A Comprehensive Team Approach to the Management ofIntroduction. The treatment of children with Prader-Willi syndrome Prader-Willi syndrome (PWS) is (PWS) represents a new challenge in the field of pediatric endocrinology.characterized by infantile hypotonia; The handicaps and problems of affected children are manifold, more so
short stature; small hands and feet; increased
than in any other typical disease of pediatric endocrinology, perhaps withthe exception of craniopharyngioma. Therefore, management of children
decreased muscle mass; scoliosis; reduced
with PWS may be most successful with a team approach to comprehen-
resting energy expenditure (REE); reduced
bone mineral density (BMD), which may leadto osteopenia and osteoporosis; hypogo-
We thank Pharmacia Corporation for organizing a workshop on such an
nadism; hypothalamic dysfunction; and a par-
approach in St. Julians, Malta, on April 24, 2001. This newsletter sum-
ticular facial appearance. These clinical fea-
marizes the proceedings of that workshop. The reader will notice that the
tures are accompanied by hyperphagia, cogni-
development of a comprehensive professional team approach to PWS has
tive disabilities, and behavioral problems,
only just begun. Much work remains to be done, primarily to define what,
including skin picking. In 70% of individuals,
exactly, a “comprehensive team approach” to PWS means. For example,
the syndrome is the phenotypic expression of a
it appears necessary for one highly experienced specialist team member
complex genetic disorder resulting from a
to assume leadership, to allow patients and their families to interact with
paternally derived de novo deletion of the prox-imal long arm of chromosome 15 (at bands
one single professional. Further, growth hormone treatment has becomea very important tool in the management of PWS. Nevertheless, it must
15s from the mother) is seen in about 25% of
be emphasized that without a comprehensive team approach, especiallyto restrict caloric intake and provide psychosocial support for families,
imprinting defect in the rest.1 Prader-Willi syn-
children receiving growth hormone therapy will not lose weight, and the
drome and its sister syndrome, Angelman syn-
impact on their quality of life may remain relatively small.
drome (an entirely different clinical syndrome),were the first examples in humans of genetic
Some centers have a great deal of experience and know-how in managing
imprinting, or the differential expression of
PWS. This know-how, however, is most often attributable to the experi-
genetic information depending on the parent
ence of a single person. Through intensive study of the experience and
of origin. Prader-Willi syndrome is one of the
strategies of such centers and individuals, a professional comprehensive
most common conditions seen in genetics clin-
team approach can be developed that will allow centers all over the
ics worldwide and the most common genetic
world to offer optimum care to their patients with PWS.
cause of marked obesity yet identified,2 and its
various clinical manifestations are major caus-
es of morbidity and social limitations. Learning
Meeting Participants Panelists Moderator Presenters Sponsored by the International Prader-Willi Syndrome Organization through an unrestricted educational grant provided by
A Comprehensive Team Approach to the Management of
only in conjunction with a multidiscipli-
family dynamics, in addition to cognition
and behavior, may all be adversely affect-
studied extensively in the United States,
experience and to identify strategies for
American Experience
to respond to at least two of the stimuli,
individuals with PWS require a variety of
cologic stimuli appeared to be related to
reported for the first time that GH thera-
py led to significant increases in the lin-
ear growth rate of patients with PWS.6 All
the patients in their study initially had
and family interaction, support, and care.
composition, strength and agility, respira-
observed in these cases were not an arti-
nator, a geneticist, a psychologist, and a
ise that the poor linear growth in patients
dietitian. This newsletter describes such
at baseline.7 Thirty-five children received
GH EFFECTS ON PHYSICAL PARAMETERS IN PWS
ed the results of an uncontrolled trial of
increased height velocity (Figure 1),
cipal cause of short stature in the major-
abnormalities.14 All 12 children initially
had low serum levels of GH, IGF-1, there was no significant increase in REE.
therapy. Dual-energy x-ray absorptiometry
value in improving some physical disabil-
(DEXA) at baseline revealed increased fat
ities experienced by children with PWS.
