were further processed into 90 microsections for different
staining methods (ESM, Table II, Fig. 1). The first assessment was
made in the department performing the autopsy. The validation of
these findings was done at the study centre by an experienced his-tologist using coded slides. The histology was evaluated qualita-
tively and quantitatively (grading) and every 10th case was sent to
Mild forms of metabolic disorders without
an expert in paediatric pathology for confirmation. A weighted
kappa index was calculated to evaluate the interreader agreement.
Interstitial pneumonia showing bacterial superinfection
The “routine” examination was based on the SAP (ESM Tables I
Enteritis with exsiccosis Pericarditis/myocarditis, especially of the
borderline type Mild forms of meningo-encephalitis
Body fluids, tissue samples and stomach contents were taken(ESM Table III) and toxicological analysis was performed for the
1. Ethanol, methanol, acetone, iso-propanol; blood/serum; head-
space gas chromatography [18], cut-off 20 µg/ml
2. Carboxyhaemoglobin; cardiac blood, photometry [19]3. Amphetamines, cannabinoids, cocaine, opiates; acetone extract
from cardiac blood, immunology screening [20]
4. General unknown analysis [21] for the detection of antiepilep-
tic drugs (carbamazepine, phenobarbital), benzodiazepines andmetabolites, hypnotics (e.g. diphenhydramine), antidepressants(e.g. amitriptyline, maprotiline), neuroleptics, opiates and otheranalgetic drugs; blood, liver tissue, determined by gas chroma-
tography mass spectrometry after enzymatic cleavage of metabo-lites and an extraction procedure.
A review committee consisting of a forensic pathologist, a paedia-trician, a histologist, a microbiologist and an epidemiologist re-viewed all cases to determine the cause of death and to assign a
case to a specific category, using a modified version of the classi-fication proposed by Taylor and Emery [22]. As the information
Virology screening was done for the detection of defined viruses
derived from cases with a parental interview was much more de-
by PCR methods in the tracheal mucosa (influenza A+B, parain-
tailed than that from cases lacking an interview, a second category
fluenza virus, adenovirus, respiratory syncytial virus and cy-
was introduced. Cases were allocated to a P-cat. (pathological cat-
tomegalovirus) and in the stool (adenovirus, enterovirus, rotavirus,
egory), and interviewed cases to an E-cat. (extended category),
based on the pathological findings, the previous history and the
Microbiology was carried out using conventional techniques
circumstances of the death (Tables 2 and 3).
for the detection of bacteria in smears taken from defined regionsand tissue samples (ESM Table IV).
All data were entered with a case-related code number. Data record-ing and statistical analysis were performed at the study centre using
Comparison of the data from the Federal Offices of Sta-
the SAS (Statistical Analysis System, version 6.12) software.
tistics and the cases registered in the study reveals that the
Table 3 Extended categories (E-cat.) with additional informa-
For the age-matching criterion the overall difference in
tion on pathological categories and criteria deduced from infor-
mean age was 1 week (mean age of cases 19 weeks, con-
mation on the circumstances of the death and the previous
Previous history and circumstances of the death
Of thepaediatricians 69 did not complete the questionaire
P-cat. 1 or 2 in addition with minor findings in
and 34 infants had never been seen by a doctor. The re-
sponse rate to the questionnaire was therefore 95.3%. Dis-
charge letters were requested for 378 admissions to chil-
dren’s hospitals (response rate 93.4%, n=354).
A total of 1,491 discharge letters from delivery clinics
were requested. Data on 16 home deliveries could not be
obtained and 8 hospitals refused to participate (response
Possible suffocation in soft bedding No feeding: ≥12 h until 12th week of life,
≥14 h after the 12th week of life
P-cat. 1–4 and findings explaining the death
For the differences between interreader variability of the
histological diagnosis the weighted kappa index [24] was
Emergency doctor measured rectal temperature
used. The final diagnosis of the institute and the second
opinion in the study centre were compared for 433 cases
Body weight loss over several weeks with clear signs of dystrophy
(for 22 cases only 1 result was obtained): the weighted kappaindex was calculated as κ=0.67 (95% CI: 0.61–0.73). Thecomparison of the second and third diagnoses (n=120)
Table 4 Case recruitment in relation to the data of the Federal Of-
gave a similar level of agreement (κ=0.57; 95% CI: 0.45–
fice of Statistics with the diagnosis “SIDS” (ICD 10; R95) and thetotal infant mortality after the 7th day of life
Pathomorphological classification of cases (P-cat.)
