Liver transplantation for children – the red cross children's hospital experience
Pediatr Transplantation 2004: 8: 136–144
Liver transplantation for children – the RedCross Children’s Hospital experience
Millar AJW, Spearman W, McCulloch M, Goddard E, Raad J,
Rode H, Kahn D, Cywes S. Liver transplantation for children – the
Red Cross Children’s Hospital experience.
Pediatr Transplantation 2004: 8: 136–144. Ó 2004 Blackwell Munksgaard
Department of Paediatric Surgery, Paediatrics,Medicine and Surgery, Red Cross Children's Hospital,
Abstract: Liver transplantation for infants and children has been
Institute of Child Health and Medical Research
available in South Africa at a single centre, the only established service
Council Liver Research Centre, University of Cape
in Sub-Saharan Africa, for more than a decade. Current concerns have
shifted from an initial target of early post-transplant survival to qualityof life in the long-term. Materials and methods: Since 1985, 225 infantsand children have been assessed, with 146 accepted for transplantation. Sixty-nine have had 71 orthotopic liver transplants (OLTx). Biliaryatresia was the most frequent diagnosis (54%) followed by acute liverfailure (ALF) (15%). Waiting list mortality has remained high (23%),particularly for the ALF group (50%). Forty-three were reduced sizetransplants with donor: recipient weight ratios ranging from 2:1 to 11:1. Twenty-seven were <10kg. Results: Fifty (74%) survive 1 month–12 years post-transplant. Actuarial survival after 1996 since HBV coreantibody positive donor livers were refused and prophylactic IVganciclovir used has been >82%. Early post-OLTx mortality was low(5%), one primary non-function, one IVC thrombosis, one PV throm-bosis, but late morbidity and mortality (20%) was mainly due to viralinfection: de novo hepatitis B (five patients, three deaths), EBV-relatedpost-transplantation lymphoproliferative disease (PTLPD) (eightpatients, six deaths) and CMV disease (11 patients, five deaths). Tuberculosis prophylaxis, required in six cases, resulted in majormorbidity in two and mortality in one. Poor compliance played a sig-nificant role in seven deaths. Hypertension requiring medication along
Key words: liver transplantation – children – South
with some compromise of renal function has been present in all but two
Africa – tuberculosis – hepatitis B – Epstein–Barr
patients. However, all those of school-going age (25) attend school
virus – cytomegalovirus – human immunodeficiency
normally and remain in good health and only three of the survivors
have abnormal liver function tests. Conclusions: Successful liver trans-plantation is possible in a developing country with limited resources.
A.J.W. Millar, Red Cross Children's Hospital,
Scarcity of virus-free donors (HBV and HIV) leading to waiting list
University of Cape Town, Rondebosch 7700, CapeTown,
mortality and infrequent re-transplantation along with long-term
consequences of immunosuppression (infection, lymphoma and renal
toxicity) remain problems. Intense education of the caregiver and
close follow-up, particularly of those living at long distances haspartly addressed the compliance problem.
Accepted for publication 30 September 2003
During the early and mid-1980s several SouthAfrican children with end stage liver disease weresent abroad to the USA and UK at great
Abbreviations: AZA, azathioprine; CMV, cytomegalovirus;
expense, the money in most cases being raised
CyA, cyclosporin A; EBV, Epstein–Barr virus; HBV,
by public appeal. It was during this time that
hepatitis B virus; HIV, human immunodeficiency virus;
preparations were made to develop liver trans-
INH, isoniazid; IVC, inferior vena cava; OLTx, orthotopic
plantation for children at the Red Cross Chil-
liver transplants; PCR, polymerase chain reaction; PTLPD,post-transplantation
dren’s Hospital, Cape Town. The first children
portal vein thrombosis; TB, tuberculosis.
were accepted on to a transplant waiting list as
psychosocial factors (parental substance abuse, psychiatric
problems), rarely socio-economic factors and parental
decision, but most importantly poor compliance with pre-
operative therapy. Compliance was most difficult to predictin children with acute hepatic failure as time from presen-
tation to transplant was so much shorter. Indications for
early transplant were evidence of poor synthetic liver func-
tion including prolonged prothrombin time, low serumalbumin and cholesterol, presence of ascites, bleeding from
oesophageal varices not controlled by sclerotherapy and
failing nutritional status (3, 7, 8). Those with acute hepatic
failure who developed encephalopathy, hypoglycaemia, aprothrombin time of greater than 100 s, and factor five level
less than 20% were considered for transplant, as almost alldie without transplantation. There were few medical contra-
Fig.1. Geographical origin of all patients, referred for
indications, however children with disseminated TB, severe
consideration for liver transplant since 1985.
cardiac, renal or pulmonary disease, marked neurologicalimpairment, chronic Hep B infection and HIV infectedpatients were not accepted. All patients accepted underwent
early as mid-1985. Since then 225 children have
intensive medical and nutritional resuscitation to treat
been referred for assessment (Fig. 1). The first
complications of liver disease, portal hypertension and
transplant took place on 6 December 1987 on a
nutritional deprivation (3, 10). Immunization status was
6-yr-old girl with end stage liver disease and
reviewed and supplemented with Hepatitis A and B, Hinfluenza and pneumococcal vaccine in most cases. The
cirrhosis from alpha I anti-trypsin deficiency.
