Laser in Conjunction with Endoscopic Forehead Surgery for Soft Tissue Masses
Chang Gung Memorial Hospital, Chang Gung University, Taipei, Taiwan
Running Title: Laser and Endoscopic surgery
ABSTRACT
Purpose: The use of the endoscopic techniques in plastic surgery has been a significant turn
around of the traditional techniques. However, the combination of the laser with
Method: Between January 1996 and January2003, 42 patients have been treated for
removal of benign tumor. 18 males and 24 females. Their age ranged from 5
to 64 years. The laser that we are using is Surgilase 150XJ CO2 laser system in
connection with the flexible FIBERLASE (Sha rplan, NJ, USA). Our endoscopy
instrumentation is a 4 mm 30 angle endoscope (Snoden Pancer, USA). The
dissection can be performed through a video dissection. The basic instrumentation
consists of elevators, nerve hook, retractor and endoscopic scissors. Suction of the
smoke cause by laser evaporization should also be prepared.
Result: After laser in conjunction with endoscopic surgery for the patients in each group,
the follow- up period ranged from 6 months to 2 years and 6months with average
of one year and 7 months. In our retrospective review, the early complications of
these 42 patients are scalp alopecia, scar alopecia, numbness, ecchyrnosis. There
is no hematoma case happened in each group. In the evaluation of the final results,
Conclusion: Pulse CO2 laser in conjunction with endoscopic surgery enable plastic surgeon to
work at a distance through small incisions without bleeding. Visible scares are
reduced and recovery time is diminished.
Key Word: endoscopy, laser, forehead, soft masses INTRODUCTION
The use of the endoscopic techniques in plastic surgery has been a significant turnaround of the
traditional techniques1-3. Such as the treatment of carpal tunnel syndrome4,5, face- lift6,
placement of tissue expander, breast augmentation, abdominoplasty, and removal of benign
tumor. Endoscopic corrugator/procerus laser ablation using the Nd: YAG contact laser has been
reported by Liang in 19927. However, the combination of the laser with laser surgery has
been very slow. We have been using the Nd: YAG laser with endoscope to treat the carpal
tunnel syndrome. In addition, we have been used SurgiPulse CO2 laser combined with
endoscope for breast augmentation. The major advantage of this technique is less bleeding.
For the introduction of this technique at forehead surgery. I would like to focus on the
MATERIAL AND METHODS
Patients
Between January 1996 and January 2003, 42 patients have been treated for removal of benign
tumor. Eighteen males and 24 females. Their age ranged from 5 to 64 years with an average
of 23 years and 2 months. After laser in conjunction with endoscpic surgery for the patients,
the follow-up period ranged from 6 months to 2 years and 6 months with an average of one
Instruments
The laser that we are using is Surgilase 150XJ CO2 laser system with SurgiPulse. In connection
with the flexible FIBERLASER, made of ceramic and metal with a complex waveguide, is
available up to 1 meter long. Our endoscopy instrumentation is made by Snoden Pancer
Endoscopy, a 4 mm 30 angle endoscope. The dissection can be performed through a video
dissection. The basic instrumentation consists of elevators, nerve hook, retractor, and
endoscopic scissors. Suction of the smoke cause by laser evaporization should also be
Surgical Technique
The surgical technique should cover the procedures of markings, anesthesia, creation of
visualization pocket, periosteal release, tumor removal, wound closure, and dressing.
Marking for incision and identifying the supraorbial, supratrochlear neurovascular bundle, and
frontal branch of facial nerve. For the nerve block, 1% xylocaine with 1: 100,000 epinephrine.
For the pediatric patients, general anesthesia is indicated.
The dissection is done under direct endoscopic view in the subperiosteal plane. A visualization
pocket is created for the instrument manipulation. The pocket is created by subgaleal, above
deep temporal fascia, and subperiosteal dissection. Transection of periosteum can be done by
using Surgilase CO2 laser with the power of 8 watts total energy of 250 mj followed by benign
tumor removal. All the specimens were send to the Department of Pathology, Chang Gung
Memorial Hospital, for pathological examination. In some cases, muscular dissection for
reaching the sot tissue mass is necessary. The ablation of the muscle groups after identifying
the neurovascular bundle by nerve hook is indicated for prevention of the complications. The
wound closure can be done primarily after removal of the benign tumor. Then the wound was
In our retrospective review, the pathological finding demonstrated 30 patients with lipomas, 10
patients with inclusion cysts, and 2 patients with dermoid cysts. Excellent results can be
achieved (Fig. A, B, C). The early complications of these 42 patients are listed in Table 1.
