PRODUCT MONOGRAPH (Amcinonide USP) Cream 0.1% Topical Corticosteroid TaroPharma A Division of Taro Pharmaceuticals Inc. 130 East Drive Brampton, Ontario L6T 1C1 Control # 086229 PRODUCT MONOGRAPH Amcort Cream 0.1% Amcinonide Cream USP 0.1% Therapeutic Classification Topical Corticosteroid
Amcort (amcinonide) Cream is a potent fluorinated topical corticosteroid. Topical
corticosteroids are synthetic derivatives of cortisone which are effective when applied
locally to control many types of inflammatory, allergic and pruritic dermatoses.
Modifications to the chemical structure such as fluorination, generally enhances both
anti-inflammatory activity and increases the likelihood of adverse effects. The
mechanism of anti-inflammatory activity of topical corticosteroids is generally unclear.
However, corticosteroids are thought to induce phospholipase A2 inhibitor proteins,
preventing arachidonic acid release and the biosynthesis of potent mediators of
Topical corticosteroids are primarily effective because of their anti-inflammatory, anti-
pruritic and vasoconstrictive actions.
Amcort Cream 0.1% is indicated for the relief of inflammatory manifestations of acute
and chronic corticosteroid-responsive dermatoses, such as atopic dermatitis, contact and
eczematous dermatoses, psoriasis and neuro-dermatitis.
It must be remembered that steroid therapy, although responsible for remissions of
dermatoses, especially of allergic origin, cannot be expected to prevent recurrence. In
the case of contact or allergic dermatitis, it is important to investigate causal factors and
to remove the offending material or allergen.
Topical steroid therapy is contraindicated in fungal diseases of the skin, untreated
bacterial infections, in tuberculosis of the skin and certain viral diseases such as herpes
Amcort Cream is contraindicated in those patients with a history of hypersensitivity to
any of the components of the products.
Amcort Cream is contraindicated in bacterial/fungal skin infections, tuberculosis of the
skin, syphilitic skin infections, chicken pox, eruptions following vaccinations and viral
Amcort Cream is not for ophthalmic use.
When used under occlusive dressing, over extensive areas, or on the face, scalp, axillae
and scrotum, sufficient absorption may occur giving rise to adrenal suppression and
Systemic absorption of topical corticosteroids can produce reversible hypothalamic-
pituitary-adrenal (HPA) axis suppression with the potential for glucocorticosteroid
insufficiency after withdrawal of treatment. Manifestations of Cushing’s syndrome,
hyperglycaemia and glucosuria can also be produced in some patients by systemic
absorption of topical corticosteroids.
Conditions which augment systemic absorption include application of the more potent
steroids, use over a large surface area, prolonged use and occlusive dressings. Patients
receiving a large dose of potent topical steroids to a large surface area or under an
occlusive dressing should be evaluated periodically for evidence of HPA axis
suppression. This may be done by using the ACT stimulation test or other
recognized/validated test. If HPA axis suppression is noted, an attempt should be made
to withdraw the drug, to reduce the frequency of application, or to substitute a less
potent steroid. Recovery of HPA axis function is generally prompt and complete upon
discontinuation of topical corticosteroids. Infrequently, signs and symptoms of
glucocorticoid insufficiency may occur requiring supplemental systemic corticosteroids.
Occlusive dressings should not be applied if body temperature is elevated. To minimize
systemic absorption when long-term therapy or large surface area for treatment is likely,
periodic interruption of treatment or treatment of one area of the body at a time should
Children may be more susceptible to systemic toxicity from equivalent doses due to
larger skin surface to body mass ratios (see Precautions - Pediatric Use).
Topical corticosteroids, particularly the more potent ones, should be used with caution
on lesions close to the eye because systemic absorption may cause increased intra-
ocular pressure, glaucoma or cataracts.
Prolonged use of topical corticosteroid preparations may produce striae or atrophy of
the skin or subcutaneous tissue. Topical corticosteroids should be used with caution on
lesions of the face, groin and axillae as these areas are more prone to atrophic changes
than other areas of the body. Frequent observation is important if these areas are to be
treated. If skin atrophy is observed, treatment should be discontinued.