All cases were classified by the committee into 1 of 4 cat-
egories using defined criteria (Table 2). Of the children
7.3% were assigned to category 1 (no pathological findings:
SIDS), 61.1% to category 2 (minor findings: SIDS+),20.4% to category 3 (severe findings: SIDS+) and 11.2%
recruitment rate was 67.3% out of 384 cases in 1999 and
to category 4 (findings which explained the death: non-
82.2% out of 286 cases in 2000 (Table 4).
SIDS). The distribution of cases with or without interviewinto the 4 categories did not differ significantly (Tables 5and 6). Extended classification by E-category (E-cat.)
Of the 455 cases recruited into the study, 82 parents did
The E-cat. was introduced to consider the previous his-
not consent to participate in the interview (18%). The in-
tory, the circumstances of death as well as pathological
terview was held 31 days after death on average.
findings (Table 3). Example: an infant with an upper air-
Table 5 Pathomorphological classification for all cases (n=455)
Proportions of response, contact and co-operation were
calculated according to the definitions of Slattery et al. [23]. Overall, 2,702 families were contacted, and 58.7%
Table 6 Pathomorphological
(P-cat.) and extended classifi-cation (E-cat.) for interviewed
with regard to the circumstances of death led to a decreasein category 2 and consequently to a significant increase incategory 3 (Fig. 1).
A total of 45 million inhabitants, 54.9% of the total popu-lation of Germany, live in the study areas. At 430,000 theannual number of births is approximately 55.7% of theoverall number. Taking into account that some states werefully covered in the investigation, that all major geo-
Fig. 1 Shifts in the classification of cases (P-cat.) due to the intro- duction of E-cat
graphical regions of Germany were included, and that theproportions of rural and urban regions were well bal-anced, and reflected those of the whole of Germany, the
way infection graded P-cat. 2 had been found dead with a
study area can be considered as being representative for
rectal temperature of 42.5 C°. Hyperthermia was consid-
ered to be the cause of death. Final classification: E-cat. 4.
To determine the incidence of SIDS in the study area,
The 82 cases lacking an interview were classified as P-cat.
the reported cases were compared with the annual data of
only. The distributions of the combined E-cat and P-cat.
the Federal Office of Statistics which suggest a high rate
revealed either no difference (P-cat. 4 and E-cat. 4; 11%)
of case recruitment into the study for the years 1999 and
or only minor differences in category 1 (P-cat. 8%, E-cat
2000 of 74.5% (official data for 2001 are not available at
2%) (Table 6). Major shifts were observed between cate-
gories 2 (P-cat. 60%, E-cat. 34%) and 3 (P-cat. 21%, E-cat.
The rate of parental consent of case families to the in-
53%). The combination of pathology and previous history
terview was high (82%), suggesting reliable findings re-
Table 7 Pathological categories and distribution of main variables (n=373)
lating to the epidemiology of SIDS. The average time in-
Among the 455 cases autopsied, only 7% remained with-
terval between death and interview of 31 days has logisti-
out significant findings in the pathology investigation
cal reasons but was in the range of other studies (ECAS
scheme (Table 5). This figure is further decreased if the
34 days [11], NZ study 28 days [25]). It has been shown
combined P/E-cat. criterium is applied (Table 6). Only ap-
in other SIDS studies that such a time interval did not in-
proximately 2% of all cases investigated were without find-
fluence the results, because parents are able to remember
ings in the pathology scheme as well as in the previous his-
in great detail what happened around the time of the in-
tory. Only 36% of cases with the combined score E-cat.
failed to offer an adequate explanation for the fatal outcome.