decision as to which waiting list patient to transplant was
The patient survived the operation but died from
taken at the time a donor presented. In principle, the sickest
complications in January 1988. A successful
patient was transplanted first with a blood group compat-
adult programme was commenced during that
ible donor but also taken into account was the best possible
year at Groote Schuur Hospital and when this
use of the donor organ. This resulted in some patients
had become established, the paediatric pro-
remaining on the waiting list until their medical conditionhad deteriorated to the extent that they were considered too
gramme was restarted in November 1991 (1).
sick to withstand the transplant operation. Of the 146
Liver disease has been generally underestima-
children accepted, 33 have died prior to transplant (23%).
ted as a cause of death in children in South
These included 17 with biliary atresia and nine with acute
Africa as elsewhere. This is probably because
hepatic failure. Most of the biliary atresia deaths occurred in
many liver conditions in children have led to
the early years of our programme, current waiting list
rapid deterioration and death in the past (2).
At the time of writing, of the 32 children accepted and
However, it has taken at least a decade of hard
awaiting transplant only 14 are considered urgent cases. The
work to publicize amongst medical colleagues the
others have established liver disease but 18 are in good
fact that in most cases the only chance of a cure is
health at present and would not be transplanted until
liver transplantation and that this service was
deterioration of growth velocity or complications became
available locally (3). Also, that, liver transplan-
evident. Six patients have had transplants abroad, three in
tation should be considered as an option for
USA and three in the UK, four of whom survive, 5 monthsto 17 yr after transplant.
chronic liver disease before the condition of endstage liver disease is realized; thus allowing time
for a thorough assessment of the child and thefamily, for full and frank discussions of treat-
The surgical techniques used for donor retrieval and
ment options and assessment of the family’s
recipient liver removal and engraftment have been previ-ously described in detail (1, 4, 5). Because of donor recipient
capacity to sustain long-term compliance after
height and weight mismatch, reduced sized livers have been
transplantation, which is so crucial to the success
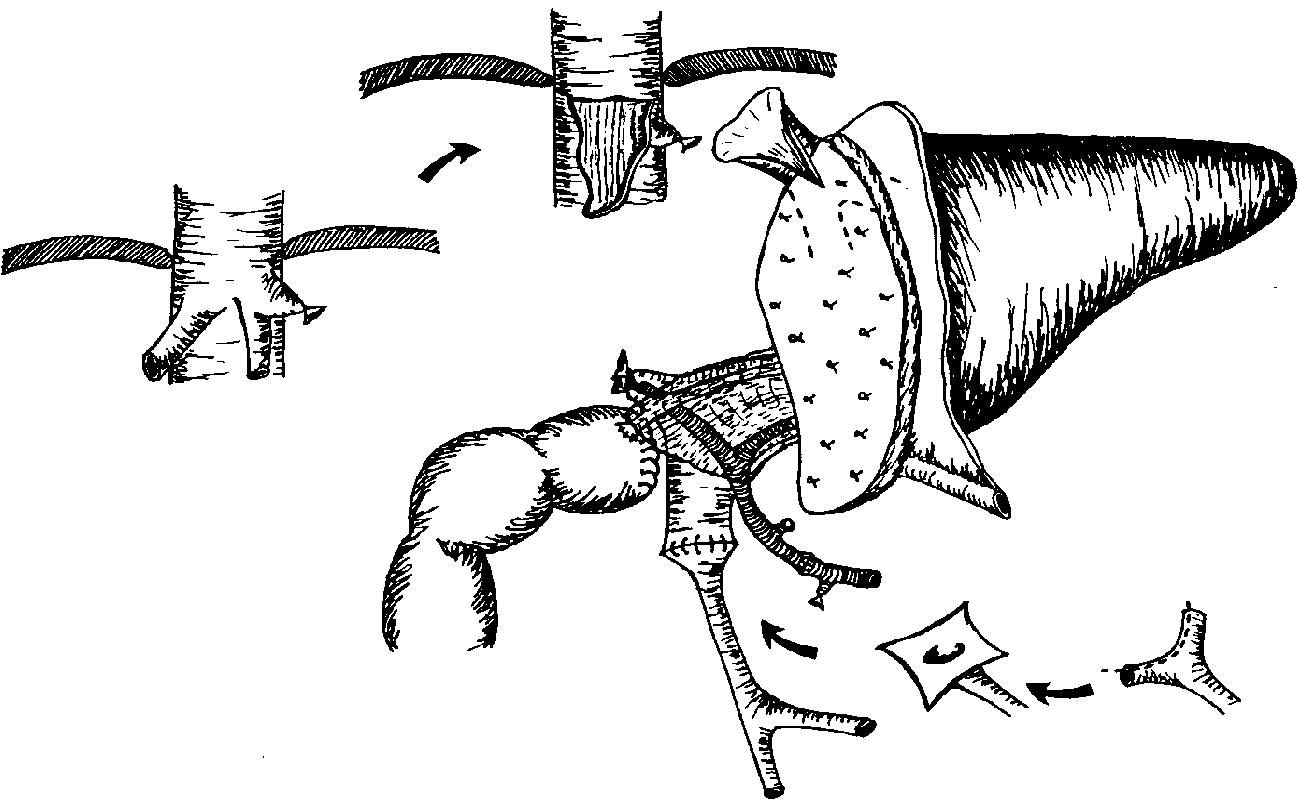
used since 1992 (Fig. 2) (11). With all reduced size livers and
in patients with biliary atresia, choledochojejunostomy hasbeen used for biliary drainage without stents or T-tubes. In
most cases of reduced size grafts, the hepatic venous outflowwas anastomosed to the preserved recipient inferior vena
Since 1985, 225 children have been referred to our unit for
cava with a large, flush, triangular anastomosis to avoid
assessment for transplantation. Initially they predominantly
venous outflow obstruction (Fig. 2) (12). To overcome the
came from the Western Cape Province and were few but
disparity in size of the often small and hypoplastic recipient
numbers have increased over the last 6 yr, on average 16
portal vein, the right and left bifurcation of the recipient
referrals a year, with a greater proportion coming from
vein was preserved and opened to make a trumpet-shaped
elsewhere in South Africa (Fig. 1). In addition, several
orifice to anastomose to the larger donor portal vein or else
families have migrated from other provinces so that they
the anastomosis was done at the confluence of the splenic
could be managed before and after transplantation in close