If irritation develops, Amcort Cream should be discontinued and appropriate therapy
instituted. Allergic contact dermatitis from corticosteroids is usually diagnosed by
observing ‘failure to heal’ rather than clinical exacerbation as with most topical
products not containing corticosteroids. Such an observation should be corroborated
with appropriate diagnostic patch testing.
Suitable precautions should be taken when using topical corticosteroids in patients with
stasis dermatitis and other skin diseases with impaired circulation.
If concomitant skin infections are present or develop, an appropriate antifungal or
antibacterial agent should be used. If a favourable response does not occur promptly,
use of Amcort Cream should be discontinued until the infection has been adequately
Patients should be advised to inform subsequent physicians of the prior use of
Corticosteroids are generally teratogenic in laboratory animals when administered
systemically at relatively low dosage levels. The more potent corticosteroids have been
shown to be teratogenic after dermal application in laboratory animals. There are no
adequate and well-controlled studies in pregnant women on teratogenic effects from
topically applied corticosteroids. Therefore, Amcort Cream should be used during
pregnancy only if the potential benefit justifies the potential risk to the fetus,
particularly in the first trimester of pregnancy. Drugs of this class should not be used
extensively on pregnant patients, in large amounts, or for prolonged periods of time.
Infants born of mothers who have received substantial doses of corticosteroids during
pregnancy should be carefully observed for hypoadrenalism.
Systemically administered corticosteroids are secreted into human milk and could
suppress growth, interfere with endogenous corticosteroid production or cause untoward
effects. Caution should be exercised when Amcort Cream is administered to a nursing
Safety and effectiveness of Amcort Cream in children and infants have not been
established. Because of the higher ratio of skin surface area to body mass, children are
at a greater risk than adults for HPA axis suppression when treated with topical
corticosteroids. They are also at greater risk of glucocorticosteroid insufficiency after
withdrawal of treatment and of Cushing’s syndrome while on treatment. Adverse
effects including striae have been reported with use of topical corticosteroids in infants
and children. HPA axis suppression, Cushing’s syndrome and intracranial hypertension
have been reported in children receiving topical corticosteroids. Manifestations of
adrenal suppression in children include: linear growth retardation, delayed weight gain,
low plasma cortisol levels and absence of response to ACT stimulation. Manifestations
of intracranial hypertension include bulging fontanelles, headaches and bilateral
Chronic corticosteroid therapy may interfere with the growth and development of
Carcinogenesis, Mutagenicity, Reproduction
Long-term animal studies have not been performed to evaluate carcinogenic potential of
Amcinonide, in doses up to 2000 mg/kg, had no effect on the incidence of micronuclei
in rat polychromatic erythrocytes, indicating no evidence of mutagenic potential in this
test system. The microbial assay was also negative with regard to a mutagenic potential
for amcinonide in concentrations up to 2,500 Fg/well/plate.
The findings of the studies in rats and rabbits are consistent with known teratogenic
effects of glucocorticoids in laboratory animals.
When occlusive dressings are used, pustules, miliaria, folliculitis, and pyoderma may
occur. The following additional local adverse reactions have been reported with topical
corticosteroids and may occur more frequently with use of occlusive dressings. These
reactions are listed in decreasing order of occurrence: burning, itching, irritation,
dryness, folliculitis, hypertrichosis, acneiform eruptions, hypopigmentation, perioral
dermatitis, allergic contact dermatitis, maceration of the skin, secondary infection, skin
atrophy, striae and miliaria. In addition, there are reports of the development of pustular
psoriasis from chronic plaque psoriasis following reduction or discontinuation of potent
Topically applied Amcort Cream can be absorbed systemically. Percutaneous
absorption is enhanced when large amounts of corticosteroid are applied, when used
under occlusive dressing or when used chronically. Toxic effects of hypercorticism and
adrenal suppression may appear. Should toxic effects occur, the dosage of Amcort
Cream should be discontinued slowly, consistent with accepted procedures for
discontinuation of chronic steroid therapy. The restoration of hypothalamic-pituitary
axis may be slow; during periods of pronounced physical stress (severe infections,
trauma, surgery) a supplement with systemic steroids may need to be considered.
