Medical Risks of Infertility
Infertility, next to pregnancy and childbirth, affects
more women of reproductive age than any other condition. Literally millions of women are affected by this condition every year but are
not able to receive adequate medical care because the health insurance industry excludes coverage for “fertility-related services” (to be read:
Infertility is associated with a group of diseases that affect not only
the reproductive status of women but also their very health. An enor-mous amount of insight has been gained into the causes of infertility over the last 20 to 30 years. Infertility is now known to be associated
with diseases that have a substantial health impact on women and, if
these women are left untreated, such diseases lead to a decrease in quality of life and the potential that life may be either impaired or shortened.
Infertility is usually associated with some degree of either organic disease, or hormonal or ovulatory dysfunction. In women, these include
such conditions as endometriosis, ovulation-related disorders, various
hormonal dysfunctions, pelvic adhesive disease, polycystic ovarian disease, various forms of tubal occlusion and anovulation. Male causes of infertility are associated with low sperm counts, and these are associ-
ated with such conditions as chronic prostatitis, hormonal dysfunction,
varicocele (varicose vein of the testicle), and some causes that are not yet known.
In women, one of the main diffi culties with infertility and the
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
organic diseases and hormonal dysfunctions that are associated with it is that these same diseases can also cause both short- and long-term disability,
impairment of one’s quality of life and even potentially the shortening of one’s life. In other words, fertility-related problems in women have a
“two-pronged” effect. They not only affect a woman’s fertility but they
also affect her general health. Because infertility evaluation and treatment
has been excluded by the insurance industry for so many years, literally thousands, if not millions, of women throughout the United States have been denied access to the type of medical care that they deserve for these medical conditions.
Such problems as pelvic pain; dysmenorrhea; dyspareunia; irritable
bowel syndrome; various metabolic effects including increased risk for heart attack, and diabetes; the potential onset of various cancers includ-ing ovarian cancer, endometrial cancer and breast cancer; osteoporosis; and the risks of subsequent pathologic pregnancies and low birth weight infants are all associated with that “two-pronged” effect. It has become irresponsible for a society not to recognize these medical effects and risks exist while denying appropriate third-party reimbursement for their medical care. Endometriosis
Endometriosis is notorious for causing such problems as severe pelvic pain, menstrual cramps, and pain with intercourse. But it is also
associated with irritable bowel syndrome, hormonal dysfunctions, and a
Endometriosis is treated either surgically or medically, but the
surgical approach is generally better for the relief of pain and for future
fertility purposes. However, surgical procedures must be done expertly in such a fashion so as to prevent adhesions (or scar tissue) from forming
as a result of the surgical procedure itself. Even with these treatments,
there is some rate of recurrence with the disease. However, long-lasting relief can be anticipated especially with surgical treatment.
It is well known that certain aspects of endometriosis are similar to
those of malignant disease.1 Endometriosis may proliferate and invade other tissues due to a loss of control of growth and proliferation, and the mechanisms underlying this loss may be similar to those seen in cancers.
It has been observed in association with small bowel obstruction,2 the
Internet Appendix 3: Medical Risks of Infertiltiy
involvement of the ureter leading to kidney obstruction and uremia
(kidney failure),3 and other areas of the urinary tract.4-7 The sigmoid
colon has been perforated during pregnancy as a result of endometrio-sis8, and massive ascites can also be associated with endometriosis.9-10
Endometriosis has been observed in the lung,11-12 the sciatic nerve,13
the diaphragm,14 and in the rectal/vaginal area15 along with many other
Hormonal Dysfunctions associated with Infertiltiy
Hormonal dysfunctions are very common in women with infertility
problems. These problems are often associated with the abnormalities that occur in association with infertility relative to the occurrence of ovulation. Abnormal events of ovulation are common in women with infertility and because of this, the hormonal dysfunctions associated
with abnormal ovulations are also common.
In Figure 1, the luteal phase progesterone levels are shown for
women who have infertility from all causes. In patients with endome-
Figure 1: Postovulatory (post-Peak) progesterone profi le in patients with infertility and regular cycles (N=240, dotted line) compared to a control group of women with normal ovulatory func- tion. All levels in the infertility group are signifi cantly lower than in the control group (From: Pope Paul VI Institute research, 2004).
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
triosis, polycystic ovarian disease, pelvic adhesive disease, and distal
and proximal tubal occlusion, the production of progesterone during
the postovulatory phase of the cycle has been shown to be signifi cantly decreased.
Progesterone is very important to the support of pregnancy and it
also modulates or modifi es the immune system. It supports the immune system and, when the progesterone levels are low, the immune system becomes less effective. It is thought that these decreased progesterone
levels are one reason why women with infertility have an increased risk of various types of cancers (see later).
In Figure 2, the androgen levels in women with polycystic ovarian
disease are shown. Testosterone and androstenedione, are specifi cally elevated. In women with polycystic ovaries (PCOD), hirsutism, acne, obesity and hypertension are all associated with these elevated androgen levels. Furthermore, some of the cancers that are associated with long-term, untreated PCOD are associated, at least in part, to the elevated androgen levels (see below). Figure 2: Androgen levels in patients with PCOD compared to a control population without PCOD. Total testosterone, free testosterone and androstenedione levels are all statistically signifi cantly higher and DHEAs levels are higher and approach statistical signifi cance (From: Pope Paul VI Institute research, 2004).
Internet Appendix 3: Medical Risks of Infertiltiy
Pelvic Adhesive Disease
Pelvic adhesions are formed in a variety of different conditions.
Endometriosis, for example, is notorious for causing very thick and
dense pelvic scar tissue. However, pelvic infections such as Chlamydia and gonorrhea also cause such problems.
When a women has pelvic adhesions, it is often associated with
pelvic pain and increases her risk of tubal pregnancy. Pelvic adhesions cause infertility or other reproductive problems by scarring the fallopian tubes and causing tubal blockage. Polycystic Ovarian Disease
In women who have polycystic ovaries, the condition is associated
with long and irregular menstrual cycles. These ovaries do not respond
normally and so these women are chronically anovulatory or oligo-ovulatory. Much of their infertility is due to the fact that they are not ovulating regularly and, of course, treatment is aimed at trying to assist them with this.
Polycystic ovarian disease is often associated with a variety of different
metabolic abnormalities (see later) and the increased risk of endometrial
cancer is signifi cant. These cancers are preventable with adequate evalu-ation and treatment and, more and more, the metabolic abnormalities are also treatable as well. Pelvic Pain, Dysmenorrhea, and Dyspareunia
The long-established associations between endometriosis and pelvic
pain and between endometriosis in general and infertility have been confi rmed.16 The frequency of symptoms in association with women
with endometriosis are identifi ed in Table 1. In a survey conducted by
the Endometriosis Association, 72% of patients had symptoms for six or more years before they eventually obtained adequate evaluation and treatment. Furthermore, 60% of women saw more than three physi-cians and 32% saw fi ve or more physicians. This data suggests that
women with endometriosis continue to experience signifi cant delays in the diagnosis and treatment of this condition and they suffer considerable
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
Table 1: Frequency of Symptoms Associated with Endometriosis1 Frequency
1. Halstead L, Pepping P, Dmowski WP: The Woman with Endometriosis: Ignored, Dismissed and Devalued. The Second International Sympo-sium on Endometriosis. The Endometriosis Association, 1989.
