Evaluation of disability from chronic fatigue syndrome (cfs), fibromyalgia (fms), multiple sclerosis (ms)
Disability Litigation for Attorneys and Patients: The Functional Capacity Method of evaluating fibromyalgia and chronic fatigue syndrome disability is scientifically invalid and should not be used. Richard Podell, MD, MPH Clinical Professor, UMDNJ-Robert Wood Johnson Medical School (105 Morris Avenue, Springfield, NJ, tel. 973 218-9191; Web address: DrPodell.Org (This essay adapts Dr. Podell’s lecture to the American Conference Institute’s 10th National Advanced Forum on Resolving Disability Insurance Claims and Litigation, June 2007. The American Conference Institute’s legal seminars are balanced to provide equal participation from attorneys for both plaintiff and defense.) Summary: Current methods for evaluating disability for fibromyalgia and chronic fatigue syndrome are grossly inadequate. One method in particular, the Functional Capacity Evaluation (FCE) is demonstrably false and should not be permitted. The FCE asks patients to do mild to moderate exertion over a period of several hours. The examiner then uses these observations to predict whether that person could continue to perform at a similar level of activity week after week for 40 hours a week, as would be required for a job. The FCE should be banned from disability litigation. This is because its core assumption, that one can predict 40 hour a week performance by observing for just three to six hours-- this core assumption can be proved to be false. And not only false, but highly misleading. I will focus on these three pivotal questions: 1. What Is Fibromyalgia and What Is Chronic Fatigue Syndrome. What “Objective” evidence of Illness do You Expect to Find on Physical Examination or Laboratory Tests? 2. What is the Scientific Evidence That the Pain of Fibromyalgia and the Fatigue of Chronic Fatigue Syndrome are in fact real? 3. How the clinical pattern of FMS and CFS is different from that of many other conditions that disability insurance carriers see. Why that causes misunderstanding 4. How this difference in clinical pattern requires different tools for evaluating disability. Why the often used tool of Functional Capacity Evaluation (FCE) should not be used for Fibromyalgia or Chronic Fatigue Disability. What Is Fibromyalgia. What Is Chronic Fatigue Syndrome?
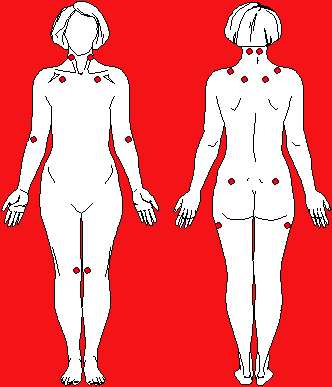
Definition of Fibromyalgia: The American College of Rheumatology Criteria For Fibromyalgia Requires:
1) History of widespread chronic pain in 4 quadrants of 2) Abnormal tenderness at 11 or more of 18 designated anatomic sites, called tender points. 3) Appropriate Rule/outs Clarification: Tender points are areas of muscle/tendon insertion. These “points” are normally more sensitive to painful stimuli than other sites. To be abnormal the
patient must report pain, not just tenderness. Examine pressing with the thumb using a force that just makes thumbnail blanch. Tender point counts can vary from day to day. Psychological distress makes tender points more painful. A person who has chronic widespread pain but < l1 of 18 tender points meets the definition for chronic pain syndrome. Technically, fibromyalgia is a sub-class of chronic pain syndrome
Please note: The formal definition of fibromyalgia
provides no guide to assessing disease severity or disability.
One can be disabled from fibromyalgia despite having only 11 positive tender points on a given day. Or one might be able to work despite having 18 out of 18 positive tender points. In principle, one can be disabled due to chronic pain syndrome, even when it does not meet the definition of fibromyalgia e.g. if there is severe, widespread pain but with only a few positive tender points.
Other than tender points there are no objective finding to be looked for on physical examination or standard laboratory tests that measures the severity of fibromyalgia (or of chronic fatigue syndrome). However certain findings, when present, do provide evidence that illness is major. For example, abnormal results on formal neurocognitive testing; low blood pressure, increased heart rate and/or fall in blood pressure with prolonged standing.
The same holds true for Chronic Fatigue Syndrome:
No specific physical exam or lab findings are required to
There are no specific findings on physical exam or lab
that reliably measures disease severity.
There are no specific findings on physical exam or lab
that distinguish between one person with fibromyalgia or chronic fatigue syndrome who is able to work from another person with fibromyalgia or chronic fatigue syndrome who is, in fact, disabled.
So far as the physical exam and standard lab tests are
concerned, both persons can appear exactly the same. Yet despite the same appearance, one person has the stamina to
sustain a regular level of function for five days a week. The other person cannot.