Toxic effect may include ecchymosis of skin, striae, discolouration or atrophy of the
skin, peptic ulceration, hypertension, aggravation of infection, hirsutism, acne, edema,
hypokalemia, subcapsular cataracts, muscle weakness and wastage due to protein
depletion. Treatment of a patient with systemic toxic manifestations consists of
assuring and maintaining a patent airway and supporting ventilation using oxygen and
assisted or controlled respiration as required. This usually will be sufficient in the
management of most reactions. Should circulatory depression occur, vasopressors and
i.v. fluids may be used. Should a convulsion persist despite oxygen therapy, small
increments of ultra-short acting barbiturate (pentobarbital or secobarbital) may be given
i.v. Allergic reactions are characterized by cutaneous lesions, urticaria, edema or
Apply Amcort Cream 0.1% to the affected area two or three times daily. Application
twice a day is usually sufficient. Rub in gently and completely. If a symptomatic
response is not noted within a few days to a week, the local applications of
corticosteroid should be discontinued and the patient re-evaluated. Therapy should be
discontinued as soon as lesions heal. The patient should be kept under close
observation if treated with large amounts of topical corticosteroid or with the occlusive
technique or use over a prolonged period of time.
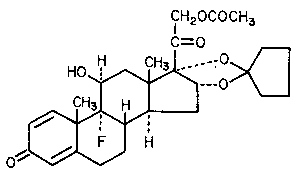
9-Fluoro-11β, 16α, 17, 21-tetrahydroxypregna-1, 4-diene-3,
20-dione cyclic 16, 17-acetal with cyclopentanone, 21-acetate
Amcinonide occurs as a white to cream coloured crystalline
powder, having not more than a slight odour.
Amcinonide is soluble in alcohol, methanol; sparingly soluble in
acetone and chloroform; slightly soluble in ether and insoluble in
Amcort Cream 0.1% contains 1 mg/g amcinonide in a base of benzyl alcohol (as
preservative), emulsifying wax, glycerin, isopropyl palmitate, lactic acid, purified water,
Amcort Cream 0.1% should be stored at controlled room temperature 15E-30EC. Avoid
Amcort Cream 0.1% is recommended for topical use and is available in 4, 15, 30 and 60
Amcort Cream 0.1% Amcinonide Cream USP, 0.1% Information for the Patient
Please read this leaflet before you start using Amcort Cream 0.1%. Each time you
renew your prescription, re-read the leaflet that comes with your medicine, just in case
any information has changed. Remember, this leaflet does not take the place of talking
to your health care provider (such as your doctor, nurse, or pharmacist). You and your
health care provider should discuss Amcort Cream 0.1% while you are using it. What is Amcort?
· Amcort Cream is the brand name of TaroPharma’s amcinonide cream. Amcort Cream
is a topical corticosteroid. It belongs to the general family of medicines called steroids
and is used to help relieve redness, swelling, itching, and discomfort of many skin
· Amcort is a white cream. Amcort Cream 0.1% contains 1 mg/g amcinonide in a base
of benzyl alcohol (as preservative), emulsifying wax, glycerin, isopropyl palmitate,
lactic acid, purified water, and sorbitol solution 70%. Before using Amcort:
· Tell your doctor if you are currently using or have previously used corticosteroids for
the treatment of skin disorders, allergic reactions, arthritis or asthma and if you have
ever had any unusual or allergic reaction to corticosteroids. Also tell your doctor if you
are allergic to any other substances, such as food, preservatives, or dyes.
· Tell your doctor if you are pregnant, intend to become pregnant or are breast- feeding
or intend to breast-feed before using Amcort. How to use Amcort:
· This medication is to be used only as directed by your doctor. Do not use more of it,
do not use it more often, or do not use it for a longer period of time than your doctor has
· Rub a small amount of Amcort Cream into to the affected area 2 or 3 times daily.