Furthermore, pelvic adhesive disease and chronic pelvic infections,
while associated with infertility, can also be an associated fi nding in
Chronic pelvic pain is associated with endometriosis in 71 to 87%
of cases.19-23 Such pelvic pain and its associated dysmenorrhea can be extremely debilitating but also can be treated quite adequately if the
woman is given access to medical care.24-29
Interestingly enough, women with endometriosis and pelvic pain
who conceive are less likely to experience persistent pelvic pain through-
Gastrointestinal Problems, Irritable Bowel Syndrome
Endometriosis can frequentlyinvolve the intestinal tract (approxi-
mately 25% of cases31). This may involve the sigmoid colon, the rectum, the terminal ileum, cecum or appendix. When such involvement occurs, it can create symptoms of irritable bowel syndrome, partial bowel obstruc-tion,2 and even mimic primary gastrointestinal cancers on x-ray imaging.32
Furthermore, the ovarian steroid hormones (especially progesterone) have
long been thought to have important effects on the motor activity of the gastrointestinal tract and to determine the expression of that activ-ity. Dysfunction of these hormones has been observed in patients with idiopathic functional bowel disease33 and, with the decreased production of progesterone observed in a variety of infertility states, it is easy to
Internet Appendix 3: Medical Risks of Infertiltiy
understand how this could be made worse. In these conditions, the
ability of progesterone to quiet the bowel is less intense, and functional bowel disease may be exacerbated. These symptoms can be debilitating
for women and lead to a signifi cant decrease in their quality of life. Metabolic Effects of PCOD
It has been clearly recognized now that polycystic ovarian syndrome
is associated with major metabolic disturbances which are related to insulin resistance and that same insulin resistance plays a role in the development of the reproductive abnormalities that occur with this disorder. Insulin resistance and elevated low density lipoprotein (LDL cholesterol) levels
are observed in women with PCOD. Furthermore, brothers of women
with PCOD have insulin resistance and elevated DHEAs levels which
suggests that these are genetically related conditions.34-35
Polycystic ovarian disease is a metabolic disorder which affects
multiple organs. Studies have suggested that women who have this
condition are at risk for developing Type II diabetes mellitus, hyperten-sion, dyslipidemia (increased triglycerides, increased cholesterol), and even an increased risk of myocardial infarction.36-38 In addition, women
with pre-existing polycystic ovarian disease have an increased risk for
developing diabetes when they are pregnant.39 The impairment of glucose tolerance in normal women and women with polycystic ovarian disease is identifi ed in Table 2. Chronic fatigue syndrome is also observed
more frequently in women who have polycystic ovaries.40
Table 2: Incidence of Glucose Tolerance in Normal Women and Women with PCOD1 Normal Control Polycystic
Dunaif A and Thomas A: Current Concepts in Polycystic Ovary Syn-drome. Annu Rev Med 52: 401-419, 2001.
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
PCOD, Dysfunctional Bleeding, and Hirsutism
Additional symptoms associated with PCOD include dysfunctional
uterine bleeding. This dysfunctional bleeding is associated with the prolonged absence of ovulation and the chronic stimulation of the endo-metrium with estrogen which is unopposed by progesterone. Because of the unopposed estrogen stimulation of the endometrium, the endometrium breaks down and the woman experiences chronic bleeding, which is not
a true menstrual period. This is truly an endocrine disorder, but it does
need to be properly evaluated and treated.41
Excessive hair growth on the chin, upper lip, sideburns, chest,
abdomen and upper thighs is also a common condition associated with
PCOD. This is usually thought to be associated with the increased
androgens (male hormones) that are associated with this condition
(Figure 2). Such hirsutism can be disfi guring and very problematic
decreasing the quality of life for these women. Without proper medical evaluation and treatment this condition can go on unabated. However, it does respond fairly well to medical treatment.42-45
Infertility and Cancer
It is clear that some forms of infertility are associated with the
development of certain types of cancers. In some cases, this connection is well established while in other cases it is more speculative. Nonethe-less, there are certain types of cancers that are clearly associated with problems related to infertility. This is particularly true for ovarian cancer, endometrial cancer and breast cancer.
With regard to endometriosis, the Endometriosis Association
recently conducted a survey that showed an elevated risk for breast cancer, ovarian cancer, non-Hodgkin’s lymphoma and melanoma in
women with endometriosis. In addition to this, the study indicated
elevated risks for these cancers in the families of women with endo-
metriosis.46 Furthermore, the risk of ovarian cancer, breast cancer, and non-Hodgkin’s Lymphoma have been shown to be increased by others47 in patients with endometriosis. A. Ovarian Cancer
Because ovarian endometriosis may play a role in the pathogenesis
Internet Appendix 3: Medical Risks of Infertiltiy
of some ovarian cancers, it has been recently suggested that ovarian endometriosis should be recognized as a precancerous condition and strictly followed up.48 Nulliparity and infertility are both associated
with an increased risk of developing ovarian cancer with these women
nearly three times more likely to develop ovarian tumors compared to women who have been pregnant.49 Malignant transformation of
endometriosis is a well documented process especially with regard to ovarian endometriosis.50-52
It has been suggested that genetic factors contribute both to the
development of endometriosis and also to ovarian cancer and that there
may be some common linkages53 to that genetic inheritance. It has also
been suggested that infertility and endometriosis may be independent risk factors for ovarian cancer and that both, therefore, should be taken into consideration as risk factors.54 In any regard, the linkage between infertility, endometriosis and ovarian cancer is strong and has been well documented in the medical literature.55-65
B. Endometrial Cancer
An increased risk for endometrial cancer has been found among
a variety of subgroups of infertile women. It is suggested that chronic anovulation is primarily responsible for this linkage.66 In anovulation,
the endometrium is exposed to chronic estrogen stimulation unopposed by progesterone. Progesterone is normally produced following ovulation. In the absence of ovulation, of course, progesterone is no longer produced.
Thus, this presents a situation where there are relatively high estrogen
and low or absent progesterone and this is clearly associated with an
increased risk of endometrial cancer.67-68
The most commonly cited pre-existing linkage with endometrial
cancer is polycystic ovarian disease because it is often associated with long and irregular menstrual cycles and prolonged periods of anovulation.
This situation sets itself up for prolonged exposure of the endometrium
with estrogen and a situation that is progesterone defi cient.69-71 With proper evaluation and treatment—with the use of exogenous progesterone therapy—the incidence of endometrial cancer can be signifi cantly reduced. However, women must have exposure to medical care in order for this
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
C. Breast Cancer
Over the past 20 years, the overall incidence of breast cancer has
increased (see Figure 39-3). Furthermore, one of the clear risk factors for the development of breast cancer is delayed onset of the fi rst pregnancy.72
It has been long recognized that progesterone defi ciency states have been
associated with an increased risk of breast cancer particularly of the
Furthermore, it has been shown that women who have elevated
androgen levels and decreased progesterone levels also have increased
risks of breast cancer.75-79 While the relationship of the factors remains controversial, the risk factor of delayed onset of pregnancy (which is common in infertility patients) is incontrovertible. Considering also that these are patients who often have signifi cantly decreased luteal phase progesterone production and in some cases elevated androgen levels (Figure 2), this is something that needs to be further discussed
Figure 3: This shows the increasing rates of stage I breast cancer. The diagnosis of stage I breast cancer has increased 113% between 1983 and 1997 (data is from the Surveillance, Epidemiology and End Results—SEER—Program of the National Cancer Institute72).