and superior mesenteric veins (13). The arterial anastomoses
proximity to our centre. Of these 225 patients, 146 were
were in most cases from the recipient common hepatic
accepted for transplant. Reasons for refusal included
artery to the base of the donor coeliac trunk. The various
Right and middle hepatic veins opened. Left sutured or ligated.
IVC incised inferiorly and donor hepatic vein sutured onto this
opened at bifurcationand sutured to donor
Connective tissue sheath and bloodvessels supplying the hepatic ducts leftundisturbed to preserve blood supply
Fig.2. The surgical technique of a left lateral segment reduced size liver transplant.
types of interposed grafts described in other series were not
instead of AZA in three patients because of persistent
used in any of our cases. Crucial to the success of the
rejection with conventional therapy and rapamycin has been
operative procedure was good anaesthetic support (14, 15).
used in two patients with chronic rejection and high EB viruslevels. In the last 2 yr anti-CD25 antibodies have been used
weight < 20kg, daclizumab 1 mg/kg/dose) both as a two
dose regimen (20). Later conversion from cyclosporin totacrolimus was prompted in a few cases because of cosmetic
CyA (5 mg/kg) was given immediately prior to the operation
side effects of gingival hyperplasia and hirsutism.
and was continued in the post-operative period initiallyintravenously but since 1997 as an oral dose using cyclosp-orin emulsion (Neoral) (Novartis), given as a three times a
day dosage aiming for a trough level of around 350ng/mLinitially and currently a 2 h peak level of >1000 ng/mL (17–
Fungal prophylaxis was given prior to transplant as
19). Dosage was adjusted frequently in the post-operative
mycostatin orally and after transplant, amphotericin B
period as particularly in small children, absorption was er-
lozenges were added and continued over a period of several
ratic with diarrhoea and rejection and low CyA levels being a
months. Infants in poor condition with prolonged pre-
recognized association. AZA (1–2 mg/kg) and methyl-
prednisolone (10mg/kg) were given at the time of reper-
amphotericin for 2–3 wk. From 2–3 wk after transplant for
fusion of the graft. The methylprednisolone doses were
at least the first year, trimethoprim/sulphamethoxazole was
reduced over the first week to 1 mg/kg for the first month
given at a dose of 6 mg/kg a day in two divided doses 3 days
and then further reduced to a level of 0.2 mg/kg as main-
a week for prevention of pneumocystis carinii infection. As
tenance. This was later reduced in some patients to alternate
oral therapy has been found to be less effective, intravenous
day therapy or even withdrawn. The AZA dose 0.5–1 mg/kg
gancyclovir 5 mg/kg per dose 12 hourly was given as viral
was monitored keeping the leukocyte count above 4000/mm
prophylaxis against CMV and EBV infection, initially for
(2) and was continued for at least 6 months. Tacrolimus was
2 wk but currently this is continued for up to 3 months in
used as rescue therapy if an acute rejection did not respond
high risk patients not previously exposed to EBV in an
to three or four daily pulses of methylprednisolone
attempt to prevent post-transplantation lymphoproliferative
10mg/kg/dose and recently with compatible but not
disease (PTLPD). (25) Either hyperimmune CMV globulin
identical blood types. Mycophenolate mofetil was used
or immunoglobulin in the form of Polygam (Natal Blood
Transfusion Service) was given to assist viral prophylaxis.
Leucocyte filtered blood products were used since 1995 toreduce CMV viral load. Prophylactic antibiotics were given
with induction of anaesthesia and continued for 3–5 days.