Within 3 months of the patients’ begin-
regulation may contribute not only to the
excess of body fat and the deficit of lean
of fat mass from the trunk to the thighs.
improved behavior and appetite control.
promotes growth of lean body mass,7,8,11,12
Evaluation Growth (cm/yr)
• Complete examination• Dietary evaluation and counseling• Physical therapy evaluation
Figure 1. Height velocity in patients with PWS treated with growth hormone (GH). Thirty-five
children received GH at a dose of 1 mg/m2/day for 24 months and 19 were untreated. After 12 months,
the GH-treated children showed significantly increased height velocity. The growth rate slowed
• Initial discussion of growth hormone
between 12 and 24 months, although height velocity remained significantly higher than at baseline
(*P<0.01 compared with baseline [0 months]). (Reproduced with permission from Carrel AL, Myers SE,Whitman BY, Allen DB. Prader-Willi syndrome: the effect of growth hormone on childhood body compo-
sition. Endocrinologist. 2000;10(suppl 1):43S-49S.)
• DNA studies • IGFBP-3, IGF-1, thyroid panel, lipid
social services, and educational services,
and agility.8 Height velocity remained sig-
as well as readily available facilities for
(P<0.01), although the growth rate
physiology. The Table lists the compo-
nents of the initial evaluation and test-
should be started early; GH therapy start-
considered for them on the basis of clin-
DEXA=dual-energy x-ray absorptiometry; IGF-1=insulin-like
Swiss Experience
growth factor-1; IGFBP-3= IGF binding protein-3.
py in infants. (In the United States, clin-
ical trials of GH therapy in infants with
ture remain the basic defects in PWS.
stabilize their weight for height. Such a
reduction of food intake is possible only
activity, which is probably caused by the
through close, strict parental supervision,
During the first year of the study, no sig-
nificant difference in scoliosis progres-
muscle mass, in turn, is the cause of the
group (from a mean of 9.2° at baseline to
efit of GH therapy for children with PWS,
12.1°) and the control group (from 14.7°
quent increase in REE. If energy intake is
the GH-treated group also was not signif-
not increased, these alterations lead to a
ed and treated in a multidisciplinary clin-
notype (Figure 2). However, even though
tal overweight children. All were treated
cialist, geneticist, psychologist, and die-
titian. Ancillary resources should include
A Comprehensive Team Approach to the Management of
satiety but increases the energy expendi-
had become not only taller but also slim-
was rather limited. The investigators con-
only if energy intake is not increased at
the same time. It is therefore imperative
that parents continue to keep patients’
and height predictions reach the parental
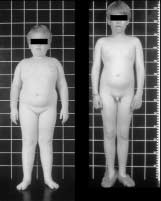
Figure 2. A child with PWS before and 12 months after treatment with growth hormone (GH). For GH therapy to increase lean body mass,
reduce body fat, and stabilize weight for height,
children with PWS must maintain their energy
intake at about 75% that of healthy children.
older children (group 3) was considerable
leagues used the Griffith test19 to study
(Figure 3). The influence of exogenous
the first year of GH treatment.20 At base-
line, the children were significantly more
retarded on the “locomotor” and “hear-
addition, the increase in fasting insulin
ing and speech” scales than on the other
sient.22 Three years of GH therapy did not
er than untreated children with PWS.