Internet Appendix 3: Medical Risks of Infertiltiy
Osteoporosis
In patients with hypothalamic amenorrhea, the infertility is due
to the lack of ovulation. The reason the woman does not ovulate is because the hypothalamusoperates dysfunctionally and the pituitary does not respond with the needed cyclic gonadotropin production. In
such conditions, without ovulation occurring, the woman is exposed
to chronic low levels of estrogen and the complete absence of progesterone.
In such circumstances, the woman is signifi cantly at increased risk for
In addition, because women with regular menstrual cycles who
have infertility also have decreased progesterone production by their ovaries, there is the likelihood that they may be at increased risk for osteoporosis in the long term as well. In fact, there is evidence to suggest that progesterone is a bone-building hormone and that postmenopausal osteoporosis may be, at least in part, a progesterone defi ciency disease
which is exacerbated in women who have a prolonged chronic defi ciency
of progesterone during their reproductive years.82
Immune Defi ciency and Infertility
It has been thought for a number of years that endometriosis may
be associated with some type of alteration in cell-mediated immunity.83
In fact, endometriosis fulfi lls all the classic characteristics of an autoim- mune disease—polyclonal B cell activation, tissue damage, multi-organ involvement, female preponderance, familial occurrence, and increased
concurrence with other autoimmune diseases.84
In women with endometriosis, there is a defect in natural killer cell
activity, and the natural killer cell activity of the peritoneal fl uid mono-
nuclear cells is decreased in endometriosis. This correlates signifi cantly
with the severity of the disease in both the peripheral blood and the
peritoneal fl uid of women with endometriosis.85,86
Substantial evidence indicates that endometriosis shares many
similarities with autoimmune diseases. The theory of an altered immune system and endometriosis suggests that changes in cell-mediated im-
munity and/or humoral immunity may contribute to the development of the disease. Many investigators now are looking at immunomodulaters
and infl ammatory modulators as possible innovative treatments for endometriosis.87-89
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
Salpingitis Isthmica Nodosa and Ectopic Pregnancy Salpingitis isthmica nodosa (SIN) is a condition which usually
affects the portion of the fallopian tube that immediately enters the
uterus. The proximal fallopian tube that is involved with this condi-tion results in either complete or partial blockage of that fallopian tube.
Most commonly, the blockage of the fallopian tube is partial. Because
the blockage is only partial, it disturbs the normal transmission of the fertilized ovum down the fallopian tube and into the uterus. Because of this abnormality, the blastocyst or early embryo may get caught in the fallopian tube resulting in an ectopic pregnancy. Such a pregnancy is dangerous for the woman because the fallopian tube can rupture unexpectedly and cause uncontrollable hemorrhage. It may require
Infertility and Subsequent Pregnancy Complications
Women suffering from infertility who then achieve a pregnancy are
also at increased risk for subsequent pregnancy-related complications.
For example, it has been known for a long time that the incidence of
spontaneous abortion, ectopic pregnancy, intrauterine growth retarda-
tion, and stillbirth are all increased in a subsequent pregnancy following infertility.94-105 The above risks occur in women who have pre-existing
endometriosis but also occur in women with hyperprolactinemia.100
In women who have polycystic ovarian disease, the incidence of
gestational diabetes and pregnancy-induced hypertension is increased signifi cantly.106-107 In fact, even the pre-existing diagnosis of infertility
will increase the risk of pregnancy-induced hypertension in a subsequent
It has also been known that a pre-existing history of infertility is
a risk factor when it comes to preterm delivery. Babies born to moth-ers who have previous infertility have a signifi cantly increased risk of
having a low birth weight infant due either to premature delivery or to intrauterine growth restriction.108-110
As a result of these medical fi ndings, pregnancies that occur in
women who have pre-existing infertility are more commonly high risk
and demand to be followed more carefully and with more focused
medical intervention. With pre-existing knowledge of the cause of the
Internet Appendix 3: Medical Risks of Infertiltiy
underlying infertility factor, a more specifi c form of intervention can be made. General Medical Problems
There are also a number of other general medical problems that
occur more commonly in women who have infertility. For example,
women with endometriosis have been shown to have heavier menstrual fl ow and signifi cantly higher abnormal menstrual scores than those who do not have the disease.111 Thyroid disease is often associated with
fertility problems of one type or another. Various types of subfertility is associated with both hyper- and hypothyroidism.112-113 Thus, these patients require a complete evaluation of thyroid function as a part of their evaluation for infertility.
In women who have hypothalamic amenorrhea, it has been shown
that certain psychosocial stressors may be associated with this condi-tion.114 These women often report more depressive symptoms and dysfunctional attitudes than other women and also an increased risk of disordered eating patterns. With these types of problems, psychological intervention and support may be necessary.114
Socioeconomic and Health Costs of Infertility Care
It has been shown that most women with impaired fertility do not
obtain infertility services.115 This means that the underlying medical risks of their infertility problem are not being evaluated or subsequently treated. It also means that a large number of women are not being evalu-ated or subsequently treated. It also means that many women are being signifi cantly underserved when it comes to their basic health needs.
Standard insurance plans generally have language that excludes
coverage for “an expense or charge for the diagnosis or treatment of fertility or infertility or promotion of fertility including (but not limited to): (1) fertility tests and procedures; (2) reversal of surgical sterilization and (3) any attempts to cause pregnancy …”. This language has led to signifi cant problems in this area of medicine for physicians, hospitals and patients. These problems include but are not limited to the following:
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
1. The language is extremely vague and leads to an inability on the
part of the physician or the patient to reasonably interpret the provision. This leads to a very uneven and unfair administration of the provision.
2. An example of this would be that many “fertility-related” pro-
cedures are, in fact, often paid for by insurance coverage and are not excluded by these provisions. These include such things as surgical sterilization, various methods of contraception, and abortion procedures. If, in fact, an insurance program excludes contraceptive coverage, the plan will often subsidize the use of birth control pills for the treatment of various women’s health problems even though those pills are technically “fertility related.”
3. Patients complain that the administration of this provision is
often irrational. For example, insurance may cover a particular surgical procedure for the treatment of a particular disease, but it
will not pay for the diagnostic laparoscopy which is necessary for
the physician to adequately and accurately diagnose it and thus prescribe the proper surgical procedure.
4. This exclusion is often dependent upon the review of the claims
person in charge of reviewing the particular claim at the insurance company. It is often open to their interpretation even though they
are not medically qualifi ed to assess the medical aspects of the situation, and experience has shown that the actual application of the provision is extremely uneven. The claims review person
is usually not medically trained and not prepared to deal with all of the variations of evaluation and treatment that might exist for the condition. The same is often also true for those physicians
employed by the insurance industry for review of these claims.