Since 1991, 71 transplants have been carried out
These were changed according to cultures taken of blood,secretions, sputum and urine. Anti-TB prophylaxis was
on 68 patients of whom 46 were black and 22
given only if the reason for transplant was a reaction to anti-
white (Fig. 3). Thirty-three were female and 25
TB drugs, where evidence of TB was found prior to surgery
male. The mean weight was 18 kg with a range of
or if close family contact was recorded. Ofloxacin,
4–53 kg. Twenty-five were less than 10kg in
rifampicin and ethambutol or ethionamide was used in
weight (37%). The mean age was 5.3 yr with a
addition to INH but very careful monitoring of liver func-tion tests was required because of both drug induced hepatic
range of 6 months to 14 yr. Patient diagnoses
toxicity and decrease in levels of cyclosporin or tacrolimus
and survival are listed in Table 1. There were
due to enzyme p450induction with increased drug meta-
three retransplants, one for acute fulminant
rejection and two for chronic rejection. Themean anaesthetic time was 10h with a range of
7–16 and the mean volume of blood transfused
Post-operative management was according to protocol (3,
was 2.5 blood volumes with a range of 0.5–5.7.
28). Patients were usually weaned off the ventilator within
Blood group crossmatch was identical in 53,
the first 48 h. Liver ultrasound with a colour flow doppler
compatible in 15 and blood group B to O in
was performed frequently to confirm vascular patency and
three. The mean donor liver ischaemic time was
absence of biliary dilatation. Liver biopsies were performed
8 h with a range of 5–16 h. Reduced size liver
if indicated by increasing serum liver enzyme activity or
transplants were performed on 42 occasions,
bilirubin levels by means of the Menghini technique [Hep-afix needle (Braun) diameter 1.4 mm] unless biliary dilata-
which included the left lateral segment in 23, the
tion was observed on ultrasonography. Biopsies were
left lobe in 15 and the right lobe in four. Donor
routinely assayed for viral and bacterial activity.
recipient weight ratios averaged 3.4:1 with a
Diagnosis of rejection was made on the basis of clinical,
range of 2:1 to 11:1. Three patients received a
biochemical and histologic criteria (29). The grade of
whole liver and a kidney graft for primary
rejection was according to established histologic criteriabeing graded from 0to 4. Rejection was treated with four
hyperoxaluria in two, and polycystic disease in
doses of methylprednisolone 10mg/kg, the first three on
one. We have performed one living related
successive days and then the fourth dose on the fifth day
after commencing treatment. If rejection persisted, the
All patients survived the operative procedure.
immunosuppressive protocol was changed to tacrolimus at a
Currently, of the 68 patients transplanted, 50
starting dose of 0.3 mg/kg per day in two divided doses to
survive (74%), 2 months to 12 yr post-trans-
obtain a trough level of 10–15 ng/mL initially.
Hypertension, which was present in all of our patients was
plant. Forty-seven of these are in excellent health
managed initially with nifedipine as required in conjunction
(Fig. 4). Three have persistent liver dysfunction
with diuretic agents and subsequently enalapril or amlodi-
pine in the appropriate dosage (30). Aspirin 3 mg/kg was
convalescing after recent transplant. The causes
given on alternate days as prophylaxis against hepatic
and timing of deaths are listed in Table 2 and can
arterial thrombosis along with sucralfate initially and lat-
be divided into those occurring early after
terly omeprazole for gastric mucosal protection (31).
Nutrition and vitamin supplementation was commenced
transplant which were predominantly related to
usually within 72 h of surgery and was supplemented by
the operative procedure itself and those occur-
nasogastric feeding or parenteral nutrition in the early phase
ring later on, which were predominantly due to
if there was delay in restoration of bowel function. Mag-
the consequences of immunosuppression or of
nesium and phosphate deficiency required replacement
immunosuppressive failure but in one case of
Table 1. Primary diagnosis of recipients from 1991 to 2003. Sixty-eight patients
Table 2. Current status of transplant patients 1991–2003, n ¼ 68
requiring 71 transplants with 50 surviving (74%)
PTLPDs (n ¼ 6)Chronic rejection (n ¼ 2)
bleeding oesophageal varices, the consequence ofa PVT which occurred shortly after transplant.
sion and subsequent uncontrollable bleeding
varices 6 months post-transplant. Two other bile
Fortunately these have been relatively few. Hep-
leaks occurred. The first patient developed a bile
atic artery thrombosis occurred on one proven
leak on the 8th day post-surgery which was
occasion and one suspected. The first patient
successfully repaired and another reduced size
developed a bile leak 1 month post-transplant,
liver transplant had bile stained ascites, which
which was successfully treated with revision
resolved spontaneously. Two patients developed
IVC thrombosis, the first, 6 months post-trans-
child, an infant of under 10kg in weight, devel-
plant probably secondary to chronic rejection and
oped fulminant hepatic failure 3 wk post-trans-
enlargement of the donor graft with distortion of
plant and no cause was identified. The hepatic
the IVC anastomosis. The second developed an
artery was seen to be pulsating on ultrasound.