Don't put on too much; a thin layer works best.
· Contact your doctor if there is no improvement in your condition within one (1) week.
· Do not to use Amcort for any other skin condition without asking your doctor first.
· Be careful not to get this medication in your eyes. Wash your hands after using this
· Do not bandage or otherwise cover or wrap the treated skin area unless your doctor has
While you are using Amcort:
· Do not get any vaccinations while you are using this medication without your doctor's
· Tell your doctor if you experience side effects to Amcort (e.g., burning or stinging). How to store Amcort:
Amcort Cream 0.1% should be stored at controlled room temperature 15 -30°C. Avoid
A Division of Taro Pharmaceuticals Inc.
C14 amcinonide was administered intravenously to rats and dogs at a dose of 1 mg/kg.
The plasma radioactivity showed a biexponential disappearance and the major portion
(86 - 90%) of the dose was excreted in the feces by both species. After six hours, plasma
concentrations were in the order of 10% of those at 15 minutes, suggesting a half-life of
Similar results were seen when C14 amcinonide was administered orally and
intraperitoneally. It appears that a slower rate of excretion occurs following intra-
muscular and, perhaps, subcutaneous administration than following oral, intravenous or
Rats and dogs were treated topically with 0.5% C14 amcinonide cream. Rabbits were
treated with 0.05% C14 amcinonide cream.
In rats, the data on recovery of the drug in the urine and feces showed that 6.7% (4.4 to
8.7) and 8.1% (4.3 to 12.6) of the dose was excreted at the 1.0 and 5.0 mg/kg dose
levels, respectively. In the rabbit, percutaneous absorption of C14 amcinonide from the
0.05% cream formulation was relatively high; for exposure periods of one to six hours,
total excretion in urine and feces was 7 - 20% of the radioactivity applied. In the dog,
the proportion of the dose excreted was similar to that in rats.
When rabbits were exposed to multiple topical doses of up to 0.5 mg/kg amcinonide
applied daily for three weeks in ointment form, the during-life and postmortem findings
were characteristic of those associated with prolonged glucocorticoid administration and
in agreement with previous results in the cream formulation studies. Similarly, when
rabbits were exposed to 0.05% C14 amcinonide ointment (0.5 mg amcinonide/kg)
applied to intact and abraded skin for up to 6 hours, 4 to 9% of the radioactivity was
recovered in the excreta, also consistent with cream formulation studies.
When rats were exposed to topical applications of 0.05% C14 amcinonide (0.5 mg/kg) in
propylene carbonate ointment for up to 6 hours, 16 to 39% of the applied dose was
recovered in urine and feces. The number of variables involved precluded direct
comparison with previous absorption studies in rats utilizing the 0.1% amcinonide
The extent of metabolism of C14 amcinonide in rats and dogs was measured. In both
species, there was little or no parent drug found in the urine and feces. At least five
metabolites were present in the rat and four in the dog. The identities of these
The vasoconstrictor activity of 0.1% amcinonide cream was compared with that of
0.12% betamethasone valerate and 0.1% triamcinolone acetonide creams.
Twenty-four healthy male volunteers, aged 26 - 47, having no history of dermatologic
disease, were used in this double-blind study. Forty-eight patches, containing the test
materials at various dilutions, were applied in random order to the upper backs of each
subject. After four hours, they were removed and the degree of skin blanching
determined at 2, 5, 20 and 24 hours following removal of the patches.
(1) When the frequencies of positive vasoconstrictor reactions were compared at each
time interval, no significant differences were found in the vasoconstrictor activities of
(2) When eight different dilutions of the cream preparations were compared according
to the degree of blanching produced, no differences were found between the blanching
activity of the eight diluted samples of amcinonide cream and the eight corresponding
dilutions of triamcinolone acetonide cream. Only one significant difference occurred in
the comparisons of results for eight amcinonide cream dilutions and eight
betamethasone valerate cream dilutions, that is 0.12 x 4-3% betamethasone valerate
cream produced a greater degree of blanching than 0.1 x 4-3% amcinonide cream.