They are often not up-to-date with current capabilities of diagnosis
5. Medical problems associated with male infertility are often covered
without any questions asked. For example, antibiotics for the
treatment of prostatitis which will improve fertility; a surgical procedure for the repair of a varicocele which also may improve
Internet Appendix 3: Medical Risks of Infertiltiy
male fertility; testicular biopsies which will assist in the diagnosis
of various male diseases that may be associated with infertility and, of course, the use of Viagra for male impotence which
may improve a male’s fertility by correcting impotence are often,
without question, reimbursed by the insurance industry. This
clearly opens up the problem of gender-specifi c discrimination
where the exclusionary causes, which most often affect women,
6. It has been known, in addition, that nuns, who may have hormone
problems associated with their menstrual cycles, are at times denied coverage because of it being “fertility related” when it is quite obvious that the medical evaluation and treatment has nothing to do with fertility.
7. In addition, patients who have premenstrual syndrome, which
is also often observed in women who have infertility, are often denied coverage for both the evaluation and treatment of their condition because it is tagged as “fertility related” when, in fact, it is not at all fertility related in these cases. The same is true for
various hormone-related causes of abnormal bleeding.
8. As a result, this has led to a very contentious and confrontational
relationship between women and their insurance companies when it comes to issues related to the reproductive system. It is not uncommon for these couples to hire attorneys to represent them in their negotiations with their insurance companies, to constantly be on the telephone with their insurance plan trying to straighten out the claim’s process and to often enter into very contentious
appeals hearings which are stressful and quite unbecoming the
premium paid to the insurance company for health coverage.
9. Finally, some physicians have been targeted by the insurance
industry in retaliation for some of the contentiousness.
The current use of “exclusion of coverage” clauses by the insurance
industry for “fertility-related services” is very problematic and needs to be remedied. Furthermore, it is out of date with our modern knowledge
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
of the underlying diseases that actually cause fertility-related problems.
It has been argued that managed care organizations should take
the lead in providing infertile couples with an organized, humanistic
approach that is mindful of the attending social and health issues.116 In
this way, care for infertility and its attendant health risks can be made more accessible and comprehensive.
In a recent study of the costs of an infertility evaluation and treat-
ment, infertility costs accounted for only a small fraction of the total health care costs of the plan. Furthermore, the addition of infertility
specifi c evaluation and treatment programs could be obtained for a
nominal monthly fee. This was estimated to be an additional member per month health care cost of $0.67.117 Summary and General Conclusions Infertility is the inability of a woman to achieve a pregnancy over a period of one year of unrestricted intercourse. In reality, it is only a symptom of underlying disease. While many years ago infertility was thought to
be “all in your head,” work that has been done over the past 30 years has shown that the inability to achieve pregnancy is the result of a
multi-factorial combination of organic, hormonal and immunological
The current approach of insurance plans to exclude coverage for
“fertility-related services” does not recognize this change in the under-
standing of the underlying problems of infertility. It still appears to observe infertility as more of a psychological problem than a medical one. In fact, next to pregnancy and childbirth, it is the most common medical problem affecting reproductive age women. And yet, because of excluded coverage, the insurance industry has specifi cally targeted this group of women with poor medical care.
There are many issues that are involved in this current problem.
The primary issue, however, should be the question of whether or not
women should be given the right to have reproductive health care
specifi c to their gender. While a U.S. District Court in Chicago ruled
that infertility fi t the defi nition of a disability and was therefore subject to the antidiscrimination enforcement under the Americans with Dis-
ability Act,116 this approach ultimately denies the fundamental issue that
this is a health care issue encountered by women. It is not only a health
Internet Appendix 3: Medical Risks of Infertiltiy
care issue specifi c to their immediate health but also, and perhaps most importantly, their long-term health.
It is quite possible that the current procedures followed by the
insurance industry of excluding infertility coverage from the standard health care plans of women discriminate against women mostly on a
gender basis. In fact, from actual practice, it is clear that this exclusion specifi cally targets women because similar conditions which have a
two-pronged effect of affecting one’s fertility and also one’s health that involve men are not subject to similar discrimination.
It should also be pointed out that many of the very same tests,
procedures and treatments that are used to diagnose and treat these conditions from an infertility perspective are also used to diagnose and treat these diseases from a purely women’s health perspective. Diagnostic tools include laparoscopy, ultrasound assessment, testing of various hormones, testing for blockages in the fallopian tubes, various types of biopsies, and seminal fl uid analysis in men. Treatment procedures that treat the underlying diseases include various surgical procedures, hormonal therapies, programs that treat ovulatory dysfunction, and
Therefore, it seems that legislatures must understand the reality of
the underlying diseases and medical risks that infertility poses. These
women often suffer from severe pelvic pain, dysmenorrhea and dyspa-
reunia. They may have gastrointestinal abnormalities and irritable bowel
syndrome. They may have severe hormonal defi ciencies, which result in
formation of cancers such as ovarian cancer and endometrial cancer in
women who have pre-existing infertility. Furthermore, the risk of breast
cancer is defi nitely increased in those women who have had prolonged episodes of infertility.
Other health risks include the growing knowledge that there are
similarities between certain types of infertility and some of the autoim-
mune disorders such as thyroiditis, systemic lupus, and rheumatoid
arthritis. Furthermore, women who have prolonged anovulation are at
increased risk for osteoporosis which can be a debilitating disease not only in younger women but most importantly as those women age.
Perhaps one of the most hidden of all of the factors relative to the
infertility medical crisis is the issue of what happens to these women
when they become pregnant. The evidence that shows that the preg-
nancies are at increased risk once the woman becomes pregnant after a
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
pre-existing infertility problem is overwhelming. With better medical knowledge and understanding of the basic underlying problem of the infertility that exists—whether that be organic or hormonal or immune
stimulated—the physician is in a better position to adequately treat
that pregnancy and reduce the types of problems associated with those pregnancies. Taking simply one example, the example of prematurity,
with medical intervention, the prematurity rate can be expected to be
decreased if the physician has a better understanding of the underlying causes. The cost for the delivery of a premature infant to that infant as
well as to the insurance industry and to society in general, is exorbitant.
Any headway that can be made in the reduction of those premature
births and the improvement of the outcomes of those infants can only benefi t the health insurance industry and society in general not to speak at all of the individual baby and their families (which ultimately are the
Finally, this can all be done at a relatively low cost. It has been shown
that if the standard exclusion is removed and infertility is covered by the
standard health insurance plan, the actual per member cost is extremely
low. Currently, it is estimated at being less than $1.00 per month.
Internet Appendix 3: Medical Risks of Infertiltiy
References
1. Thomas EJ, Campbell, IG: Evidence that Endometriosis Behaves in a
Malignant Manner. Gynecol Obstet Invest 50 (Suppl 1): 2-10, 2000.
2. Dmowski WP, Rana N, Jafari N: Post Laparoscopic Small Bowel Obstruction
Secondary to Unrecognized Nodular Endometriosis of the Terminal Ileum.