IVC thrombosis in the immediate post-operative
Post-mortem examination was refused. Histology
period shortly after an acute rejection episode,
of a needle biopsy showed a massive fallout of
which had resulted in significant graft swelling.
liver cells, which was in keeping with either an
Both patients were treated with thrombolytic
ischaemic, toxic or viral injury. PVT occurred on
therapy, the first successfully but the second
three occasions, two of which were repaired
developed significant bleeding from the cut edge
successfully and the third led to portal hyperten-
of the reduced size graft and sepsis and died
Fig.4. Pediatric liver transplan-tation: cumulative proportion
surviving (Kaplan–Meier), Nov1991–1995 vs 1996–2003. The
1996 – Aug 2003 (n = 47)
divided into those receivingtransplants before 1996 and
after. Current expected 5 yrsurvival is >80%. Nov 1991 – 1995 (n = 22)
shortly after. At post-mortem, however, there was
which was described as polyclonal in four,
no visible thrombus in the vena cava. Post-
monoclonal in two and T-cell lymphoma in two.
operative gastrointestinal bleeding occurred in
Management strategies included adenotonsil-
three patients. One ceased spontaneously, an-
lectomy, reduction of immunosuppression and in
other required laparotomy and was found to be
two complete withdrawal (24, 25). Three received
bleeding from the Roux-en-Y anastomotic site
chemotherapy and these three died within 10wk
and the third bled uncontrollably from a large
of diagnosis. Three died despite significant
ulcer in the lower oesophagus secondary to
pretransplant sclerosant injection for control of
patients have made a complete recovery although
one required retransplant for chronic rejectionafter total immunosuppression withdrawal. Thusoverall there was a 14% incidence of PTLPD
with a 75% mortality. Currently, pre-emptive
Most could be discharged from the intensive care
intravenous gancyclovir therapy given for at least
unit within the first week after transplantation
3 months to high risk children and PCR viral
although in practice this was delayed because
monitoring only available in the last year, has so
logistical problems of a full surgical ward.
far been effective management (23, 25).
Bacterial infection in the post-transplant period
Hepatitis B de novo infection has occurred in
was frequent but had surprisingly little morbidity
five children and resulted in three deaths.
and only one suspected mortality. The only
Although not proven, these almost certainly
systemic fungal infection was the first transplant
were acquired from the donor liver as prior to
in 1987 who died of a ruptured mycotic (Can-
1996 donor livers were not tested for HBV core
dida) aneurysm at the hepatic arterial anastomo-
antibody and since excluding HBV core antibody
sis. Minor skin infections have been frequent and
positive donors, we have not seen a case (35). Of
have been treated with local anti-fungal agents
these five patients, three developed HBV hepati-
and fluconazole. Viral infections, however, have
tis post-transplant and have died of severe
been a problem with major morbidity and late
progressive chronic active hepatitis. The other
mortality (25, 30, 32–34). CMV is endemic in our
two survivors have responded very well to anti-
population and 90% of donors carried the virus
viral therapy using initially famciclovir and
(34). CMV disease occurred in 11 patients (13
currently, lamivudine with reduction of HBV
transplants) and CMV infection in a further 12.
Five of 11 patients with CMV disease died. The
below recordable levels (32, 36, 37). One patient
site of the CMV disease was the lung in four,
however escaped initial control and being poorly
liver in seven and pancreas and gastrointestinal
compliant, developed DNA levels in excess of
tract in one each. Initially the diagnosis was
made using serology and cultures but from 1995,
All children have received some form of anti-
the CMV PP65 antigen test became available.
hypertensive therapy in the post-transplant per-
Particularly at risk were patients with poor
iod. As a degree of renal impairment is almost
clinical status prior to transplantation and those
inevitable with patients suffering from severe
who required steroid pulses for more than one
chronic liver disease and with the additional
rejection episode. EBV infection has also resulted
burden of use of the nephrotoxic calcineurin
in significant morbidity and mortality. Ten chil-
inhibitors, cyclosporin and tacrolimus for immu-
dren developed EBV infection and eight subse-
nosuppression, most children continue to require
quent PTLPD. All were transplanted for biliary
at least one anti-hypertensive agent (30). When
atresia following a failed Kasai procedure. The
the doses of steroids were reduced and cyclosp-
development of PTLPD in five patients followed
orin and tacrolimus levels were allowed to settle
a typical acute membranous tonsilitis with asso-
to the lower therapeutic range, less anti-hyper-
ciated cervical lymphadenopathy. Mean time to
development of PTLPD in these children was
All surviving children of school-going age (25)
9.2 months, with a range of 3–30months post-
attend school normally and participate in normal
transplant. Three of the eight children were EBV
sporting and recreational activities. Three chil-
nuclear antigen positive at the time of transplant
dren transplanted for biliary atresia, have learn-
and all were positive at the time of diagnosis of
ing difficulties and attention deficit disorder and
require special schooling but are physically fully
included four tonsillar, one intestinal, two gas-
rehabilitated (38). All eight children transplanted
trointestinal tract and one central nervous system
for fulminant hepatic failure made a complete
involvement. Histology confirmed the diagnosis,
neurologic recovery after transplant.