There is no hematoma case happened. However, the high incidence of early complications of
forehead numbness may be due to extensive dissection of the pocket with the results of soft
tissue swelling at forehead area. Most of these early complicatuion have been resolved in our
conservative management. In the evaluation of the final results, scar alopecia can be noted
(Table 1). In some critical area such as supraorbital region, we should pay attention to
asymmetry of eyebrow when the tumors are located at brow areas.
DISCUSSION
From an aesthetical point of view, the forehead is the structure that has been more amenable to
endoscopic approach in the face for removal of benign tumor. Identify the supratrochlear,
supraorbital neurovascular bundle and frontal branch of the facial nerve for avoidance of injury
that causes numbness and/or bleeding are important10. Therefore, the indications for this
combined technique are the same as for the endoscopic forehead surgery, and the same
difficulties also arise in these group of patients using the endoscopic approach. Advantages
of the endoscopic surgery includes: decreased scarring, less numbness, acceptability, less
bleeding, less edema. The main advantage of the endoscopic surgery at forehead area is the
minimization of scars. This is particularly true for the scalp. In our series, the less scar on
patients behind hairline is more acceptable. In addition, there are no significant incision s on
the forehead, there is less bleeding. However, the potential complication of bleeding can be
eliminated by using the laser combined with endoscpic surgery for dissection of tumor or
The laser that we are using is Surgilase 150XJ CO2 laser system. In connection with the
flexible FIBERLASE, made of ceramic and metal with a complex waveguide, is available up
to 1 meter long. As we know, all CO2 lasers suffer the loss of CO2 partial pressure during the
discharge process due to energetic electron collisions causing CO2 disassociation. In this
particular Freespace Direct Current (D.C.) laser system of Surgilase, glass is the most inert
material available for laser construction and lends itself well to D.C. laser design. Gold as a
discharge driven catalyst has allowed a huge leap in performance. At all energy levels, the
width of an individual pulse will never exceed 600 µS which is within the limits of the thermal
relaxation time of tissue, and as the programed energy level is changed the width of each pulse
The FIBERLASER has the property of reshaping the beam profile of the original Gaussian
beam to minimize the beam skirts on tissue. This special design results lower energy pulses
to be effective in char free tissue removal, and achieves in difficult areas to reach.
In some patients, it is significantly difficult to elevate the forehead reliably for endoscopic
approach. This is because of the tight or thick skin in the forehead and the significant bony
attachment s of the frontal/periorbital soft tissues. In these group of patients, the endoscopic
approach will probably not work unless an extended subperiosteal release is made. Like other
new procedure there is a learning curve that must be followed to achieve the optimal technical
expertise, which will yield the best results. This require new training. Completely new
instrumentation is required. In addition, it is necessary to determine the limitation of this
technique and when to combine the endoscopic technique with laser surgery.
CONCLUSION
SurgiPulse CO2 laser in conjunction with endoscopic surgery enable plastic surgeon to work at
a distance through small incisions without bleeding. Visible scares are reduced and recovery
time is diminished. Limitations for the tight skin and forehead irregularity are still existed.
Comparison of different lasers and parameters for expanding to what we can do should be our
REFERENCES
Carson WG: Arthrosocopy of the Shoulder, Anatomy and Technique. A review paper.
Grimes D: Frontiers of the Operative Laparoscopy: A Review and Critique of the
Evidence. Am J Obstet Gynecol 166: 1062,1992.
Gadacz TR: U.S. Experience with Laparoscopic Cholecystectomy: Am J Surg 165:450,
Chow JC: Endoscopic Release of the Carpal Ligament: A New Technique for Carpal
Okutsu I, Niromiya S, Takatori Y, Ogawa Y: Endoscopic Management of the Carpal
Tunnel Syndrome: Arthroscopy 5:11, 1989.