J Am Assoc Gynecol Laparosc 8: 161-166, 2001.
3. Henkel A, Christensen B, Schinler AE: Endometriosis: A Clinically Malignant
Disease. Euro J Obstet Gynecol Repro Bio 82: 209-211, 1999.
4. Nezhat C, Nezhat F, Nezhat C, Nasserbakht F, Rosati M, Seidman DS: Urinary
Tract Endometriosis Treated by Laparoscopy. Fertil Steril 66: 920-924, 1996.
5. Zanetta G, Web MJ and Segura GW: Ureteral Endometriosis Diagnosed at
Ureteroscopy. Obstet Gynecol 91: 857-859, 1998.
6. Nackley AC, Jeko TR: Ureteral Displacement Associated with Pelvic Peritoneal
Defects and Endometriosis. J Am Assoc Gynecol Laparosc 7: 131-133, 2000.
7. Maxson WS, Hill GA, Herbert CM, Kaufman AJ, Pittaway DE, Daniell JF,
Winfi eld AC, Wentz AC: Ureteral Abnormalities in Women with Endome-
triosis. Fertil Steril 46: 1159-1161, 1986.
8. Loverro G, Cormio G, Greco P, Altomare D, Putignano G, Slevaggi L:
Perforation of the Sigmoid Colon During Pregnancy: A Rare Complication
of Endometriosis. J Gynecol Surg 15: 155-157, 1999.
9. Halme J, Chafe W, Currie JL: Endometriosis with Massive Ascites. Obstet
10. Samora-Mata J, Feste JR: Endometriosis Ascites: A Case Report. JSLS 3:
11. Mendez LE, Echt L, Rock JA, Horowitz IR: Pulmonary Endometriosis: A
Clinical Review. J Pelv Surg 6: 130-135, 2000.
12. Seltzer VL, Benjamin F: Treatment of Pulmonary Endometriosis with a
Long-Acting GnRH Agonist. Obstet Gynecol 76: 929-931, 1990.
13. Torkelson SJ, Lee RA, Hildahl DB: Obstet Gynecol 71: 473-477, 1988.
14. Nezhat C, Seidman DS, Nezhat F, Nezhat C: Laparoscopic Surgical Manage-
ment of Diaphragmatic Endometriosis. Fertil Steril 69: 1048-1055, 1998.
15. Fedele L, Bianchi S, Portuese A, Borruto F, Dorta M: Transrectal Ultrasonog-
raphy in the Assessment of Rectal Vaginal Endometriosis. Obstet Gynecol
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
16. Thorton JG, Morley S, Lilleyman J, Onwude JL, Currie I, Crompton AC:
The Relationship Between Laparoscopic Disease, Pelvic Pain and Infertility: An Unbiased Assessment. Uro J Obstet Gynecol Repro Bio 74: 57-52, 1997.
17. Halstead L, Pepping P, Dmowski WP: The Woman with Endometriosis:
Ignored, Dismissed and Devalued – A Research Pilot Study Presented at the Second International Symposium on Endometriosis. The Endometriosis
18. Chronic Pelvic Pain. ACOG Technical Bulletin. No. 223, May. The Com-
mittee on Technical Bulletins of the American College of Obstetricians and
19. Ling FW: Randomized Control Trial of Depo Leuprolide in Patients with
Chronic Pelvic Pain and Clinically Suspected Endometriosis. Obstet Gynecol
20. Koninckx PR, et al: Suggestive Evidence that Pelvic Endometriosis is a
Progressive Disease, Whereas Deeply Infi ltrating Endometriosis is Associated with Pelvic Pain. Fertil Steril 55: 759-765, 1991.
21. Carter JE: Hysteroscopic and Laparoscopic Findings in Chronic Pelvic Pain.
J Am Assoc Gynecol Laparosc 2: 4, 1994.
22. Ripps BA, Martin DC: Focal Pelvic Tenderness, Pelvic Pain, Dysmenorrhea
and Endometriosis. J Reprod Med 36: 470-472, 1991.
23. Carter JE, Trotter JP: GnRH Analogs in the Treatment of Endometriosis:
Clinical and Economic Considerations. Female Patient. 20: 13-20, 1995.
24. Fedele L, Bianchi S, Bocciolone L, DiNola G, Parazzini F: Pain Symptoms
Associated with Endometriosis. Obstet Gynecol 79: 767-769, 1992.
25. Popora MG, Koninckx PR, Piazze J, Natili M, Colagrande S, Cosmi EV:
Correlation Between Endometriosis and Pelvic Pain. J Am Assoc Gynecol Laparosc 6: 429-434, 1999.
26. Chapron C, Dubuisson J-B, Tardif D, Fritel X, Lacroix S, Kinkel K, Du-
montier I, Dousset B, Vacher-Lavenu M-C: Retroperitoneal Endometriosis and Pelvic Pain: Results of Laparoscopic Uterosacral Ligament Resection
According to the rAFS Classifi cation in Histopathologic Results. J Gynecol
27. Dmowski WP, Lesniewicz R, Rana N, Pepping P, Noursalehi M: Changing
Trends in the Diagnosis of Endometriosis: A Comparative Study of Women
with Pelvic Endometriosis Presenting Chronic Pelvic Pain or Infertility. Fertil Steril 67: 238-243, 1997.
28. Reiter RC, Gambone JC: Demographic and Historic Variables in Women
with Idiopathic Chronic Pelvic Pain. Obstet Gynecol 75: 428-432, 1990.
Internet Appendix 3: Medical Risks of Infertiltiy
29. Chronic Pelvic Pain and Dysmenorrhea. ADS: The Female Patient 10: 79-80,
30. Stovall DW, Bowser LM, Archer DF, Guzick DS: Fertil Steril 68: 13-18, 1997.
31. Redwine DB: Ovarian Endometriosis: A Marker for More Extensive Pelvic
and Intestinal Disease. Fertil Steril 72: 310-315, 1999.
32. Szucs RA, Turner MA: Gastrointestinal Tract Involvement by Gynecologic
Diseases. Radiographics 16: 1251-1270, 1996.
33. Mathias JR, Clench MH: Relationship of Reproductive Hormones and
Neuromuscular Disease of the Gastrointestinal Tract. Dig Dis 16: 3-13, 1998.
34. Dunaif A, Thomas A: Current Concepts in the Polycystic Ovary Syndrome.
35. Dunaif A: Insulin Resistance in the Polycystic Ovary Syndrome: Mechanism
and Implications for Pathogenesis. Endo Rev 18 (6): 774-800, 1997.
36. Heim SC, De Geyter C, Siegrist W, Bilz S, Keller U: Polycystic Ovary Syn-
drome – Only Relevant in Reproductive Medicine? Therapeutische Umscha.
Revue Therapeutique. 56: 271-275, 1999.
37. Dahlgren E, Janson PO, Johansson S, Lapidus L, Oden A: Polycystic Ovary
Syndrome and Risk for Myocardial Infarction – Evaluated from a Risk Factor Model Based on a Prospective Population Study of Women. Acta Obstet Gynecol Scand 71: 599-604, 1992.