The overall cumulative 5 yr survival is around
recent years. The premorbid clinical state had
60% but the projected survival since 1996 when
significant detrimental impact on the subsequent
aggressive anti-viral prophylaxis was started
outcome following surgery (3, 7, 8, 41). The
along with exclusion of HBV c AB +ve donors
increasing evidence that patients with cholestatic
and a more pro-active follow-up programme is
liver disease early on in life have nutritional
deficiencies which render them at risk for neuro-developmental impairment was confirmed being
present in four of our longer-term survivors (38,42). There is thus a need for earlier referral and
Careful planning, extensive preparation of per-
transplantation in these children. We have made
sonnel and a broad base of skills along with
it an absolute requirement that any patient
excellent team work between adult and paediatric
referred would need caring health professionals
health professionals allowed for the development
to take on the responsibility of looking after that
of a successful paediatric transplant programme
patient on return to his/her home following
(3–5). Further improvements in surgical tech-
successful transplantation. Current methods of
nique, anaesthetic skills, medical care and immu-
improved management and long-term follow-up
projected 5 yr survival to greater than 80% and
much longer survival in good health is clearly
Endemic viral and bacterial infections partic-
possible and should become the norm in the
ularly CMV, EBV and TB have had a significant
future. These results are equivalent to other
negative impact on our programme (32–34, 36,
reported series (39, 40). However, liver trans-
43). Specifically the strategies of anti-viral pro-
plantation remains an extremely demanding
tection have required extended hospital stay and
surgical procedure with many potential early
are clearly expensive, but fortunately seem to be
and late complications (41, 42). Most of the
effective in preventing CMV disease and the
serious complications occurred in the first few
consequences of EB virus infection or reactiva-
months after operation and many of these could
have been avoided with meticulous attention to
Hepatitis B acquired after liver transplant is a
technical detail and intensive prophylactic meas-
tragic occurrence and in our experience is not a
ures. The regrettable need for immunosuppres-
benign disease. Evidence that most were acquired
sive therapy with all its consequences along with
from HBV core antibody positive donors is
immunosuppressive failure still remain major
overwhelming. One published series quotes a
stumbling blocks to an uneventful post-operative
greater than 80% conversion rate (35). In two of
course. After the first few months post-transplant
our five patients anti-viral therapy has been
complications usually resulted from immunosup-
effective in reducing viral DNA levels but eAg
pressive therapy whether this was infection,
remains positive in both (37). Since 1996, when
usually viral, or from the toxic effects of the
we introduced HBV core Ab screening for liver
drugs themselves (30). All three children receiv-
transplants we have not seen a further case.
ing liver and kidney grafts have done well. One
TB with its very high endemic incidence in the
older child (10yr) with hyperoxaluria continues
South African population (150–200 per 100 000)
to receive overnight hydration via button gas-
is a constant hazard to any immunosuppressed
trostomy. The one child transplanted for mult-
child. Careful screening of the child and family
isectoral hepatoblastoma had portal vein tumour
pretransplant is necessary. Prophylaxis or full
treatment can be successfully carried out but
apparent complete surgical clearance developed
hepatotoxicity and markedly reduced cyclosporin
multiple hepatic metastases 3 months post-trans-
levels which may require up to five times increase
plant. Her tumour showed evidence of vascular
in dosage are potential dangers and should be
invasion on histology and did not respond well to
cisplatinum and adriamycin chemotherapy. At
The costs of our transplant programme are
the time of writing, she has an enlarging liver and
difficult to quantify but detailed costing of some of
no further anti-tumour therapy is contemplated.
our patients has indicated that an uncomplicated
Patients have been referred from all over South
transplant costs in the region of 20 000 US$ for the
Africa and clearly this dislocation from family,
first 3 months and thereafter approximately 500–
friends and workplace has had major emotional
1000 US$ per month for the first year. The costs of
and financial implications. Initially referrals fre-
immunosuppression medication are significant
quently occurred when the child was in very poor
but decrease, as smaller doses are required.
condition, however this has been less frequent in
Complications after transplantation and retrans-
receiving liver transplants is likely to increase.
plantation become very expensive thus we have
There will thus be an increasing need for a wider
attempted to transplant those children who would
involvement of local medical and surgical teams
likely benefit most from the procedure. This has
and perhaps the development of other transplant
meant in some instances that patients on the
centres in South Africa to cater for this demand.
waiting list in a poor medical condition have been
As with any new development, knowledge and
overlooked in favour of those in better health but
experience improves, costs decline, application
still with irreversible liver disease. Also retrans-
increases and success is ensured (51).
plantation has rarely been an option because ofdonor scarcity. Compliance with regard to medi-
cation and follow-up is an absolute requirementfor success. This is easier to predict pretransplant
The support and enthusiasm of our anaesthetic and medicalcolleagues and nursing personnel is greatly appreciated.
in those with chronic liver disease than those who
They have been an integral part of the transplant manage-
present with fulminant hepatic failure. Poor socio-
ment team from the commencement of the programme.
economic status has never been a contra-indica-tion to transplantation and we have been
frequently impressed by parents with relativelypoor material resources who have been able to
1. Robson SC, Spearman CW, James MF et al. Orthotopic liver
diligently care for their children. The value of a
transplantation at Groote Schuur Hospital. S Afr Med J 1992:
sympathetic social worker to provide support for
2. Lloyd-Still JD. Impact of liver transplantation on mortality
distressed families cannot be overstated.
from pediatric liver disease. J Pediatr Gastroenterol Nutr 1991:
The need for paediatric liver transplants has
been assessed at approximately one to two
3. Whitington PF, Balistreri WF. Liver transplantation in
children per million per year and this would
pediatrics: indications, contraindications and pretransplant
mean 20–30 transplants per year being required
management. J Pediatr 1991: 118: 169–177.