Core GB, Vasconez, LO, Askren C, Yamamoto Y, Gamboa M: Coronal Face-Lift with
Endoscopic Techniques: Plast Surg Forum XV: 227. 1992
Liang M, Narayanan K: Endosxopic Ablation of the Frontalis and Corrugator Muscles – A
clinical Study: Plast Surg Forum XV: 54, 1992
Ramirez OM, Oneal R: First International Workshop on Facial Rejuvenation: The
sub-periosteal and other deep plane techniques. Baltimore, Maryiand, April, 1992.
Isse NG: Endoforehead Presentation at the Second International Workshop on Facial
Rejuvenation: Subperiosteal, Facelift, Ancillary and Alternative Techniques. Baltimore,
10. Hamas RS: Endoscopic Corrugator-Procerus Muscle Resection. Presentation at the 26th
Annual Meeting of the American Society, Boston, Massachusetts, April 1993.
11. Ramirez OM: The Subperiosteal Rhytidectomy: The Third Generation Face Lift: Am Plast
12. Aiache A: Presentation at the Endoscopic Plastic Surgery Educational Seminar, New Port
13. Ramirez OM: Presintation at the Endoscopic Plastic Surgery Educational Seminar, New
14. McKinney P, Mossie RD, Zwkowski ML: Criteria for the Forehead Lift: Aesth Plast Surg,
15. Ramirez PM, Fuente del Campo A: Subperiosteal Brow and Face Lift PSEF Instructional
Coures, Vol VI, Mosby Yearbook, in print.
16. Giampapa V: Neck Recountouring : Suture Suspension Technique. Presented at the 26th
Annual Meeting of the American Society, Boston, Massachusetts, April 1993.
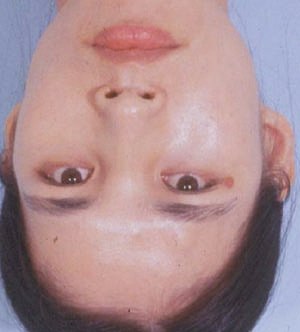
Figure A. Twenty-two-year-old female with a soft tissue mass (lipoma) at forehead area.
Due to cosmetic concerning, endolaser was used.
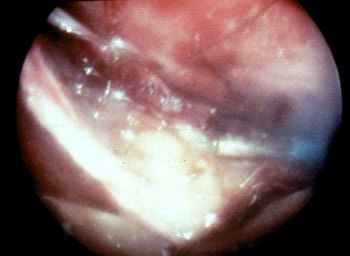
Figure B. The periosteum was ablated by sugilase followed with dissection and removal of
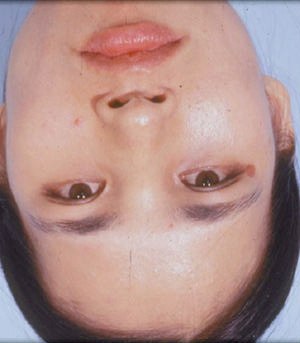
Figure C. Follow- up 12 months after endolaser surgery.
Table 1 Complications of the Endolaser Forehead Surgery for Benign Soft Tissue Tumors in 42
Newsletter April 2012 Ihnen allen muntere und gesunde Osterfeiertage. Ihre Rita Schulz-Hillenbrand Fachanwältin für Medizinrecht Arzthaftungsrecht 1.) Darlegungs- und Beweislast für die Kausalität der Pflichtverletzung durch Unterlassen Besteht die Pflichtverletzung in einer Unterlassung, ist diese für den Schaden nur dann kausal, wenn pflichtgemäßes Handeln den Eintritt des Scha
Valley Bible Church – Sermon Transcript The Cleansing of the Temple John 2:14-17 On June 23, 2003, the NPR radio show "fresh air with Terry Gross" interviewed Dr. Samuel Barondes the author of a new book, Better than Prozac: Creating the Next Generation of Psychiatric Drugs. The book traces the history and analyzes the effectiveness of the current crop of antidepressants