Definition of Chronic Fatigue Syndrome. This section reprints sections from the Center for Disease Control’s Webpage as last modified May 6, 2006: I have omitted or adapted non-essential parts for editorial clarity. Diagnostic Challenges
Diagnosing chronic fatigue syndrome (CFS) can be complicated by a number of factors: 1) there's no diagnostic laboratory test or biomarker for CFS, 2) fatigue and other symptoms of CFS are common to many illnesses, 3) CFS is an invisible illness and many patients don't look sick, 4) the illness has a pattern of remission and relapse, 5) symptoms vary from person to person in type, number and severity, and 6) no two CFS patients have exactly the same symptom set. These factors have contributed to an alarmingly low diagnosis rate. Of the four million Americans who have CFS, less than 20% have been diagnosed. Clinical Evaluation Because there is no blood test, brain scan or other lab test to diagnose CFS, it's a diagnosis of exclusion. Your health care professional will first take a detailed patient history, including a review of medications that could be causing your fatigue. A thorough physical and mental status examination will also be performed. Next, a battery of laboratory screening tests will be ordered to help identify or rule out other possible causes of your symptoms. Your professional may also order additional tests to follow up on results of the initial screening tests. Diagnostic Criteria Your clinician should consider a diagnosis of CFS if these two criteria are
1. Unexplained, persistent fatigue that's not due to ongoing exertion, isn't
substantially relieved by rest, is of new onset (not lifelong) and results in a significant reduction in previous levels of activity.
2. Four or more of the following symptoms are present for six months or
o Postexertional malaise (extreme, prolonged exhaustion and
sickness following physical or mental activity)
o Multijoint pain without swelling or redness
o Sore throat that's frequent or recurring
o Tender cervical or axillary lymph nodes
Exclusionary Conditions
Chronic fatigue syndrome can resemble many other illnesses, including mononucleosis, chronic Lyme disease, lupus, multiple sclerosis, fibromyalgia, primary sleep disorders, severe obesity and major depressive disorders. Medications can also cause side effects that mimic the symptoms of CFS. Because CFS can resemble many other disorders, it's important not to self-diagnose CFS. It's not uncommon for people to mistakenly assume they have chronic fatigue syndrome when they have another illness that needs to be treated. If you have CFS symptoms, consult a health care professional to determine if any other conditions are responsible for your symptoms. A CFS diagnosis can be made only after other conditions have been excluded. It's also important not to delay seeking a diagnosis and medical care. CDC research suggests that early diagnosis and treatment of CFS can increase the likelihood of improvement.
What is the “Objective” Evidence (besides the patient’s self-report) that the Pain of Fibromyalgia and the Fatigue of Chronc Fatigue are In Fact “Objectively” Real?
In principle, an individual patient could fake or
exaggerate his or her report of pain on the tender point exam. However, many research studies now show that, as a group, fibromyalgia patients do accurately report the pain that they feel. Objective research studies confirm that fibromyalgia patients 1) feel pain when exposed to much lower levels of minor trauma/adverse stimuli compared to normals. 2) Experience a more rapid increase in pain levels when traumatic or noxious stimuli are repeated 3) Have a slower decay/decline of pain levels after the experimental stimulus is removed
4) Have a halt or reversal of the decline of pay after experimental stimulus stops, if even a very small adverse stimulus is reintroduced. In contrast, among normals, adding such small adverse stimuli do not prevent the pain’s decline and resolution.
These research articles are relevant to establishing that
-- Fibromyalgia is mediated through physical mechanisms.
Psychological factors can trigger and/or exacerbate or result from fibromyalgia; but the primary nature of this disease is physical.
-- The main “end organ damage” of fibromyalgia affects the
pain signaling pathways within the central nervous system (spinal cord and brain).
-- Fibromyalgia patients, for the most part, accurately report
The following research articles that support these
conclusions. I offer representative quotations from their abstracts.
Cook D, Lange G Ciccone D et. Al., Functional imaging of pain in patients with primary fibromyalgia, J Rheumatol 2004;31:364-78
“Subjects underwent fMRI scanning while receiving painful and nonpainful heat stimuli… fMRI data indicated that the FM group exhibited greater activity than controls over multiple brain regions in response to both nonpainful and painful stimuli (p < 0.01). . Data from the practice session indicated brain activity in pain-relevant areas for the FM group but not for controls. CONCLUSION: Our results provide further evidence for a physiological explanation for FM pain. Staud R and Rodriguez M, Mechanisms of Disease: pain in fibromyalgia syndrome, Nature Clinical Practice Rheumatology, 2005; 3: 90-98
“Persistent or intense nociception (noxious stimuli) can lead to transcriptional and translational changes in the spinal cord and brain resulting in central sensitization and pain. This mechanism represents a hall mark of fibromyalgia and many other chronic pain syndromes…”
Harris R and Clauw D, How Do We Know That the Pain in Fibromyalgia is “Real”? , Current Pain and Headache Reports 2006; 10:403-7
“ …neurobiological studies indicate that fibromyalgia patients have abnormalities within central brain structures that normally encode pain sensations in healthy pain-free controls…There are now multiple, converging lines of evidence confirming that the pain of fibromyalgia is “real” and that there are strong neurobiological underpinnings to this condition.” Gracely R, Petzke F, Wolfe M, Clauw D Functional magnetic resonance imaging evidence of augmented Pain Processing in Fibromyalgia, Arthritis & Rheumatism 2002:46: 1333-43 “In FM patients, application of mild pressure produced subjective pain reports and cerebral responses that were qualitatively and quantitatively similar to many of the effects produced by application of at least twice the pressure in control subjects.” In summary: Fibromyalgia was first recognized by rheumatology/arthritis specialists. It was first thought to involve mainly the muscles and joints. However, as research has developed, we now know that a major part of this illness affects the pain signaling pathways of the central nervous system–the brain and the spine. This is the main site of the “end-organ damage”. This distortion of neural pain pathways has been given the name “neural sensitization”.