(3) The 50% effective dose values were very similar for all three cream preparations
The overall conclusion was made that there was very little difference in the
vasoconstrictor activity of 0.1% amcinonide cream, 0.12% betamethasone valerate
cream and 0.1% triamcinolone acetonide cream.
In another study, the vasoconstrictor activity of 0.1% amcinonide cream was compared
with that of 0.1 % triamcinolone acetonide cream and 0.1% betamethasone valerate
Ten mg quantities of 0.1% amcinonide cream were applied to prescribed areas (2 cm) of
intact skin on the forearm of 30 normal, adult volunteers. The reference formulation
(0.1% triamcinolone acetonide or 0.1% betamethasone valerate cream) was applied at
another test site on the same arm. Readings were made 16 and 23 hours after
The degree of vasoconstriction observed with each steroid preparation was scored: - (no
response), +, ++, +++. Activity was determined by summing the scores of all patients (+
= 1, ++ = 2, +++ = 3). Activity was expressed in two ways: (1) as the combined 16-hour
and 23-hour scores or (2) as the 23-hour scores alone.
In the two assays comparing 0.1% amcinonide cream with 0.1% triamcinolone
acetonide cream, combined scores for amcinonide were 4 and 8 times higher than
combined scores for triamcinolone acetonide, while the 23-hour scores were 3 and 7
times higher for amcinonide than for triamcinolone acetonide.
In three assays comparing 0.1% amcinonide cream with 0.1% betamethasone valerate
cream, the combined scores and the 23-hour scores ranged from 2.2 to 2.8 times higher
for amcinonide than for betamethasone valerate.
In summary, 0.1% amcinonide cream was found to have substantially greater
vasoconstrictor activity than either 0.1% triamcinolone acetonide or 0.1% beta-
methasone valerate creams. This result differs from that obtained in the first study
described above. The difference in results may be related to the different assay
conditions employed in the two studies.
A study was conducted in 30 normal volunteers comparing, in each subject, the
vasoconstrictor activity of amcinonide ointment 0.1% in propylene carbonate base with
amcinonide cream 0.1%amcinonide ointment 0.1% in benzyl alcohol baseARISTOCORT® Ointment 0.1% (triamcinolone acetonide)ARISTOCORT A® Ointment 0.1% (triamcinolone acetonide in Aquatain base)betamethasone diproprionate ointment 0.05%betamethasone valerate ointment 0.1%amcinonide ointment base - placebo
Amcinonide ointment 0.1% in propylene carbonate base exhibited the highest mean
vasoconstriction score among the seven active treatments. The differences between its
mean score and those of the other active preparations indicated a statistical advantage
(P#0.05) for amcinonide ointment in propylene carbonate base over four of the
treatments (betamethasone valerate ointment, amcinonide cream, ARISTOCORT®
Ointment and ARISTOCORT A® Ointment). Vasoconstrictor activity of amcinonide
ointment in propylene carbonate base was not statistically different from that achieved
with amcinonide ointment in the benzyl alcohol base or betamethasone diproprionate
A one-period, randomized, vasoconstrictor study was performed with 35 prescreened,
qualifying subjects to compare Amcort Cream 0.1%, manufactured by TaroPharma, A
Division of Taro Pharmaceuticals Inc. with the Canadian marketed product, Cyclocort®
Cream 0.1%, manufactured by Stiefel Canada Inc.
A 10µl amount of cream was applied to the subject’s forearm and left in place for seven
minutes. The degree of vasoconstriction was determined with a Chroma Meter at pre-
dose, 0, 2, 4, 6, 8, 10, 12, 20 and 24 hours after removal.
The area under the response curve from 0-24 hours was determined using the Chroma
Meter data and results are tabulated below:
Summary of Bioequivalence Evaluations
Statistical evaluation of the vasoconstrictor activity determined by the Chroma Meter
indicated that the vasoconstrictor response from TaroPharma’s Amcinonide Cream 0.1%
was not statistically different from that obtained from Cyclocort® Cream 0.1%.