38. Hunter MH, Sterrett JJ: Polycystic Ovary Syndrome: It’s Not Just Infertility.
39. Anttila L, Carjala K, Penttila T-A, Ruutiainen K, Ekblad U: Polycystic Ovaries
in Women with Gestational Diabetes. Obstet Gynecol 92: 13-16, 1998.
40. Harlow BL, Signorello LB, Hall JE, Dailey C, Komaroff AL: Reproductive
Correlates of Chronic Fatigue Syndrome. Am J Med 105: 95S-99S, 1998.
41. Slowey MJ: Polycystic Ovary Syndrome: New Perspective on an Old Problem.
42. Crosby PDA, Rittmaster RS: Predictors of Clinical Response in Hirsute
Women Treated with Spironolactone. Fertil Steril 55: 1076-1081, 1991.
43. Young RL, Goldzieher JW, Elkind-Hirsch K: The Endocrine Effects of
Spironolactone Used as an Anti-Androgen. Fertil Steril 48: 223-228, 1987.
44. Pittaway DE, Maxson WS, Wentz AC: Spironolactone in Combination Drug
Therapy for Unresponsive Hirsutism. Fertil Steril 43: 878-882, 1985.
45. Pittaway DE, Wentz AC: Therapeutic Alternatives for the Hirsute Patient.
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
46. Duczman L, Ballweg ML: Endometriosis and Cancer: What is the Connec-
tion? Endometriosis Association, 1999.
47. Brinton LA, Gridley G, Persson I, Baron J, Bergquist A: Cancer Risk After a
Hospital Discharge Diagnosis of Endometriosis. Am J Obstet Gynecol. 176:
48. Nishida M, Watanabe K, Sato N, Ichikawa Y: Malignant Transformation of
Ovarian Endometriosis. Gynecol Obstet Invest 50 (Suppl 1): 18-25, 2000.
49. Bass KM: Epethelial Ovarian Cancer: Epidemiology, Screening, and Preven-
tion. Menopausal Medicine. 4: 8-12, 1996.
50. DiSilvestro PA, Gold MA, Gould NS: Malignancies Arising in Endometriosis.
Prime Care Update. 6: 122-124, 1999.
51. Fishman A, Demirel D, Laucirica R, Ramzy I, Klima T, Lyzak G, Kaplan AL:
Malignant Tumors Arising in Endometriosis: Clinical-Pathological Study and Flow Sytometer Analysis. Euro J Obstet Gynecol Repro Bio 70: 69-74, 1996.
52. Erzen M, Kovacic J: Relationship Between Endometriosis and Ovarian Cancer.
Eur J Gynaec Oncol 19: 553-555, 1998.
53. Baxter SW, Thomas EJ, Campbell IG: GSTM1 Null Polymorphism and
Susceptibility to Endometriosis and Ovarian Cancer. Carcinogenesis. 22:63-65, 2001.
54. Burmeister L, Healy, DL: Ovarian Cancer in Infertility Patients. Ann Med
55. Sugiyama T, Nishida T, Kataoka A, Okura N, Iwanaga S, Yakushiji M: A
Pregnant Woman with Clear Cell Adenocarcinoma of the Ovary Arising
from Endometriosis and with Benign and Borderline Adenoma Fibroma of the Clear Cell and Endometrioid Types. Euro J Obstet Gynecol Repro Bio.
56. Unkila-Kallio L, Tiitinen A, Wahlstrom T, Lehtovrita P, Leminen A: Repro-
ductive Features in Women Developing Ovarian Granulosa Cell Tumour at a Fertile Age. Human Reproduction. 15: 589-593, 2000
57. Zhang Y, Huang H, Lian L: Clinical Discussion of the Relationship Between
Endometriosis and Epithelial Ovarian Cancer. Zhonghua Fu Chan Ke Za Zha. 34: 544-546, 1999.
58. Yoshikawa H, Jimbo H, Okada S, Matsumoto K, Onda T, Yasugi T, Taketani
I: Prevalence of Endometriosis in Ovarian Cancer. Gynecol Obstet Invest. 60
59. Vercellini P, Parazzine F, Bolis G, Carinelli S, Dindelli M, Vendola N, Luchini
L, Crosignani PG: Endometriosis and Ovarian Cancer. Am J Obstet Gynecol.
Internet Appendix 3: Medical Risks of Infertiltiy
60. Obata K, Hoshiai H: Gynecol Obstet Invest. 50 (suppl 1): 39-43, 2000.
61. Nieto JJ, Rolfe KG, MacLean AB, Hardiman P: Ovarian Cancer and Infertility:
A Genetic Link? Lancet. 354: 649, 1999.
62. Jiang X, Morland SJ, Hitchcock A, Thomas EJ, Campbell IG: Allelotyping
of Endometriosis with Adjacent Ovarian Carcinoma Reveals Evidence of a
Common Lineage. Cancer Research. 58: 1707-1712, 1998.
63. Jimbo H, Yoshikawa H, Onda T, Yasugi T, Sakamoto A, Taketani I: Prevalence
of Ovarian Endometriosis in Epithelial Ovarian Cancer. Inter J Gynecol
64. Heaps JM, Nieberg RK, Berek JS: Malignant Neoplasams Arising in Endo-
metriosis. Obstet Gynecol. 75: 1023-1028, 1990.
65. Fukunaga M, Nomura K, Ishikawa E, Ushigome S: Ovarian Atypical
endometriosis: It’s Close Association with Malignant Epithelial Tumours.
66. Escobedo LG, Lee NC, Peterson HB, Wingo PA: Infertility-Associated
Endometrial Cancer Risk May be Limited to Specifi c Groups of Infertile
67. Deslypere JP: Obesity and Cancer. Metabolism. 44: 24-27, 1995.
68. Insler V, Lunenfeld B: Pathophysiology of Polycystic Ovarian Disease: New
Insights. Human Reproduction. 6: 1025-1029, 1991.
69. Parazzini F, La Vecchia C, Negri E, Fedele L, Balotta F: Reproductive Factors
and Risk of Endometrial Cancer. Am J Obstet Gynecol. 164: 522-527, 1991.
70. Coulam CB: Why CA Risk is Higher in Anovulatory Women. Contemporary
71. Coulam CB, Annegers JF, Kranz JS: Chronic Anovulation Syndrome and
Associated Neoplasia. Obstet Gynecol. 61: 403-407, 1983.
72. Archer DF: The Changing Face of Breast Cancer. Clinic Bull Menop. 4: 1-3,
73. Cowan LD, Gordis L, Tonascia JA, Jones GS: Breast Cancer Incidence in
Women with a History of Progesterone Defi ciency. Amer J Epidem. 114:
74. Swain MC, Bulbrook RD, Hayward JL: Ovulatory Failure in a Normal Popula-
tion and in Patients with Breast Cancer. J Obstet Gynaecol Brit Common. 81: 640-643, 1974.
75. McFadyen IJ, Prescott RJ, Groom GV, Forrest APM, Golder MP, Fahmy DR,
Griffi ths K: Circulating Hormone Concentrations in Women with Breast Cancer. Lancet. 1100-1102, May 22, 1976.