A useful way of thinking about neural sensitization is to imagine a
radio with the volume dial turned up very high, and the station selection knob being slightly off frequency. Hence, the amplification and distortion of pain signaling to the brain.
What About Chronic Fatigue Syndrome (CFS) patients? Do
There is an analogous research literature on chronic fatigue
syndrome, although this is less extensive than in fibromyalgia. However, functional MRI studies also tend to confirm that brain activity during effort is abnormal in CFS.
Lange G, Steffner, J, Cook, D et. Al. Objective evidence of cognitive complaints in Chronic Fatigue Syndrome: A BOLD fMRI study of verbal working memory, NeuroImage 2005; 26: 513-524
Using functional MRI, Lange compared a group of “mentally healthy”
patients with CFS to healthy controls. “Thus, CFS patients have more anatomical changes in the brain than do healthy controls–independent of whether or not they also have psychological illness.”
Using changes in regional blood flow in the brain as a measure, Lange
also showed that CFS patients when challenged with a mental task, had to recruit many more areas of the brain to fulfill the mental task than did controls. This abnormality was present even among those whose formal standard neuropsychological test results were normal. “This confirms that there is something wrong with brain function among chronic fatigue syndrome patients, that current standard neuropsychological tests may be unable to detect. In these patients, they are able to fulfill the initial challenge adequately in the short term, but have to exert substantially greater mental effort to do so. This is consistent with the clinical observation that many CFS patients can think clearly for short periods, but pay the price of increased symptoms and decreased function after prolonged effort.
Summary: “Individuals with CFS appear to have to exert greater effort to process auditory information as effectively as demographically similar healthy adults. Our findings provide objective evidence for the subjective experience of cognitive difficulties in individuals with CFS.” How Should Medical Examiners Evaluate Disability for chronic fatigue syndrome? In most cases there are no findings on physical examination or standard lab testing that reliably distinguishes one person with CFS who is disabled and another person with CFS who is still able to work. Given two individuals with CFS–one unable to work and one able to work despite the obstacle of the illness–these two individuals could have exactly the same findings on physical examination and exactly the same values on most standard lab tests.
Therefore, with only a few exceptions it is medically incorrect to claim
that an individual with CFS is still able to work because physical exam and labs provides “no objective evidence” to the contrary. At the same time abnormalities such as tender muscles, enlarged lymph glands, and positive Epstein Barr antibody tests are often present among persons with CFS, who, despite their illness are still able to work. Therefore, to the extent that the patient’s self-reported symptoms and limitations are credible, the judgment of disease severity must usually be based, first and foremost, on the patient’s self-report of symptoms and abilities. The credibility of these self-reports in turn should be based on “objective” factors including, most importantly, the documented medical records, consistency of the self-reports with the known patterns of disease, the medical opinion of treating physicians, the medical opinion of “expert” physicians, personal diaries, surveillance and other information about how the patient in fact lives and functions.
. The Delayed Post-exertional Flare-up Phenomenon–A Critical Difference Between CFS/FMS and Other Conditions that Insurance Carriers are More Used To
The most crucial difference between the clinical patterns of Fibromyalgia and Chronic Fatigue Syndrome and those of many other conditions is the timing of the Flare-Up of Symptoms that typically occurs because of physical effort.
For example, when a person with angina, a lumbar disc or emphysema pushes past their limits, the increase in symptoms typically occurs during the period of exertion. We call this an immediate or acute exertional flare-up. Symptoms increase during the exertion and decrease rapidly once the activity is stopped. In an observed setting such as a Functional Capacity Evaluation subjects report increased symptoms in real time. The observer may observe signs of distress and/or objective changes on vital signs, ability to bend over, strength, EKG, oxygen saturation, etc. In CFS and fibromyalgia the typical clinical pattern is very different.The patient might or might not have increased symptoms during the exertion, but whether they do or do not, their symptoms of fatigue, pain, poor concentration, etc. typically flare some hours or even a day or two later. We call this the Delayed Post-Exertional Flare-up Phenomenon. The flare up of pain and/or fatigue typically lasts 24 hours or more. The longer or more often the patient tries to push through, the worse and the longer the flare-up.
In an FCE setting, the subject might appear to be okay at the end of the session, but might then “crash” hours later or the next day. They might then remain more symptomatic for 24 hours or more. Unless, the Post-Exertional Flare-up Phenomenon is sought out by the observer, the observer will necessarily be unaware of the negative consequences of the activity session.
This fact alone negates the validity of current FCE protocols.
Current protocols do not seek out or attempt to recognize the delayed post-exertional flare-up. Yet a key issue in deciding whether or not a patient is disabled is whether they are, in fact, telling the truth—that modest activity increases symptoms not necessarily during the exertion but hours or a day later. In principle the truth or
falsity of these claims could be objectively determined e.g. by testimony of persons who are familiar with the patient’s usual patterns of activity; by prolonged (and fairly interpreted) video surveillance; by a patient’s wearing a simple device that measures activity (e.g. a pedometer).