served, the investigators speculated that
sition during GH therapy result from sev-
eral therapeutic interventions. It is criti-
cal to maintain control of nutrient intake
of the parents—the most important ther-
apeutic effect of GH.21 After 1 year of GH
certain aspects of lipid metabolism differ
still correlated with abdominal obesity),
formance leads to an increase in activity,
decreased.23 These lipid levels normalize
for the first time that insulin secretion in
Lean mass SDS for height SDS for height 1
olism, as described in adult patients with
Swedish Experience Duration of GH therapy (mo)
deficiency seen in the syndrome was aresult of the characteristic obesity, and
Figure 3. Body composition measured by DEXA in 16 children with PWS. Body composition is expressed
as the height-related standard deviation score and compared with reference values for a Dutch population
older than 4 years or taller than 100 cm.16 The graphs show medians ( , thick black lines) and individual
courses of young underweight (n=4; ■, blue lines), prepubertal overweight (n=8; ■, blue lines), and puber-
tal children with PWS (n=4; ●, dotted lines) treated with growth hormone (GH). Significant differences vs
baseline at 6, 24, and 42 months (*P<0.05, **P<0.01 [Wilcoxon test]). (Reproduced with permission from
Eiholzer U, Bachmann S, l’Allemand D. Is there growth hormone deficiency in Prader-Willi syndrome? Six
arguments to support the presence of hypothalamic growth hormone deficiency in Prader-Willi Syndrome. Horm Res. 2000;53(suppl 3):44-52.)
inary results of this study in 199725 and5-year results in 1999.10
CLINICAL MANAGEMENT OF PWS-ASSOCIATED BEHAVIORS
patients with PWS between the ages of months, height velocity declined dramat-
3 and 7 years were randomized into ically in both groups; height SDS fol-
role in regulating appetite, sensitivity to
group A (n=15), which received GH lowed a similar pattern. Growth hormone
the second year. After 2 years, all chil-
prove that the effects of GH therapy were
again increased (Figure 4). Body mass
low levels of insulin. During the first year
of the study, IGF-1 levels increased rap-
children, levels of fasting insulin, glu-
unchanged in group B (no treatment).
cooperative.26 By adolescence, behavioral
first year of GH therapy in group A, fol-
the second year. In group B, height veloc-
ity SDS decreased slightly during the first
A Comprehensive Team Approach to the Management of
sive, manipulative, irritable, mood-labile,
age, appears to affect the entire brain.
frustrated. Transitioning from one activity
to another becomes increasingly difficult,
ioral manifestations reflect a distributed
includes an inability to recognize cause-
izing this disorder, and the food behavior
four cognitive difficulties have been iden-
ent approach to traditional behavior man-
link punishment or reward with anantecedent behavior. Many patients withPWS who frequently exhibit problem
instituted. These changes require creativ-
ity, hard work, and, often, many monthsbefore a behavior is altered, and some
unalterable. It is particularly difficult
Height SDS Height SDS Time from start of study (yr) Time from start of study (yr)
level of conflict over child rearing. Although this is also true for normal chil-
Figure 4. Height velocity standard deviation scores (SDS) in patients with PWS treated with different regimens of growth hormone (GH) over 30 months. Group A received GH at a dose of 0.1 IU/kg/day
flexibility seen in normal children.
(0.033 mg/kg/day) for 2 years. Group B was untreated for the first year and then received GH at a dose of
0.2 IU/kg/day (0.066 mg/kg/day) during the second year. After 2 years, all children stopped GH therapy for 6
months and then restarted GH therapy at a dose of 0.1 IU/kg/day (0.033 mg/kg/day). Values are means ± SD.
(*P<0.001 compared with baseline; †P<0.03 compared with baseline.) (Reproduced with permission from
Lindgren AC, Ritzén EM. Five years of growth hormone treatment in children with Prader-Willi syndrome. The
Swedish National Growth Hormone Advisory Group. Acta Paediatr Suppl. 1999;433:109-111.
at behavioral management, and pharma-cologic interventions are often consid-
mately are responsible for the inability of
deficits,27 and failure to develop the abil-
adults with PWS to succeed in alternative
living and work placements. Interestingly,
iors in these individuals. A survey of par-
scores in the 90s or somewhat higher.
judgment, denial of deficits, inability to
Functional aptitude, however, is entirely
conflicts, are also seen in patients with
Psychotropic medication shouldbe used only
From the standpoint of diet, two distinct
phases of PWS are apparent: initial fail-
nizes that the constant feeling of hunger
2 months to meet energy requirements.