Rats were given large, single, oral or topical doses (22.5 – 50.0 g/kg) of 0.5% cream or
ointment formulations of amcinonide. No deaths occurred during the seven-day
observation period. Slight lethargy lasting less than 24 hours followed oral dosing. Body
weight gains of the drug-treated animals were less than those of the placebo cream or
placebo ointment treated control animals. Body weight gains of rats treated topically with
cream or ointment bases were comparable to those of the sham-treated control animals.
Decreases were noted in the weights of the thymus and spleen of animals treated with
amcinonide either orally or topically.
A statistically significant decrease in the weight of the adrenal glands was found only
after oral administration of the cream formulation of amcinonide.
No drug-related deaths occurred in rats or mice after the single oral administration of the
largest volume practical of amcinonide ointment at doses up to 50 mg/kg amcinonide in
mice, 42 mg/kg in rats. Depression in weight gain was exhibited by the high dose groups
In order to evaluate the hazard following an accidental ingestion by a child, amcinonide
0.1% cream and 0.1% lotion were administered in massive doses by gavage to fasted
adult rats of both sexes. The results indicated that both formulations, in the total amount
presumably available on prescription in each supply, if ingested by a child (1 - 1.5 g/kg
for a 20 kg child) would present no hazard.
Amcinonide cream or ointment formulations were applied to intact or abraded skin of
rabbits. At 72 hours after drug application, grade 1 erythema (slight - barely perceptible)
was observed in one of six rabbits that received 0.5 g of amcinonide 0.5% cream
formulation and in one of six rabbits that received 0.5 g of amcinonide 0.5% ointment
formulation. Grade 1 erythema was observed at 24 hours, but not at 72 hours, in one of
six rabbits treated with placebo cream; no irritation was observed in rabbits treated with
placebo ointment. Daily application of 1 g/kg placebo cream for seven days produced
grade 1 erythema in one rabbit on day 3, in two animals on days 4 and 5, and in five
animals on day 6; erythema was observed in all six rabbits on day 7. Reactions were seen
at both abraded and non-abraded sites.
Rabbits tolerated the topical application of 0.5 g of 0.1% amcinonide ointment or
ointment vehicle to intact and abraded skin very well. The slight erythema noted on the
abraded skin of four animals (2/6 experimental, 2/6 vehicle control) after the removal of
the occlusive dressing, disappeared within 24 hours.
In another study, amcinonide 0.1% cream and 0.1% lotion as well as the vehicles alone
were applied topically to abraded skin of rabbits for 7 consecutive days. The tolerance of
both cream and lotion at the site of application was good and compared favourably to the
response obtained with the vehicles alone.
Amcinonide ointment, 0.1%, produced no reactions that were considered irritant or
allergic in 25 human subjects tested in a maximization study. It was concluded that the
drug as formulated has an extremely low or negligible potential for irritation or contact
No opacity of the cornea or inflammation of the iris or conjunctiva was produced by
single doses of 0.1 mL of amcinonide 0.5% cream and ointment formulations, no signs of
irritation were produced by daily instillation of 0.1 mL of the 0.5% cream or ointment
No findings related to treatment were noted in rabbit eyes when either a 0.1 g dose of
0.1% amcinonide ointment or ointment vehicle or a 0.1 g dose of 0.1% amcinonide lotion
or lotion vehicle was introduced into the eyes.
Ninety-day topical or subcutaneous administration to the rabbit has shown that repeated
topical applications of the cream or ointment formulations of amcinonide were well
tolerated; only some degree of erythema was seen at the application sites of all treated
The findings on liver, kidney, muscle, blood chemistry and hematology are typical of the
direct and indirect effects of potent glucocorticoids. Their incidence and intensity in
these studies are, in general, a function of dose, route of administration and duration of
Any indication of toxicity observed in the ointment studies was limited to symptoms
typically associated with glucocorticoid administration. No unique toxicity was observed
1. Walker, B.E.: Induction of cleft palate in rats with anti-inflammatory drugs. Teratology 4:39-42, 1971.
2. Walker, B.E.: Induction of cleft palate in rabbits by general glucocorticoids. Proc. Soc. Exp. Biol. Med. 125:1281-1284, 1967.