The post-exertional flare-up phenomenon is well known to
physicians who specialize in treating chronic fatigue syndrome and/or fibromyalgia patients and has been measured in research studies. Reference: Kaufman K and Goodnick P, Depression, Chronic Fatigue Syndrome, and Fibromyalgia: An Update, Journal of Chronic Fatigue Syndrome, 2006; 13:77-106.
(This phenomenon is analogous to the delayed post-exertional
pain and fatigue that can often be seen among healthy persons who do “eccentric contraction” muscle exercises at levels higher than usual. However, most likely, the mechanisms are different.)
A second aspect of the Post Exertional Flare-up Phenomenon
is that it’s severity and duration both tend to increase with repeated attempts to exceed the patient’s limits.
Thus a fibromyalgia or chronic fatigue syndrome patient who
pushes beyond their limits for 4 or 6 hours on one single day may have some degree of flare-up the next day. But if that same individual repeats the same activity for two days in a row, the symptom flare-up would typically be more severe and the duration of flare-up would typically be longer. All the more so if that activity were to continue to be pushed through e.g. for five days in a row—as in a work week.
The take home lesson here is that an individual who can perform at
a relatively high level for just a few hours might or might not have the
reserve and stamina to maintain that level of performance on a regular basis day after day and week after week. One subject can; another cannot. But, limited short term observations cannot tell us which is which.
However, there is objective basis for judging the credibility of the patient’s self-report and how, in fact, they live their lives. What is objective is the paper trail of medical records, the medical opinion of physicians, appropriate surveillance records and other information that increases or decreases confidence that the self-reports are accurate. This requires interpreting the data as it applies for each specific claimant. Current Functional Capacity Evaluation (FCE) protocols lack validity in the context of chronic fatigue syndrome and fibromyalgia. Unless, radically revised, FCE should not be used for CFS or FMS. Current protocols lack empirical and also theoretical rationale. Conclusions formed in this context are inherently flawed and misleading.
The FCE, as now used is not a reliable or valid measure for
evaluating the ability of persons with severe Chronic Fatigue Syndrome or Fibromyalgia to work on an ongoing basis--week after week and month after month. The research literature and common sense both make this clear.
The FCE, asks subjects to repeatedly perform light to moderately
intense physical activities for a short period of time. Typical tasks might include stooping, crawling, squeezing, balancing. This usually takes place over two to four hours. In somecase testing is repeated on the next day. The examiner then uses the findings over short periods of time to extrapolate out to a judgment about much longer periods. The examiner observes for just 4 ours over one or two days, but then extrapolates from this to predict how that person could do over a 40 hours week—week after week-- on a continuing basis in the context of a job.
This extrapolation is not valid, for two critical reasons 1. It lacks
face validity, because the FCE fails to evaluate precisely the main reason
that persons with CFS/FMS claims prevent them from working (the prolonged but delayed and cumulative worsening after unaccustomed exertion) and 2) there is no scientific, empirical research that support the validity of extrapolating from short term observations to long term ability to work.
Whatever applicability the FCE might or might not have for other
conditions such as angina, low back pain or emphysema, there has been no medical research that provides a reasonable basis for applying current FCE methods to fibromyalgia or chronic fatigue.
There are two main arguments against the use of current FCE
protocols to assess disability for persons with CFS or FMS: 1.The FCE self-consciously avoids evaluating directly assessing the specific limitations that most CFS/FMS patients give as the reasons that they are unable to work 2. There is no empirical medical research on chronic fatigue syndrome or fibromyalgia that in any way justifies or supports any extrapolation from a person’s ability to perform over a few hours to any conclusion at all about that person’s ability to perform for 40 hours every week.
First, let’s list the main reasons that persons with CFS and/or FMS
claim they cannot sustain themselves at a job. The most prominent are:
1) The person is too fatigued and limited in stamina to be able to
function for more than a few hours a day without their symptoms getting worse.
Comment: The FCE does not attempt to verify whether or not this historical claim is accurate or whether the person actually lives his or her life within these limitations. There is no
medical scientific basis for extrapolating from the short term testing to a prediction about the ability to perform for 40 hours every week.
2) The person is in too much pain and too limited in stamina to
function for more than a few hours a day without their symptoms getting worse.
Comment: The FCE does not attempt to verify whether this is true or whether the person actually lives his or her life within these limitations. There is no medical scientific basis for extrapolating from the short term testing to a prediction about the ability to perform for 40 hours every week.
3) The person has too limited an ability to concentrate, think rapidly,
and/or multi-task to sustain effective concentration on an ongoing basis. Attempting to do so further reduces cognitive abilities and increases symptoms of “brain fog” and/or pain and/or fatigue.
Comment: The FCE does not attempt to measure cognitive stamina. Nor would it be sufficient to measure cognitive ability over just one session. Since the issue is cognitive stamina, one has to measure whether,with repeated effort and compared to controls, cognitive test scores would increase, remain stable or deteriorate over time.
4) The person suffers a prolonged increase in symptoms some hours
or a day after they attempt to push past their physical activity limits.
Comment: This phenomenon, the post-exertional flare-up, is characteristic of FCE and CFS. It is not as prominent for other common forms of illness. This is a crucial difference between CFS/FMS and those health conditions that FCE testers and disability insurance physicians often encounter. Current FCE protocols make no attempt to learn how the patient fared in the
hours or days after the testing. A similar flare-up phenomenon can occur if patients push past their cognitive limits. By ignoring this central question, current protocols forfeit their face validity.