4. Starzl TE, Demetris AJ, Van Thiel D. Medical progress:
in South Africa (4, 5). In practical terms, this
liver transplantation part I. N Engl J Med 1989: 321: 1014–
would be possible but clearly financial resources
need to be allocated to such an endeavour. In
5. Starzl TE, Demetris AJ, Van Thiel D. Medical progress:
recent years, more than 60% of children referred
liver transplantation part II. N Engl J Med 1989: 321: 1092–
for transplantation come from outside of the
Western Cape Province without at present any
6. National Institute of Health Consensus. National Institute of
Health Consensus Development Conference Statement: Liver
strategies in place to compensate the Western
Transplantation 20–23 June 1983. Hepatology 1984: 4(Suppl. 1):
Cape Provincial Government and our centre for
the costs involved. These costs are, however, very
7. Paradis KJG, Freese DK, Sharp HI. A pediatric perspective
much less than those required for a South
on liver transplantation. Pediatric Clin N Am 1988: 35: 409–
African child to receive a transplant overseas
and it is distressing to still occasionally observe in
8. Balistreri WF. Transplantation for childhood liver disease.
An overview. Liver Transpl Surg 1998: 4: 518–523.
the media of money being raised for this purpose
9. Tan KC, Mondragon RS, Vorgas V et al. Liver transplan-
when the facilities are available locally at one-
tation for fuliminant hepatic failure and late-onset hepatic
failure in children. Br J Surg 1992: 79: 1192–1194.
A most serious issue currently facing all
10. Kelly DA. Nutritional factors affecting growth before and
transplant physicians, and we are no exception,
after liver transplantation. Pediatr Transplant 1997: 1: 80–84
11. Bismuth H, Houssin D. Reduced size orthotopic liver graft in
is the major shortfall in donor organs needed to
hepatic transplantation in children. Surgery 1984: 95: 367–370.
meet current demand. This is compounded in our
12. Emond JC, Heffron TG, Whitington PF, Broelsch CE.
Reconstruction of the hepatic vein in reduced size hepatic
increasing prevalence of HIV in the donor pool
transplantation. Surg Gynaecol Obstetr 1993: 176: 11–17.
with current HIV infection rates in the 15–40yr
13. Strong R, Ong TH, Pillay P et al. A new method of seg-
age group estimated at around 20–40%. This has
mented orthotopic liver transplantation in children. Surgery1988: 104: 104–107.
to some extent been alleviated for children by use
14. Chapin JW, Newland MC, Hurlbert BJ. Anesthesia for liver
of reduced size livers (44, 45). As the numbers
transplantation. Semin Liver Dis 1989: 9: 195–201.
waiting for adult transplants becomes greater, we
15. Davis PJ, Cook DR. Anesthetic problems in pediatric liver
will have to proceed with more frequent living
transplantation. Transplant Proc 1989: 21: 3493–3496.
related donation (45–47). At present, split liver
16. Jordan SC, Rosenthal P, Makowka L. Immunosuppression
transplantation is beyond the capacity of our
in organ transplantation. Semin Pediatr Surg 1993: 2: 206–217.
17. Parrott, NR. Immunosuppression: the old and the new. In
restricted human resource allocation (5, 46, 48–
JLR, ed. Transplantation Surgery, Chapter 5.
50). The potential of organ transplantation is
Philadelphia, PA: WB Saunders Company Ltd., pp. 89–121.
great and the number of children requiring and
18. Klintmalm G. US Multicenter FK506 Liver Study Group: a
35. Dickson RC, Everhartt JE, Lake JR et al. The National
comparison of tacrolimus (FK506) and cyclosporine for
Institute of diabetes and digestive and kidney diseases liver
immunosuppression in liver transplantation. New Eng J Med
transplantation database transmission of hepatitis B by trans-
plantation of livers from donors positive for antibody to hepa-
19. Hover PF. Cyclosporin A (Neoral) in paediatric organ trans-
titis B core antigen. Gastroenterology 1997: 113: 1668–1674.
plantation. Pediatr Tranplant 1998: 2: 35–39.
36. Rayes N, Neuhaus R, Naumann U et al. Treatment of
20. Ganschon R, Broering DE, Stuerenberg I, Regiers X,
hepatitis B reinfection or de novo infection after liver trans-
HR, Burdelski M. First experience with basili-
plantation with famiciclovir – how effective is it. Transplant
ximabl in pediatric liver graft recipients. Pediatr Transpl 2001:
37. Grellier L, Motimer D, Ahmed M et al. Lamivudine pro-
21. Fishman JA, Rubin RH. Infection in Organ-Transplant
phylaxis against reinfection in liver transplantation for hepa-
recipients. N Engl J Med 1998; 338: 1741–1751.
titis B cirrhosis. Lancet 1996: 348: 1212–1215.