The overall response rate of controls (58.7%) was sim-
In particular the shift between categories 2 and 3 in the com-
ilar to response rates of other German studies [28]. In a
bined score shows that the consideration of circumstantial
sample of 54,000 deliveries from Westfalia [29] we found
factors and the previous history is of great importance in the
similar data for maternal smoking during pregnancy and
causal explanation of sudden unexpected death in infancy.
for birth weight of the infants as well as for maternal age
In conclusion a detailed investigation as carried out in
as in the present study, indicating that the controls are rep-
the GeSID study can contribute to explaining the cause of
resentative. However, a more detailed examination of
death in a considerable number of cases compared to a
these data will follow with the ongoing analyses.
routine autopsy alone and is a prerequisite for a high qual-
The κ-values for interreader variability of the histolog-
ity of epidemiological case-control studies. Some risk fac-
ical diagnoses demonstrate the quality of the standardised
tors for SIDS gradually change as more pathological find-
morphological investigations and the use of unique diag-
ings were detected by extensive postmortem investiga-
tions (Table 7). Therefore a more detailed epidemiological
Case ascertainment was thoroughly done using four
analysis of the moderately large categories of death is
categories. The Nordic study [30], the CESID study [31]
necessary to demonstrate statistically significant trends,
and the European Concerted Action on SIDS (ECAS) [17]
and statistically significant differences between subgroups
used three categories. In order to be able to compare the
and to develop focused prevention strategies.
data collected in this study with the data of the WestfalianCot Death Study [32], we used the same system again. Acknowledgements The study is supported by the Federal Ger- man Ministry for Science and Education (01 ED 9401/8). We
The categories 2 and 3 used in the German study corre-
thank H. Hansen and E.A. Mitchell for acting as consultants as
spond with the borderline SIDS or SIDS+ cases in these
well as E. Müller and T. Butterfaß-Bahloul who worked as recorders.
We thank the physicians of the health offices and the doctors of thechildren’s hospitals and the obstetric departments for sending usthe clinical documents and all paediatricians and general practi-tioners for filling in the questionnaire. We also thank the 32 inter-
viewers who undertook interviews during the 3 years of the studyand Schwertner Field Research, Augsburg, for performing the field-
To determine the strategy of the analysis in the case con-
work. We thank the police for supporting the parents and the
trol study, we analysed the distribution of 18 main factors
study. We thank all the local registry offices for sending us the ad-dresses of control families. Most importantly, the authors are in-
for SIDS in the categories defined. The statistical test ap-
debted to the parents who participated in this study.
plied to compare the subgroups 1–3 and 4 resulted in sig-nificant differences in 3 main variables:
– Breast-feeding showed an increase in P-cat. 4 (Table 7)
– The prone position was a more common sleep-related
pattern in P-cats. 1–3. There seemed to be a gradual de-
The following collaborating authors were from Institutes
crease of this risk factor in relation to an increase in the
severity of pathological changes. From a pathophysio-
– P. Bach, State of Brandenburg, Potsdam
logical point of view, this correlation seems highly
– B. Bockholt, Free University, Berlin (West)
plausible. On the other hand this link confirms the im-
– M. Bohnert, Albert-Ludwigs-University, Freiburg im
portance of the prone position as a contributing factor.