5) Patients often report that their worsening with exertion tends to
be cumulative. That is, five days of trying to push through causes much more severe and longer flare-ups than does just one day of over-doing.
6) CFS and FMS patients also report that, unpredictably, they have
days where they are even much worse than usual. Many report that on such “bad” days they can barely get out of bed. These unpredictable flare-ups are in addition to those that can be expected due to over-activity on prior days. Many report such especially “bad” days as occurring once or twice a week. If these reports are accurate, persons with frequent “bad” days would be unable to work regularly at a job just for that reason alone.
Comment: The FCE does not attempt to confirm or deny the “bad” day phenomenon.
Current FCE protocols simply ignore these issues. They make no
attempt to assess them. But, one cannot reasonably ignore the very issues that the claimant offers as the reason he or she can’t work. That is scientifically incorrect. This limitation forfeits the FCE’s claim to face validity. That is the method is invalid on its face, even before one gets to empirical testing. Simply put, the FCE as now used, is looking in the wrong place.
In practical terms, imagine an employer hiring someone with
chronic fatigue syndrome or fibromyalgia. Having interviewed on a “good day” the employer used a current FCE protocol and that it “predicted” that this person could sustain effective sedentary work function for 40 hours every week. Next, imagine that after three or four 8
hour workdays this employee had to call in sick as their stamina declined due to continuing effort. Would it be fair for such an employer to feel misled over the FCE results? Clearly the answer is Yes.
What empirical evidence underlies the FCE’s claim that measuring hand strength, squatting, balancing etc for a few minutes is relevant to an opinion about whether a person can work for 40 hours a week, week after week? Particularly, does any research support such extrapolations for the specific conditions, chronic fatigue syndrome or fibromyalgia?
The short answer is no. The rationale for this testing, when applied to CFS/FMS, is entirely speculative, and unsupported by evidence. To formally test this crucial question I ran a computer-assisted search of the National Library of Medicine medical literature data base, EntrezPubMed. PubMed contains more than fifteen million health journal articles. It contains essentially all English Language medical publications since 1966, and also a large number of foreign language publications.
Based on the National Library of Medicine’s data base there are no published controlled studies at all that support the validity of any currently standard FCE protocol as applied to chronic fatigue syndrome or fibromyalgia. By “no publications”, this means literally zero–not one or two publications, but literally zero.
On March 23, 2007 I submitted the keywords: functional capacity evaluation, FCE, fibromyalgia and chronic fatigue syndrome.
The keywords fibromyalgia and functional capacity evaluation
or FCE identified two single references. However, based on the abstracts of these articles–which are available on line--neither article
assessed the clinical relevance or validity of the FCE as a tool for evaluating FMS disability.
A search using the keywords chronic fatigue syndrome and functional capacity evaluation or FCE disclosed five articles. None of these articles provided evidence to support the validity of the FCE for patients with CFS. Indeed, their conclusions tended toward the contrary.
For Example consider Ross SD, Estok RP, Frame D, Stone
LR, Ludensky V, Levine CB. Disability and chronic fatigue syndrome: a focus on function Arch Intern Med. 2004 May 24;164(10):1098-107. Their conclusion states:
For questions of disability and employment in CFS, the limitations inherent in the current literature are extensive. Methodologically rigorous, longitudinal, and interventional studies are needed to determine baseline characteristics that are associated with the inability to work… Simple and consistent evaluations of functional capacity in patients with CFS are needed.
For example consider Nijs J De Meirleir K Wolfs S, Duquet W Disability Evaluation in chronic fatigue syndrome: association between exercise capacity and activity limitations/participation restrictions Clin Rehabil. 2004 Mar; 18(2):139-48.
CONCLUSIONS: These results suggest a moderate association between exercise capacity and activity limitations/participation restrictions in patients with CFS. The observed correlations lack strength to predict activity limitations/participation restriction based on exercise capacity parameters…
For example consider Barrows, D, Functional capacity
evaluations of persons with chronic fatigue immune dysfunction
system (Am J Occup Ther. 1995 Apr; 49(4):327-37.: Abstract: Chronic Fatigue Immune Dysfunction Syndrome (CFIDS) is estimated to affect 2 to 5 million people in the United States. Despite its high incidence, persons with CFIDS have been neglected by the medical community mainly because there is no singular confirming diagnostic test or proven effective treatment. The CFIDS population is incorrectly stereotyped as upper-middle-class, white, female hypochondriacs; consequently, symptoms often are belittled or ignored. In reality, CFIDS is a severe medical condition that affects women, men, and children of any race and often causes long-term or total disability. The results of a modified functional capacity evaluation developed by the author and completed on 86 persons with CFIDS between 1988 and 1990 confirm that this population has severe physical and cognitive disabilities that affect their professional, familial, and social lives.
Please note, this study used the authors’ own unique and newly
formulated FCE protocol. They did not assess or attempt protocols that are currently in use. Nor did they attempt validate their own protocol against a “gold standard” of actual work-place performance.