almost every available psychotropic agent
Signs of poor feeding in infants with PWS
behavioral difficulties and refractoriness
rence of targeted symptoms; only three—
tion, respiratory infections, irritability
tine—were effective.30 More recently, it
has been found that all serotonin-specif-
deterioration is, in fact, a positive out-
marked reduction in irritability, and less
perseveration, but with no specific anti-
and less perseveration.26,32 In addition,
transition to solid food, with 42% of chil-
therapy also produced positive effects on
drug to achieve a benefit; increasing the
6 months of patients’ starting treatment.
engage in food seeking and food stealing.
dose to “normal” often results in toxicity
and a return of the problem behavior.31 In
eating drive that results from their dis-
patients’ social interaction. Furthermore,
have attempted to control their children’s
and environmental changes, have failed.
weight, but dietary compliance is poor.
Severe caloric restriction for short peri-
of physical activity without parental prod-
fective in controlling food-seeking behav-
hospital setting may be helpful, but most
IMPROVING QUALITY OF LIFE IN PATIENTS WITH PWS: DIET, EXER- CISE, AND LIFESTYLE CHANGES
which are often effective in the so-called
A Comprehensive Team Approach to the Management of
19. Brandt I. Griffiths Entwicklungsskalen zurBeurteilung der Entwicklung in den ersten beiden
1. Butler MG, Thompson T. Prader-Willi syndrome: clini-cal and genetic findings. Endocrinologist 2000;10(suppl
Lebensjahren. Weinheim and Basel: Beltz Verlag; 1983.
20. Eiholzer U, Malich S, l’Allemand D. Does growthhormone therapy improve motor development in infants
tured exercise program. Aerobic exercise,
2. Carrel AL, Myers SE, Whitman BY, Allen DB. Prader-Willi syndrome: the effect of growth hormone on child-
with Prader-Willi syndrome? [letter]. Eur J Pediatr.
hood body composition. Endocrinologist. 2000;10(suppl
21. Eiholzer U, Gisin R, Weinmann C, et al. Treatment
3. Lee PDK. Effects of growth hormone treatment in
with human growth hormone in patients with Prader-
children with Prader-Willi syndrome. Growth Horm IGF
Labhart-Willi syndrome reduces body fat and increases
Res. 2000;10(suppl B):S75-S79.
muscle mass and physical performance. Eur J Pediatr.
4. Eiholzer U, Bachmann S, l’Allemand D. Growth hor-
mone deficiency in Prader-Willi syndrome.
22. L’Allemand D, Schlumpf M, Torresani T, Girard J,
Endocrinologist. 2000;10(suppl 1):50S-56S.
Eiholzer U. Insulin secretion before and under 3 years of
trampoline, dancing, and ball playing.
growth hormone (GH) therapy in Prader-Willi syndrome
5. Eiholzer U, Bachmann S, l’Allemand D. Is there
(PWS) [abstract]. Exp Clin Endokrinol Diabetes. 2000
growth hormone deficiency in Prader-Willi syndrome? Six
arguments to support the presence of hypothalamic
mented certainly include control of food-
growth hormone deficiency in Prader-Willi syndrome.
23. L’Allemand D, Eiholzer U, Schlumpf M, Steinert H,Riesen W. Cardiovascular risk factors improve during 3
Horm Res. 2000;53(suppl 3):44-52.
years of growth hormone therapy in Prader-Willi syn-
6. Lee PDK, Wilson DM, Rountree L, Hintz RL,
drome. Eur J Pediatr. 2000;159:835-842.