– Coughing the day before death: the stepwise increase in
– U. Cremer, Rheinisch-Westfälische Technische Hoch-
coughing from P-cat. 1 to P-cat. 4 correlated as a symp-
tom with the severity of upper airway infections. This
– U. Deml, Friedrich-Alexander-University, Erlangen
also confirms the accuracy of the grading of the patho-
– A. Freislederer, Universität-Gesamthochschule, Essen
– S. Heide, Martin-Luther-University, Halle
From the results (Table 7) it can be seen that the cases in
– W. Huckenbeck, Heinrich-Heine-University, Düssel-
P-cat. 1–3 show similarities (SIDS cases). The statistical
tests suggest that the epidemiological profiles of the cases
– K. Jahau, Otto-von-Guericke-University, Magdeburg
in subgroup 4 differ from those of the other groups. These
– H-J. Kaatsch, Christian-Albrechts-University, Kiel
cases (P-cat. 4) were therefore excluded from further epi-
– A. Klein, Friedrich-Schiller University, Jena
demiological analysis of SIDS cases and will be analysed
– W.J. Kleemann, Hannover Medical School, now Uni-
– K.-P. Larsch, A. Fiegut, Hannover Medical School
12. Wennergren G, Alm B, Øyen N et al. (1997) The decline in the
– H.W. Leukel, Johann-Wolfgang-Goethe-University,
incidence of SIDS in Scandinavia and its relation to risk-reduc-tion campaigns. Acta Paediatr 86:963–968
13. Keil U (1985) MONICA Project Region Augsburg. Manual of
– E. Rauch, R. Penning, Ludwig-Maximilians-University,
14. Winkler J (1998) Die Messung des sozialen Status mit Hilfe
– F. Rublack, Humboldt-University, Berlin (East)
eines Index in den Gesundheitssurveys der DHP. RKI-Schrif-
15. Brinkmann B (1999) Harmonisation of medico-legal autopsy
– G. Zimmer, Ruprecht-Karls-University, Heidelberg
16. Krous H (1996) Instruction and reference manual for the inter-
national standardised autopsy protocol for sudden unexpected
The following collaborating authors were from Institutes
infant death. J SIDS Infant Mortal 1:203–246
17. L’Hoir MP, Engelberts AC, van Well GTJ, Bajanowski T, Hel-
weg-Larsen K, Huber J (1998) Sudden unexpected death in in-
fancy; epidemiology determined risk factors related to a pa-
– D. Fischer, Children’s Hospital, Otto-von-Guericke-Uni-
thology classification. Acta Paediatr 87:1279–1287
18. Bajanowski T, Fürst P, Wilmers K, Beike J, Köhler H, Karger
B, Brinkmann B (2001) Dioxin concentrations in infant tissue
– W. Paulus, Institute of Neuropathology, University of
and sudden infant death. Int J Legal Med 116:27–32
19. Schütz H, Machbert G (1988) Photometrische Bestimmung
– C. Sauerland, Department of Medical Informatics and
von Carboxy-Hämoglobin (CO-Hb) im Blut. Mitteilung VIII
der Senatskommission für klinisch-toxikologische Analytik.
– M. Schlaud, MH Hannover Medical School
20. Käferstein H, Sticht G, Staak M (1989) Vergleich verschie-
– B. Schmidt, Institute for Virology, Friedrich-Alexander-
dener immunologischer Methoden mit einer Gc-MS Analyse.
21. Pavlic M, Haidekker A, Grubwieser P, Rabl W (2002) Fatal in-
toxication with omethoate. Int J Legal Med 116:238–241
22. Taylor EM, Emery JL (1990) Categories of preventable unex-
pected infant deaths. Arch Dis Child 65:535–539
23. Slattery ML, Edwards SL, Caan BJ, Kerber RA, Potter JD
1. Statistisches Bundesamt Deutschland (2001) http://www.statis-
(1995) Response rates among control subjects in case-control
2. Dutch Central Bureau of Statistics (CBS) (1997) Death by
24. Fleiss J (1981) Statistical methods for rates and proportions.
cause, age and sex in the years 1980–1997, Series A1 (in
Series in probability and mathematical statistics. Wiley, New
3. Jorch G, Findeisen M, Brinkmann B et al. (1991) Bauchlage
25. Becroft DMO, Thompson JMD, Mitchell EA (1998) Epidemi-
und plötzlicher Säuglingstod. Dtsch Arztebl 48:4266–4272
ology of intrathoracic petechial hemorrhages in sudden infant
4. Findeisen M, Jorch G (1991) Plötzlicher Säuglingstod: Epi-
death syndrome. Pediatr Dev Pathol 1:200–209
demiologische Daten. Dokumentationsband Expertenhearing.