For example, consider Morriss, R et. al. Exploring the validity of the Chalder Fatigue scale in chronic fatigue syndrome Psychosom Res. 1998 Nov; 45(5):411-7.) The Chalder fatigue scale is widely used to measure physical and mental fatigue… We examined the constructs of the 14-item fatigue scale in a sample of 136 chronic fatigue syndrome patients… There were four factors of fatigue explaining 67% of the total variance. Factor 1 was correlated with subjective everyday cognitive difficulties, concentration difficulties, and a deficit in paired associate learning. Factor 2 was correlated with difficulties in maintaining sleep. Factor 3 was inversely correlated with grip strength, peak VO2, peak heart rate, and peak functional work capacity. Factor 4 was correlated with interview and self-rated measures of depression. The results support the validity of mental and physical fatigue subscales and the dropping of the "loss of interest" item in the 11-item version of the fatigue scale
This study did not address standard FCE protocols or attempt to
The fifth study in the National Library of Medicine data base was a
clinical trial for treating chronic fatigue syndrome with an antiviral medicine. It was not relevant to any current FCE protocols.
Therefore, so far as can be determined from the published medical literature, there are no published studies that even attempt to validate any of the currently used FCE protocols with regard to their validity for predicting disability among persons with FMS or CFS.
There are other problems as well, for example, the relevance of the
tests given to the actual demands of the jobs for which the claimant might qualify. Often, the tasks used in the FCE are only distantly related to those actually required for the job. For example, if a job requires sustained mental concentration and high level executive decision making, the ability to do that effectively over an 8 hour day and a 40 hour week is what needs to be tested. The ability to squat repeatedly over several minutes or the ability to sit upright for several hours misses the point.
Because the FCE as currently used does not attempt to evaluate the specific limitations that CFS and FMS patients claims makes them unable to work and because it lacks empirical medical research supporting its methods for extrapolating from short to long term—for these sufficient reasons FCE protocols should not be used for CFS or FMS.
Judging the validity of FCE for other disease conditions is beyond
the scope of this review. However, it is pertinent to this discussion that, even aside from CFS and FMS, the FCE has been the subject of major criticism.
For example, see Innes and Stroker’s internet essay on the more
general validity of work-related assessments (not focused on CFS or fibromyalgia). They concluded:
“As with reliability, most work-related assessments have limited evidence of validity. A number had insufficient evidence on which to base an assessment of the level of validity. Of those that had adequate evidence, validity ranged from poor to good.. There was, however, no instrument that demonstrated moderate to good validity in all areas. Very few work-related assessments were able to demonstrate adequate validity in more than one area…This highlights the need for further research to be conducted in this area. The acceptance of work-related assessments on the basis of their longevity in the marketplace and clinic should not be assumed to equate with adequate validity.. Or consider this study conducted by Liberty Mutual Research Institute for Safety Center for Disability Research. (Liberty Mutual Research is sponsored by Liberty Mutual, the insurance company.)
Pranksy G and Dempsey P Practical Aspects of Functional
Disability Evaluation J Occup Rehabil. 2004 Sep; 14(3):217-29.
Abstract: Physicians, employers, insurers, and benefits adjudicators often rely upon functional capacity evaluations (FCEs) to determine musculoskeletal capacity to perform physical work, often with legal or occupational consequences. Despite their widespread application for several decades, a number of scientific, legal, and practical concerns persist. FCEs are based upon a theoretical model of comparing job demands to worker capabilities. Validity of FCE results is optimal with accurate job simulation and detailed, intensive assessments of specific work activities. When test criteria are unrelated to job performance, or subjective evaluation criteria are employed, the validity of results is questionable…Evaluation of sincerity of effort, ability to perform complex or variable jobs, and prediction of injury based upon FCE data is problematic.More research, especially studies linking FCE results to occupational outcomes, is needed to better define the appropriate role for these evaluations in clinical and administrative settings.
Should we design an FCE protocol that actually observes patients
over a simulated 40 hour work-week? In some ways that might make sense, if such a protocol were then evaluated objectively against a “gold standard” of actual work performance on a job over the course of many months. However, based on our knowledge of FMS and CFS, this degree of vigorous testing would be expected to seriously exacerbate illness in a substantial subset of patients. This would create a medical hazard.
Conclusion: Current FCE protocols should not be used for assessing disability due to CFS or FMS. These protocols lack face validity, and have absolutely no supportive evidence in terms of peer reviewed articles published in the medical literature.
If the FCE is to be used at all for chronic fatigue syndrome or
fibromyalgia, it must first be redesigned and then validated by proper testing to repair its deficiencies.
Based on the merits of the medical science involved, it seems highly
unlikely that current FCE protocols could survive a Daubert challenge.
Both insurance carriers and the public would benefit from a decision
to abandon the current FCE and to develop better tools for evaluating disability for fibromyalgia and chronic fatigue syndrome. For insurance carriers to rely on a provably invalid method such as the FCE, this undermines public confidence in the insurance industry as a whole. In the long run, public confidence is requires to sustain a friendly environment of law and regulation so that insurance company’s can function and so that disability insurance policies will remain available to the public.
Since the FCE is Not Valid, What Tools Can We Use to Confirm or Deny a Patient’s Self Report that their stamina is so Limited That They Cannot Sustain the Activity Any Job Would Required for Forty Hours in a Work-Week?
evaluation of the credibility of the patient’s self-reports. While self-reports are, by definition, subjective—in that you can not look at a person and automatically measure the truth of his or her statements—objective evidence can and should be used to assess the self report’s credibility. Most often the most important method is a careful review of the medical records to see whether or not
a) complaints are documented over a long period of time are
b) consistent with the patient’s self-reports and
c) characteristic of the known pattern for CFS and FMS and
d) consistent with other independent evidence such as surveillance tapes or testimony.