22. Deen JL, Blumberg DA. Infectious Disease Considerations in
38. Wayman KI, Cox KL, Esquirel CO. Neurodevelopmental
Pediatric Organ Transplantation. Semin Pediatr Surg 1993: 2:
outcome of young children with extrahepatic biliary atresia
1 year after liver transplantation. J Pediatr 1997: 131: 894–898
23. Winston DJ, Wirin D, Shaked A, Busuttil W. Randomised
39. Gosi JA, Schackleton CR, Mc Dairmid SV et al. Long-term
comparison of gancyclovir and high-dose acyclovir for long-
results of paediatric liver transplantation. Ann Surg 1998: 228:
term cytomegalovirus prophylaxis in liver-transplant recipients.
40. Migliazza L, Lopez Santamaria M, Murcia J et al. Long-
24. Morgan G, Superina RA. Lymphoproliferative disease after
term survival expectancy after liver transplantation in children.
pediatric liver transplantation. J Pediatr Surg 1994: 29: 1192–
41. Sokal EM, Veyckemans F, De Ville De Goyet J et al. Liver
25. Mc Dairmid SV, Jordan S, Lee GS et al. Prevention and pre-
transplantation in children less than 1 year of age. J Pediatr
emptive therapy of post-transplant lympopmif erative disease
in pediatric liver recipients. Transplantation 1998: 66: 1604–
42. Stewart SM, Uauy R, Waller DA et al. Mental and motor
development. Social competence and growth one year after
26. Fujisawa Ltd. Prograf Data Sheet. London: Fujisawa Ltd.,
successful pediatric liver transplantation. J Pediatr 1989: 114:
27. Sandoz Pharmaceuticals (UK) Ltd. Neoral Data Sheet Survey.
43. Meyers BR, Halpern M, Sheiner P et al. Tuberculosis in liver
transplant patients. Transplantation 1994: 58: 301–306.
28. Yandza T, Gauthier F, Valayer J. Lessons from the first 100
44. Otte JB, De Ville De Goyet J, Sokal EM et al. Size reduc-
liver transplantations in infants and children at Biie¨tre Hospi-
tion of the donor liver is a safe way to alleviate the shortage of
tal. J Pediatr Surg 1994: 29: 905–911.
size-matched organs in pediatric liver transplantation. Ann
29. Demetris AJ, Batts KP, Dillon AP et al. Banff schema for
grading liver allograft rejection: an international consensus
45. Broelsch CN, Stevens LH, Whitington PF. The use of
document. Hepatology 1997: 25: 658–663.
reduced-size liver transplants in children, including split livers
30. Noble-Jamieson Barnes N. Diagnosis and management of
and living related transplants. Eur J Pediatr Surg 1991; 1:
late complications after liver transplantation. Arch Dis Child
46. Singer PA, Siegler M, Whitington PF et al. Ethics of liver
31. Phillips JO, Metzler MH, Palmieri TL et al. A prospective
transplantation with living donors. N Engl J Med 1989: 321:
study of simplified omeprazole suspension for the prophylaxis
of stress related mucosal damage. Crit Care Med 1996: 24:
47. Emre S. Living-donor liver transplantation in children. Pediatr
32. Millar AJW, Spearman W, Mc Culloch M et al. Paediatric
48. Colombani PM, Lau H, Prakhakaran K et al. Cumulative
liver transplantation in a developing country – taking stock.
experience with pediatric living related liver transplantation.
33. Spearman CWN, Mc Culloch M, Mllar AJW et al. Post-
49. Reyes G, Gerber D, Mazariegos GV et al. Split-liver trans-
transplant lymphoproliferative disease (PLTD) in paediatric
plantation: a comparison of ex vivo and in situ techniques.
liver transplant recipients in a developing country. Pediatr
50. Testa G, Malago M, Broelsch CE. From living related to
34. Goddard EA, Millar AJW, Spearman CWN, Mc Culloch
in-situ split liver transplantation: how to reduce waiting-list
MI, Kahn D. Cytomegalovirus (CMV) infection in paediatric
mortality. Pediatr Transplant 2001; 5: 16–20.
liver transplant recipients in a developing country. Pediatr
51. Shepherd RW. Liver transplantation in children. Med J Aust
NOTE: Pages in each section start with #1. Therefore, the pages go section 1 page 1, section 1 page 2, etc. Section 1 PROTOCOL ACKNOWLEDGMENT AND AUTHORIZATION Standing Medical Orders and Treatment Protocols . 1.2 Section 2 ADVANCED CARDIAC LIFE SUPPORT GUIDELINES Asystole . 2.2 Bradycardia (Heart rate < 60 beats per minute). 2.4 Tachycardia (heart rate > 100 beats per minute
Publicité directe des médicaments d’ordonnance : protéger les Canadiens avec une information de qualitéPublicité directe des médicaments d’ordonnance : protéger les Canadiens avec une information de qualité Rapport de recherche publié par l’Union des consommateurs 1 000 rue Amherst, bureau 300 Montréal (Québec) H2L 3X5 Téléphone : (514) 521-6820 Télécopieur : (514)
 Right and middle hepatic veins opened. Left sutured or ligated.
Right and middle hepatic veins opened. Left sutured or ligated.