26. Gibbons LE, Ponsonby A-L, Dwyer TA (1993) A comparison
of prospective and retrospective responses on sudden infant
5. Mitchell EA, Scragg R, Stewart AW et al. (1991) Cot death
death syndrome by case and control mothers. Am J Epidemiol
supplement: results from the first year of the New Zealand cot
27. Drews CD, Kraus JF, Greenland S (1990) Recall bias in a case-
6. De Jonge GA, Engelberts AC, Koomen-Liefting AJM, Kos-
control study on SIDS. Int J Epidemiol 19:405–411
tense PJ (1989) Cot death and prone sleeping position in The
28. Stang A, Ahrens W, Jöckel K-H (1999) Control response pro-
portions in population-based case-control studies in Germany.
7. Fleming PJ, Gilbert R, Azaz Y et al. (1990) Interaction be-
tween bedding and sleeping position in the sudden infant death
29. Ärztekammer Westfalen-Lippe (2001) Jahresauswertung 2001
syndrome: a population based case control study. BMJ 301:
30. Gregersen M, Rajs J, Laurensen H et al. (1995) Pathological
8. Beal S (1989) Sleeping position and SIDS. Lancet ii:512
criteria for the Nordic study of SIDS. In: Rognum TO (ed) Sud-
9. Schlaud M, Kleemann WJ, Poets CF, Sens B (1996) Smoking
den infant death syndrome. New trends in the nineties. Scandi-
during pregnancy and poor antenatal care: two major pre-
navian University Press, Oslo, pp 50–58
ventable risk factors for sudden infant death syndrome (SIDS).
31. Gilbert R, Rudd P, Berry PJ et al. (1992) Combined effect of
infection and heavy wrapping on the risk of sudden unexpected
10. Leach CEA, Blair PS, Fleming PJ et al. (1999) Sudden unex-
infant death. Arch Dis Child 67:171–177
pected deaths in infancy: similarities and differences in the epi-
32. Jorch G, Schmidt-Troschke S, Bajanowski T (1994) Epidemio-
demiology of SIDS and explained deaths. Pediatrics 104:e43
logische Risikofaktoren des plötzlichen Kindstodes. Ergeb-
11. L’Hoir MP, Engelberts AC, van Well GTJ et al. (1998) Case
nisse der westfälischen Kindstodsstudie 1990–1992. Monats-
control study of current validity of previously described risk
factors for SIDS in The Netherlands. Arch Dis Child 79:386–393
Infiltration Une récrudesence de la douleur dans les 24 heures suivant l'infiltration peut être possible : Dans ce cas, il est recommandé au patient de prendre le traitement antalgique habituel dont il dispose. Il est recommandé de même de ne pas conduire aprés une infiltration quelle qu'elle soit. Deux infiltrations différentes ne peuvent être réalisées le même jour ( en dehors d
Certains petits esprits argueront que si j’aimis la lettre Z à la première place, c’est pourcommencer ce livre en parlant de zob ou dezizi. Laissons ces obsédés du sexe à leur bêtise,pour aborder un sujet des plus sérieux : lazoophilie. accouplements hommes-chèvres ou hommes-canards, peu connaissent les poissondophiles. Pourtant, ils existent et il faut avouer que cetteforme de sexua
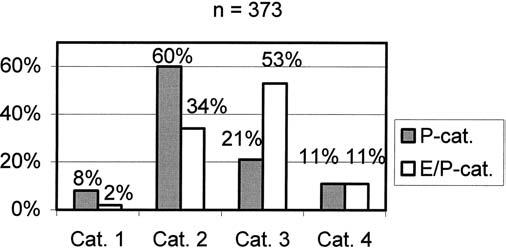 Table 6 Pathomorphological
Table 6 Pathomorphological