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
76. Meyer F, Brown JB, Morrison AS, MacMahon B: Andogenous Sex Hormones,
Prolactin and Breast Cancer in Premenopausal Women. J Nat Can Inst. 77: 613-616, 1986.
77. Secreto G, Toniolo P, Berrino F, Recchione C, Di Pietro S, Fariselli G, Decarli
A: Increased Androgenic Activity and Breast Cancer is Premenopausal Women.
Cancer Research. 44: 5902-5905, 1984.
78. Secreto G, Recchione C, Fariselli G, Di Pietro S: High Testosterone and Low
Testosterone Circulating Levels in Premenopausal Patients with Hyperplasia
and Cancer of the Breast. Cancer Research. 44: 841-844, 1984.
79. Secreto G, Fariselli G, Bandieramonte G, Recchione C, Dati V, Di Pietro S:
Androgen Excretion in Women with a Family History of Breast Cancer or
with Epithelial Hyperplasia or Cancer of the Breast. 1983.
80. Brinton LA, Gridley G, Persson I, Baron J, Bergquist A: Cancer Risk After a
Hospital Discharge Diagnosis of Endometriosis. Am J Obstet Gynecol. 176:
81. Hergenroeder AC, Smith EO, Shypailo R, Jones LA, Klish WJ, Ellis K: Bone
Mineral Changes in Young Women with Hypothalamic Amenorrhea Treated with Oral Contraceptives, Medroxyprogesterone, or Placebo Over 12 Months.
Am J Obstet Gynecol. 176: 1017-25, 1997.
82. Prior JC: Progesterone as a Bone-Trophic Hormone. Endocrine Reviews. 11:
83. Dmowski WP, Steele RW, Baker GF: Defi cient Cellular Immunity in Endo-
metriosis. Am J Obstet Gynecol. 141: 377-383, 1981.
84. Gleicher N, El-Roeiy A, Confi no E, Friberg J: Is Endometriosis an Autoim-
mune Disease? Obstet Gynecol. 70: 115-121, 1987.
85. Oosterlynck DJ, Cornillie FJ, Waer M, Vandeputte M, Koninckx PR: Women
with Endometriosis Show a Defect in Killer Activity Resulting in a Decreased Cytotoxicity to Autologous Endometrium. Fertil Steril. 56: 45-51, 1991.
86. Oosterlynck DJ, Meuleman C, Waer M, Vandeputte M, Koninckx, PR:
The Natural Killer Activity of Peritoneal Fluid Lymphocysts is Decreased in
Women with Endometriosis. Fertil Steril. 58: 290-295, 1992.
87. Johnson KM: Endometriosis: The Immunoendocrine Factor. The Female
88. Nothnick WB: Treating Endometriosis as an Autoimmune Disease. Fertil
89. Nothnick WB: Treating Endometriosis as an Autoimmune Disease. Fertil
Internet Appendix 3: Medical Risks of Infertiltiy
90. Saracoglu FO, Mungan T, Tanzer F: Salpingitis Isthmica Nodosa in Infertility
and Ectopic Pregnancy. Gynecol Obstet Invest. 34: 202-205, 1992.
91. Jenkins CS, Williams SR, Schmidt GE: Salpingitis Isthmica Nodosa: A Review
of the Literature, Discussion of Clinical Signifi cance and Consideration of
Patient Management. Fertil Steril. 60: 599-607, 1993.
92. Houston JG, Machan LS: Salpingitis Isthmica Nodosa: Technical Success
and Outcome of Fluroscopic Transcervical Fallopian Tube Recannulization.
Cardio Vasc Interven Radiol. 21: 31-35, 1998.
93. Honore GM, Holden AEC, Schenken RS: Pathophysiology and Management
of Proximal Tubal Blockage. Fertil Steril. 71: 785-795, 1999.
94. Starks GC, Grimes EM: Obstetric Outcome in Previously Infertile Patients.
Sem Reprod Endocrin. 3: 211-215, 1985.
95. Bhalla AK, Sarala G, Dhaliwal L: Pregnancy Following Infertility. Aust NZ
J Obstet Gynaecol. 32: 249-251, 1992.
96. Collins JA, Rand CA, Wilson EH, Wrixon W, Casper RF: The Better Prognosis
in Secondary Infertility is Associated with a Higher Proportion of Ovulation
Disorders. Fertil Steril. 45: 611-616, 1986.
97. Coulam CB: Association Between Infertility and Spontaneous Abortion. Amer
98. Hakim RB, Gray RH, Zacur H: Infertility and Early Pregnancy Loss. Am J
Obstet Gynecol. 172: 1510-1517, 1995.
99. Strobino B, Fox HE, Kline J, Stein Z, Susser M, Warburton, D: Characteristics
of Women with Recurrent Spontaneous Abortions and Women with Favorable
Reproductive Histories. AJPH. 67: 986-991, 1986.
100. Rossi AM, Vilska S, Heinonen PK: Outcome of Pregnancies in Women
with Treated or Untreated Hyperprolactinemia. Eur J Obstet Gynaecol Reprod Biol. 63: 143-146, 1995.
101. Whitley E, Doyle P, Roman E, De Stavola B: The Effect of Reproductive
History on Future Pregnancy Outcomes. Human Reproduction. 14: 2863-2867, 1999.
102. Gray RH, Wu LY: Subfertility and Risk of Spontaneous Abortion. Am J
103. Guillauma AJ, Benjamin F, Sicuranza B, Deutsch S, Spitzer M: Luteal Phase
Defects and Ectopic Pregnancy. Fertil Steril 63: 30-33, 1995.
104. Tancer ML, Telke I, Veridiano NP: A 15 Year Experience with Ectopic
Pregnancy. Surg Gyn Obstet. 152: 179-182, 1981.
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
105. Tenore JL: Ectopic Pregnancy. Amer Fam Phys. 61: 1080-1088, 2000.
106. Kashyap S, Claman P: Polycystic Ovary Disease and the Risk of Pregnancy
Induced Hypertension. J Repro Med. 45: 991-994, 2000.
107. Urman B, Sarac E, Dogan L, Gurgan T: Pregnancy in Infertile PCOD
Patients. Complications and Outcome. J Repro Med. 42: 501-505, 1997.
108. Gravett MG: Causes of Preterm Delivery. Sem Perinatol. 8: 246-257, 1984.
109. Williams MA, Goldman MB, Mittendorf R, Monson RR: Subfertility and
the Risk of Low Birth Weight. Fertil Steril. 56: 668-671, 1991.
110. Martius JA, Steck T, Oehler MK, Wulf KH: Risk Factors Associated with
Preterm (Less Than 37.0 Weeks) and Early Preterm Birth (Less Than 32.0
Weeks): Univariate and Multivariate Analysis of 106,345 Singleton Births
from the 1994 Statewide Perinatal Survey of Bavaria. Eur J Obstet Gynaecol
111. Vercelline P, De Giorgi O, Aimi G, Panazza S, Uglietti A, Crosignani PG:
Menstrual Characteristics in Women With and Without Endometriosis. Obstet Gynecol. 90: 264-268, 1997.
112. Thomas R, Reid RL: Thyroid Disease in Reproductive Dysfunction: A
Review. Obstet Gynecol. 70: 789-798, 1987.