Rosenfeld RG. Linear growth response to exogenous
growth hormone in Prader-Willi syndrome. Am J Med
24. Vahl N, Jorgensen JO, Hansen TP, et al. The
favourable effects of growth hormone (GH) substitution
tal controls designed to limit hyperphagia
on hypercholesterolaemia in GH-deficient adults are not
7. Carrel AL, Myers SE, Whitman BY, Allen DB. Growth
associated with concomitant reductions in adiposity. A
hormone improves body composition, fat utilization,
12 month placebo-controlled study. Int J Obes Relat
physical strength and agility, and growth in Prader-Willi
Metab Disord. 1998;22:529-536.
syndrome: a controlled study. J Pediatr. 1999;134:215-
25. Lindgren AC, Hagenäs L, Müller J, et al. Effects of
growth hormone treatment on growth and body composi-
8. Myers SE, Carrel AL, Whitman BY, Allen DB.
tion in Prader-Willi syndrome: a preliminary report. The
Sustained benefit after 2 years of growth hormone on
Swedish National Growth Hormone Advisory Group. Acta
body composition, fat utilization, physical strength and
Paediatr Suppl. 1997;423:60-62.
agility, and growth in Prader-Willi syndrome. J Pediatr.
tions may actually discourage social inte-
26. Whitman BY, Myers S, Carrel A, Allen D. A treat-ment/control group study of growth hormone treatment:
9. Eiholzer U, l’Allemand D. Growth hormone normalises
impact on behavior—a preliminary look. Endocrinologist.
height, prediction of final height and hand length in chil-
dren with Prader-Willi syndrome after 4 years of therapy. SUMMARY AND CONCLUSION
27. Dykens EM, Hodapp RM, Walsh K, Nash LJ. Profiles, correlates, and trajectories of intelligence in
10. Lindgren AC, Ritzén EM. Five years of growth hor-
Prader-Willi syndrome. J Am Acad Child Adolesc
mone treatment in children with Prader-Willi syndrome:
Psychiatry. 1992;31:1125-1130.
Swedish National Growth Hormone Advisory Group. Acta
28. Whitman BY, Greenswag L. The use of psychotropic
Paediatr Suppl. 1999;433:109-111.
medications in persons with Prader-Willi syndrome. In:
11. Lindgren AC, Hagenäs L, Müller J, et al. Growth hor-
Cassidy S, ed. Prader-Willi Syndrome and Other
mone treatment of children with Prader-Willi syndrome
Chromosome 15q Deletion Disorders. Berlin: Springer
Clinical trials confirm that GH treatment
affects linear growth and body composition favourably.
Verlag in cooperation with NATO Scientific Affairs
Acta Paediatr. 1998;87:28-31.
12. Eiholzer U, l’Allemand D, van der Sluis I, Steinert H,
29. Greenswag LR, Whitman BY. Long term follow-up of
Gasser T, Ellis K. Body composition abnormalities in
use of Prozac as a behavioral intervention in 57 persons
children with Prader-Willi syndrome and long-term
with Prader-Willi syndrome. Proceedings: 2nd Prader-
effects of growth hormone therapy. Horm Res.
Willi Syndrome International Scientific Workshop and
13. Parra A, Cervantes C, Schultz RB. Immunoreactive
30. Whitman B, Greenswag L. Psychological issues in
insulin and growth hormone responses in patients with
Prader-Willi syndrome. In: Greenswag L, Alexander R,
Prader-Willi syndrome. J Pediatr. 1973;83:587-593.
eds. Management of Prader-Willi Syndrome. 2nd ed.
14. Lee PD, Hwu K, Henson H, et al. Body composition
New York, N Y: Springer Verlag; 1995:125-141.
studies in Prader-Willi syndrome: effects of growth hor-
31. Whitman B, Greenswag L, Boyt M. The use and
mone therapy. In: Ellis KJ, Eastman JD, eds. Human
impact of psychotropic medications for managing behav-
Body Composition. In Vivo Methods, Models, and
ior in persons with Prader-Willi syndrome. Proceedings
Assessment. New York, NY: Plenum Press; 1993:201-
13th Annual Prader-Willi Association Scientific
Conference. July 22, 1998; Columbus Ohio.
15. Angulo M, Castro-Magana M, Mazur B, Canas JA,
32. Whitman B, Myers S, Carrel A, Allen DB. The behav-
Vitollo PM, Sarrantonio M. Growth hormone secretion
ioral impact of growth hormone treatment for children
and effects of growth hormone therapy on growth velocity
and adolescents with Prader-Willi syndrome: a two year
and weight gain in children with Prader-Willi syndrome. J
controlled study. Pediatrics. In press. Pediatr Endocrinol Metab. 1996;9:393-400.