In reviewing disability litigation cases, the defense sometimes
asserts that a claimant is not disabled because the evidence that the physician documents in the chart is “not objective”. This uses the term objective to mean that there should be an objective finding on physical exam or lab testing that demonstrates disease severity. As discussed above the criteria for CFS and FMS are such that normally we should not expect physical findings or lab tests to assess disease severity or to distinguish the patient who is disabled from the patient who can still work. This objective vs. subjective debate distracts from the valid question—Are the patient’s self reports of symptoms and limitations credible in view of the objective evidence available such as medical records, opinion of treating and expert physicians, independent testimony regarding actual life style, appropriate independent surveillance.
As discussed in prior sections we face a paradox. The patient’s
report is in one sense subjective i.e. based on the patient’s self-
report. But, it is also objective in the sense that these reports can be verified or denied objectively using medical records, testimony and independent observations to confirm or deny the credibility of the self-reports?
One reason for doubt an individual patient’s credibility might
be if the patient’s report is not consistent with the typical pattern of their disease. For example, it would be very atypical for a patient with FMS or CFS to feel typically 100% well and be highly active for weeks at a time, only to plunge back into severe illness for weeks at a time thereafter. Some variation in symptoms from day to day or month to month is typical but most often variation is modest. (Some CFS/FMS patients will refer to periods of being “almost normal”. However, they usually see this in comparison to a very low baseline. Close questioning will usually reveal that their energy reserves are still limited.)
Another reason for doubt might be information from the
patient spouse, or other observer claiming that the patient habitually engages in activities that are inconsistent with their self-reports. For example, persons with disabling fatigue and pain due to FMS/ CFS cannot typically play vigorous singles tennis three times a week on a consistent or regular basis. (Such activity might be tolerated once in a while, but would typically flare-up their symptoms later that day or the next.)
Another factor is the medical judgments of physicians who
know the patient well. Physicians who have developed a relationship with a patient will gain confidence in their medical opinion about the patient’s reliability. By and large we should prefer the long-term treating physician’s judgment about the patient’s credibility to that of a physician who has seen the patient only once, or, if an opinion is based just on a review of the file.
In some charts one can often sense from the physician’s note
whether or not the physician has substantial reservations about the accuracy or truthfulness of the patient’s self-reports. However, in other charts, we cannot tell.
One practical problem is that many physicians’ notes are not
very detailed. As important, the physician's main focus is most often on issues other than quantifying the severity of symptoms or functional impairment. Treating physicians tend to be much more interested in diagnosing and treating, than in asking about or writing down how long a person can sit in a chair or type on a keyboard.
Thus, a typical physician’s visit note might read something
Still tired and achy. Ultram helped, but had to stop due to nausea. Will send to PT and perhaps try Cymbalta.
This person’s illness could be mild, moderate or severe. One cannot
tell from this note. If specifically asked to, the physician might have chosen to direct questions toward assessing severity and function. However, in real world practice, other priorities take precedence. In an ideal world, physicians might directly quote the language of all their patients’ complaints. In practice, our notes are highly selective and condensed.
If there is little or no mention of functional limitations in the chart, one cannot necessarily conclude that function was normal or that no limitations were reported. Physicians may regard complaints about reduced function as more a vocational than medical concern. We’re normally more concerned about a host of other issues.
Another practical problem is that many physicians don’t know
enough about the normal pattern of fibromyalgia or chronic fatigue syndrome-- such as the post-exertional flare phenomenon. Clinical records are often silent, on what, in litigation, may turn out to be very important points.
We also face problems due to the patient’s limitations as a
communicator—e.g. limitations imposed by the duration of time allowed for a visit, the patient’s purpose for certain visits being unrelated to her FMS/CFS complaints.
Despite these limitations, the medical records remain the most
Beyond this, we could in theory consider other objective measures.
For example, insurance industry attorneys can ask to review a claimant’s credit card charges to construct a picture of the claimant’s activity levels. They might obtain records from the local golf course to see how often a claimant played. This is fair, since the insurance company does have a right to do all they can to learn whether or not a claimant is in fact living within the limits that they claim that they have.
Hidden video-surveillance is often used. This feels like an invasion
of privacy. Of course, in a sense it is. But, this is still a tool—if properly used—that can provide objective evidence of a claimant’s activity. Unfortunately, video surveillance can also be misused and misinterpreted.
Videotaping a person shopping for two or three hours on one day
with stooping down to take things off shelves, reaching up to put things back, of lifting packages in and out of a shopping cart—this should not be viewed as evidence that a patient can work a 40 hours week. A videotape of this kind is simply a less formal and planned version of the FCE. It provides no scientific basis for extrapolating out from a few hours of activity to any judgment at all about a 40 hours week. On the other hand, a video tape that shows vigorous activity 4 hours every day, five days a week, might reasonably be used to question a claimant’s claim. (But, this
works both ways. If there are four or five days of surveillance and all that is observed in that time are one or two trips to the store for shopping, this tends to support not deny the patient’s report of limitations.