3. McKenzie, A.W.: Percutaneous absorption of steroids. Arch. Derm. 86:611-614,November, 1962.
4. Stoughton, R.B. and McKenzie, A.W.: Scientific Exhibit, American MedicalAssociation, Florida, November, 1964.
5. Rocha, G.L., Quinete, S.S., Dantas, F. and Faria, T.: A double-blind comparative studybetween amcinonide and betamethasone valerate in the treatment of eczematoidconditions. Curr. Ther. Res. 19:538, 1976.
6. Ishihara, M.: Studies on the vasoconstrictor activity of amcinonide, a new synthetictopical corticosteroid. The Nishinihan Journal of Dermatology (Nishi-Nihon Hitu),38:(2)286-293, 1976.
7. Quinete, S.S., Dantas, F.E., Faria, T. and Rocha, G.L.: Comparison of the efficacy ofamcinonide, a new topical corticosteroid, and triamcinolone acetonide. A Folha Medica74:(1), 1977.
8. Product Monograph for Cyclocort® Cream 0.1%, February 24, 1982, LederleLaboratories, Cyanamid Canada Inc.
9. Package insert for Cyclocort® Cream, Ointment and Lotion, September 1998,Fujisawa Healthcare, Inc., Deerfield, IL 60015.
Presseinformation Dr. Ursula Grohs Mühelos rauchfrei Reihe: GU Multimedia mit CD 80 Seiten, ca. 20 Farbfotos Format: 16,5 x 20 cm. Klappenbroschur, Preis: 16,99 € (D)/ 17,50 € (A)/ 29,90 sFr ISBN 978-3-8338-2397-8 Erscheinungstermin: Dezember 2011 Denken Sie sich rauchfrei! Endlich mit dem Rauchen aufhören? In nur sechs Wochen und das mit einem Nichtrauchertraining, d
Gastric Ulcers: Your Questions Answered Since the first Gastric Ulcer Awareness Month in 2007, it has been well documented that approximately 60 per cent of performance horses are affected by gastric ulcers. Despite this, it is believed that it is still one of the most under-recognised problems in the equine The main reason for this lack of detection is likely to be the vague and non-spec
 9-Fluoro-11β, 16α, 17, 21-tetrahydroxypregna-1, 4-diene-3,
20-dione cyclic 16, 17-acetal with cyclopentanone, 21-acetate
Amcinonide occurs as a white to cream coloured crystalline
powder, having not more than a slight odour.
Amcinonide is soluble in alcohol, methanol; sparingly soluble in
acetone and chloroform; slightly soluble in ether and insoluble in
Amcort Cream 0.1% contains 1 mg/g amcinonide in a base of benzyl alcohol (as
preservative), emulsifying wax, glycerin, isopropyl palmitate, lactic acid, purified water,
Amcort Cream 0.1% should be stored at controlled room temperature 15E-30EC. Avoid
Amcort Cream 0.1% is recommended for topical use and is available in 4, 15, 30 and 60
Amcort Cream 0.1%
9-Fluoro-11β, 16α, 17, 21-tetrahydroxypregna-1, 4-diene-3,
20-dione cyclic 16, 17-acetal with cyclopentanone, 21-acetate
Amcinonide occurs as a white to cream coloured crystalline
powder, having not more than a slight odour.
Amcinonide is soluble in alcohol, methanol; sparingly soluble in
acetone and chloroform; slightly soluble in ether and insoluble in
Amcort Cream 0.1% contains 1 mg/g amcinonide in a base of benzyl alcohol (as
preservative), emulsifying wax, glycerin, isopropyl palmitate, lactic acid, purified water,
Amcort Cream 0.1% should be stored at controlled room temperature 15E-30EC. Avoid
Amcort Cream 0.1% is recommended for topical use and is available in 4, 15, 30 and 60
Amcort Cream 0.1%