33. Shaw V, Lawson M. Principles of paediatric dietetics.
16. Boot AM, Bouquet J, de Ridder MA, Krenning EP, de
In: Shaw V, Lawson M, eds. Clinical Paediatric Dietetics,
Muinck Kaizer-Schrama SM. Determinants of body com-
2nd ed. Oxford, UK: Blackwell Science; 2001:Chap 1.
position measured by dual-energy X-ray absorptiometry inDutch children and adolescents. Am J Clin Nutr.
34. Morris M. Feeding the young child with PWS. The
17. Stadler DD. Nutritional management. In: Greenswag
35. Lindgren AC, Barkeling B, Hagg A, et al. Eating
LR, Alexander RC, eds. Management of Prader-Willi
behavior in Prader-Willi syndrome, normal weight, and
Syndrome. New York, NY: Springer-Verlag; 1995:88-
obese control groups. J Pediatr. 2000;137:50-55.
18. Eiholzer U. Prader-Willi Syndrome. Effects of HumanGrowth Hormone Treatment. In: Savage MO, ed. Endocrine Development Series. Vol 3. Basel: Karger;
Programa de conducta empresarial y cumplimiento del reglamento Este documento proporciona información sobre nuestro Código de conducta empresarial. Todos los directores, gerentes y empleados son responsables, individual y colectivamente, de la gestión de nuestras actividades comerciales conforme al Código y a la legislación pertinente. Por ello, le recomendamos que lea este documento con ate
 A Comprehensive Team Approach to the Management of
Introduction. The treatment of children with Prader-Willi syndrome
A Comprehensive Team Approach to the Management of
Introduction. The treatment of children with Prader-Willi syndrome A Comprehensive Team Approach to the Management of
only in conjunction with a multidiscipli-
family dynamics, in addition to cognition
and behavior, may all be adversely affect-
studied extensively in the United States,
experience and to identify strategies for
American Experience
A Comprehensive Team Approach to the Management of
only in conjunction with a multidiscipli-
family dynamics, in addition to cognition
and behavior, may all be adversely affect-
studied extensively in the United States,
experience and to identify strategies for
American Experience 
 A Comprehensive Team Approach to the Management of
satiety but increases the energy expendi-
had become not only taller but also slim-
was rather limited. The investigators con-
only if energy intake is not increased at
the same time. It is therefore imperative
that parents continue to keep patients’
and height predictions reach the parental
Figure 2. A child with PWS before and 12
A Comprehensive Team Approach to the Management of
satiety but increases the energy expendi-
had become not only taller but also slim-
was rather limited. The investigators con-
only if energy intake is not increased at
the same time. It is therefore imperative
that parents continue to keep patients’
and height predictions reach the parental
Figure 2. A child with PWS before and 12 A Comprehensive Team Approach to the Management of
sive, manipulative, irritable, mood-labile,
age, appears to affect the entire brain.
A Comprehensive Team Approach to the Management of
sive, manipulative, irritable, mood-labile,
age, appears to affect the entire brain. A Comprehensive Team Approach to the Management of
19. Brandt I. Griffiths Entwicklungsskalen zurBeurteilung der Entwicklung in den ersten beiden
1. Butler MG, Thompson T. Prader-Willi syndrome: clini-cal and genetic findings. Endocrinologist 2000;10(suppl
Lebensjahren. Weinheim and Basel: Beltz Verlag; 1983.
A Comprehensive Team Approach to the Management of
19. Brandt I. Griffiths Entwicklungsskalen zurBeurteilung der Entwicklung in den ersten beiden
1. Butler MG, Thompson T. Prader-Willi syndrome: clini-cal and genetic findings. Endocrinologist 2000;10(suppl
Lebensjahren. Weinheim and Basel: Beltz Verlag; 1983.