Summary of Dr. Podell’s Background Related to Chronic Fatigue Syndrome and Fibromyalgia
Dr. Podell serves as clinical professor in the department of family
medicine, UMDNJ-Robert Wood Johnson Medical School. He is Board Certified in both Internal Medicine and in Family Practice. Chronic Fatigue Syndrome:
During 1998-2003 Dr Podell served as Principal Investigator for an
FDA approved phase III double blind trial of the drug, Ampligen, as treatment for chronic fatigue syndrome. Dr. Podell also served as Principal Investigator of an FDA approved open label study of Ampligen for chronic fatigue syndrome.
Dr. Podell was an editorial advisor for a monograph on the diagnosis
and treatment of chronic fatigue syndrome that was published in 2002 by the New Jersey Academy of Medicine and the New Jersey State Department of Health.
Dr. Podell participated in National Institutes of Health’s working
group on Chronic Fatigue Syndrome, 1993.
Dr. Podell is author of a book for patients about chronic fatigue
titled, Doctor Why Am I So Tired?, Fawcett, 1987. This was a Book-of-the Month Club Selection.
Dr. Podell has lectured on chronic fatigue syndrome to the Division
of Family Medicine, UMDNJ- Robert Wood Johnson Medical School, and other professional and lay organizations.
Dr. Podell received the Achievement Award for 2002 from
the New Jersey Chronic Fatigue Syndrome Association
Dr. Podell is a member of the Chronic Fatigue Syndrome
Association, the primary organization of health professional specialists in Chronic Fatigue Syndrome. Fibromyalgia:
Dr. Podell is the author of two review articles for physicians
Podell, R , Fibromyalgia: A Practical Guide for Diagnosis and Treatment, accepted for publication in the Journal of Musculoskeletal Pain, 2007
Podell, R, Fibromyalgia: Practical Treatments for the Family Physician, Perspectives, The Journal of the New Jersey Academy of Family Physicians pages 8-13, 4Q, 2005
Dr. Podell has lectured on Fibromyalgia before the Division
of Rheumatology at UMDNJ-Robert Wood Johnson Medical School and other lay and professional audiences.
Dr. Podell participated in the National Institutes of Health
Workshop on Fibromyalgia Research, National Institutes of Health, November, 2004
Dr. Podell is a member of the International Myopain Society,
the leading international professional organization of physicians and scientists specializing in Fibromyalgia. Dr. Podell participated in the three most recent Scientific Assemblies of the International Myopain Society.
Disability And Chronic Fatigue Syndrome or Fibromyalgia:
Dr. Podell served as invited medical expert consultant on
Chronic Fatigue Syndrome and Fibromyalgia for both the Seventh, Eighth and Ninth National Advanced Forum on Litigating Disability Insurance Claims presented by the American Conference Institute in 2005, 2006 and 2007.
Wissenschaftliche Publikationen Auswahl seit 1993 aus über 900 Veröffentlichungen 1. Spengler et al. : Differential signal transduction patterns of five splice variants of the PACAP receptor. Nature 365: 170-175 (1993) 2. Rupprecht at al. : Progesterone receptor mediated effects of neuroactive steroids. Neuron 11: 523-530 (1993) 3. Trapp et al. : Heterodimerization between mine
4 Antimicrobial Susceptibility Testing for the accurate determination of the minimum inhibitory concentration (MIC) of a test organism to an antimicrobial Antimicrobial Concentration Pack Size Product Code range µg/ml Amoxycillin Amoxycillin/clavulanic acid Ampicillin Cefotaxime Cefotaxime Ceftriaxone Ciprofloxacin NEW Clindamycin Erythromy
 patient must report pain, not just tenderness. Examine pressing with the thumb using a force that just makes thumbnail blanch. Tender point counts can vary from day to day. Psychological distress makes tender points more painful. A person who has chronic widespread pain but < l1 of 18 tender points meets the definition for chronic pain syndrome. Technically, fibromyalgia is a sub-class of chronic pain syndrome
Please note: The formal definition of fibromyalgia
provides no guide to assessing disease severity or disability.
One can be disabled from fibromyalgia despite having only 11 positive tender points on a given day. Or one might be able to work despite having 18 out of 18 positive tender points. In principle, one can be disabled due to chronic pain syndrome, even when it does not meet the definition of fibromyalgia e.g. if there is severe, widespread pain but with only a few positive tender points.
Other than tender points there are no objective finding
patient must report pain, not just tenderness. Examine pressing with the thumb using a force that just makes thumbnail blanch. Tender point counts can vary from day to day. Psychological distress makes tender points more painful. A person who has chronic widespread pain but < l1 of 18 tender points meets the definition for chronic pain syndrome. Technically, fibromyalgia is a sub-class of chronic pain syndrome
Please note: The formal definition of fibromyalgia
provides no guide to assessing disease severity or disability.
One can be disabled from fibromyalgia despite having only 11 positive tender points on a given day. Or one might be able to work despite having 18 out of 18 positive tender points. In principle, one can be disabled due to chronic pain syndrome, even when it does not meet the definition of fibromyalgia e.g. if there is severe, widespread pain but with only a few positive tender points.
Other than tender points there are no objective finding