113. Krassas GE: Thyroid Disease in Female Reproduction. Fertil Steril. 74:
114. Marcus MD, Louchs TL, Berga SL: Psychological Correlates of Functional
Hyptothalamic Amenorrhea. Fertil Steril. 76: 310-316, 2001.
115. Wilcox LS, Mosher WD: Use of Infertility Services in the United States.
116. Bron MS, Salmon JW: Infertility Services and Managed Care. Am J Man
117. Stovall DW, Allen BD, Sparks AET, Syrop CH, Saunders RG, Van Voorihs
BJ: The Cost of Infertility Evaluation and Therapy: Findings of a Self-Insured University Health Care Plan. Fertil Steril. 72: 778-784, 1999.
Internet Appendix 3: Medical Risks of Infertiltiy
Excerpted from Hilgers, TW, The Medical & Surgical Practice of NaProTECHNOLOGY, Pope Paul VI Institute Press, Omaha, Nebraska, 2004.
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
DIREITO PROCESSUAL PENAL PROF. LUIZ FLÁVIO GOMES AULAS 1 E 2 (GABARITO ABAIXO – CONFIRA) 1) Assinale a alternativa incorreta : a) Segundo clássica lição de v.Liszt/Schmidt o ius puniendi possui três momentos: a) direito de ameaçar com penas; b) direito de impor tais penas e c) direito de executá-las. b) O princípio do devido processo legal tem duas acepções, uma delas cons
Comunicato INFLUENZA AVIARIA “COMPLIMENTI STORACE!” GLI ALLEVATORI IN GINOCCHIO, LE CASE FARMACEUTICHE RINGRAZIANO AIAB E LEGAMBIENTE ACCUSANO IL MINISTRO DELLA SALUTE DI AVER AVVIATO LA PSICOSI CAUSA DEL CROLLO DELLE VENDITE DI CARNE AVIARIA “La politica portata avanti dal Ministro Storace in questa crisi da influenza aviaria è avventata”, questo i
 Medical Risks of Infertility
Medical Risks of Infertility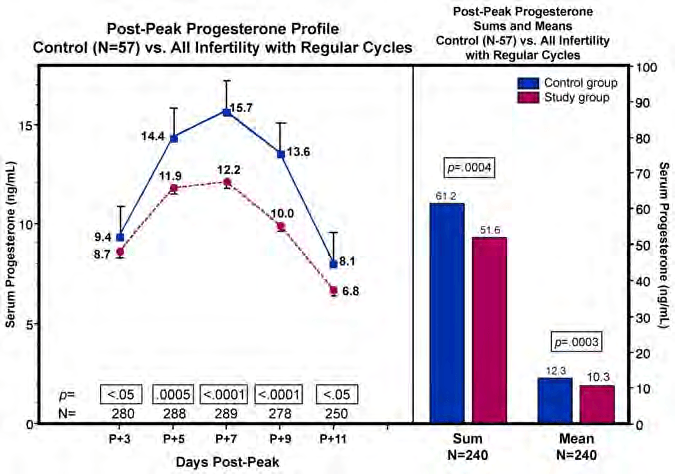 Internet Appendix 3: Medical Risks of Infertiltiy
involvement of the ureter leading to kidney obstruction and uremia
(kidney failure),3 and other areas of the urinary tract.4-7 The sigmoid
colon has been perforated during pregnancy as a result of endometrio-sis8, and massive ascites can also be associated with endometriosis.9-10
Endometriosis has been observed in the lung,11-12 the sciatic nerve,13
the diaphragm,14 and in the rectal/vaginal area15 along with many other
Hormonal Dysfunctions associated with Infertiltiy
Internet Appendix 3: Medical Risks of Infertiltiy
involvement of the ureter leading to kidney obstruction and uremia
(kidney failure),3 and other areas of the urinary tract.4-7 The sigmoid
colon has been perforated during pregnancy as a result of endometrio-sis8, and massive ascites can also be associated with endometriosis.9-10
Endometriosis has been observed in the lung,11-12 the sciatic nerve,13
the diaphragm,14 and in the rectal/vaginal area15 along with many other
Hormonal Dysfunctions associated with Infertiltiy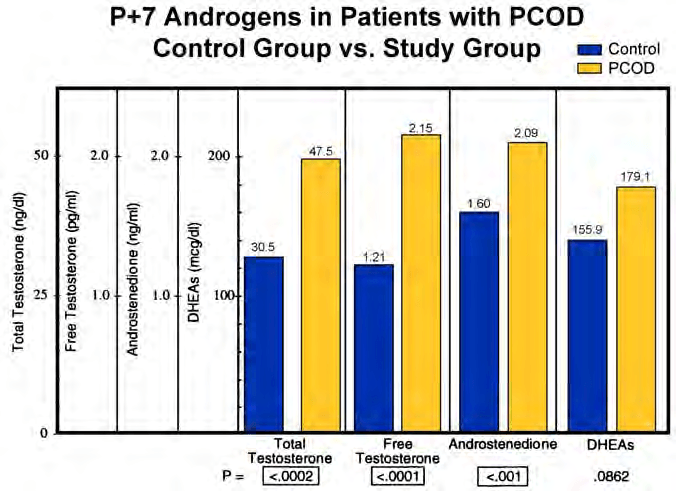 The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
triosis, polycystic ovarian disease, pelvic adhesive disease, and distal
and proximal tubal occlusion, the production of progesterone during
the postovulatory phase of the cycle has been shown to be signifi cantly decreased.
Progesterone is very important to the support of pregnancy and it
also modulates or modifi es the immune system. It supports the immune system and, when the progesterone levels are low, the immune system becomes less effective. It is thought that these decreased progesterone
levels are one reason why women with infertility have an increased risk of various types of cancers (see later).
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
triosis, polycystic ovarian disease, pelvic adhesive disease, and distal
and proximal tubal occlusion, the production of progesterone during
the postovulatory phase of the cycle has been shown to be signifi cantly decreased.
Progesterone is very important to the support of pregnancy and it
also modulates or modifi es the immune system. It supports the immune system and, when the progesterone levels are low, the immune system becomes less effective. It is thought that these decreased progesterone
levels are one reason why women with infertility have an increased risk of various types of cancers (see later).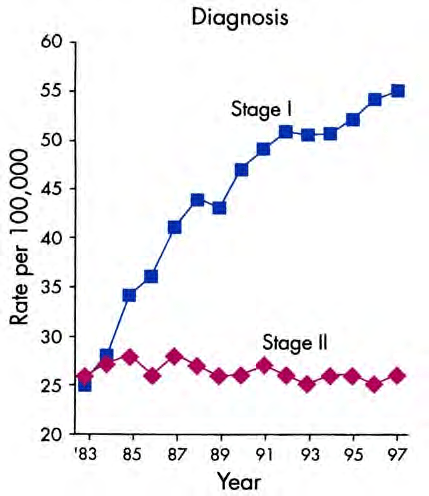 The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
C. Breast Cancer
The NaProTECHNOLOGY Revolution: Unleashing the Power in a Woman’s Cycle
C. Breast Cancer