Sore Hocks: To inject or not to inject? by Michael Scott, DVM; MVSc; Diplomate, American College of Veterinary Surgeons Dr. Michael Scott is an equine surgical specialist practicing at Moore and Company Veterinary Services in Calgary, Alberta. He has been a lifelong rider, competitor, and horse enthusiast. His practice interests include equine sports medicine, lameness diagnosis and treatment, and equine surgery.
A common lameness problem seen in western performance horses is painful hock
joints. Events such as cutting, working cowhorse, and reining require the horse to
work in a collected frame, with their hind legs bearing increased load. The sudden stops and quick turns of these events place enormous torque on the hind limbs. The
demanding physical nature of these disciplines, coupled with the horse's individual strengths and weaknesses, degree of fitness, and workload, can result in the horse
developing sore hocks at any age and at any stage of its career.
In order to have a better understanding of this
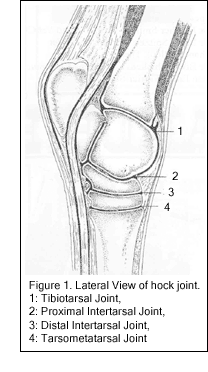
problem, it is important to have some knowledge of the anatomy of the hock joint. The hock is the analogue of the human ankle, and is composed of 8
bones and 4 separate joints (Fig. 1). The upper joint, or tibiotarsal joint, is where the movement occurs
during flexion and extension. The three lower joints (proximal intertarsal, distal intertarsal, and
tarsometatarsal joint) move very little, and are often referred to as low motion joints.
It is in the two lower joints, the distal intertarsal
and tarsometatarsal joints, where the horse most often becomes painful. This pain is due to varying
degrees of inflammation and damage to joint structures, ranging from mild synovitis (inflammation of the synovial lining of the joint) or arthritis (joint
inflammation) to advanced degenerative joint disease where there is extensive cartilage damage and bone
re-modeling. The term "bone spavin" has long been used to describe the condition of degenerative joint
disease affecting the lower hock joints.
Diagnosing lameness problems in this area may be a simple process or a
challenging puzzle. In the simplest scenario the horse is obviously lame, becomes
worse after the leg is flexed, and has obvious bone changes visible on radiographs and possibly even on the physical examination. The simple scenario doesn't seem to
be as common as the more diagnostically challenging case, where the unsoundness may only be apparent when the horse performs certain maneuvers. In such cases, communication between rider and veterinarian is important. Often the first signs of a
developing problem are detected by the astute rider as a change in the way a horse feels, the way it stops or spins in a certain direction, or its willingness to perform
When a performance problem is suspected, there are several tools and techniques
a veterinarian can use to look for unsoundness in the hock. After obtaining details
about the history of the problem, a lameness examination is performed. Diagnostic tests such as anesthetic nerve blocks, radiography, and possibly nuclear scintigraphy
may be used. Details about lameness diagnosis procedures are beyond the scope of this article, but an important point should be made regarding radiographs. In some
cases, particularly in young horses with early stages of hock arthritis, no abnormalities will be seen on the radiographs. In these cases, it is assumed that the
problem has not progressed enough to result in changes in the bones (which are the only tissues visible on radiographs).
Once arthritis of the lower hock joints has been diagnosed or is strongly suspected,
decisions can be made regarding treatment. Options include rest, evaluation and possibly changes in shoeing, nutritional supplements and systemic medications, acupuncture, hock injections, and possibly surgery. The simpler and less invasive
treatments and management options should be considered before joint injections are used.
Probably the most effective and often used treatment for arthritis and pain in the
lower hock joints is joint injection. Several different medications are used. Corticosteroids, often referred to as "steroids" or "cortisone", are actually a large
family of drugs with potent anti-inflammatory activities of varying strengths and durations. Trimacinolone is one corticosteroid which has a medium duration of action
and is widely used for joint injection. Methylprednisolone acetate (Depro-Medrol) is a potent, long acting corticosteroid most often used for injection in the lower hock
joints. Another medication that can be used is hyaluronic acid (Hyonate or Legend). Hyaluronic acid is found naturally in the cartilage and synovial fluid within the joint, where it has important functions. Administered intravenously or into the joint,
hyaluronic acid acts in numerous ways, including reducing inflammation, improving the quality of synovial fluid, and in cartilage maintenance. In the lower hock joints in
particular, methylprednisolone acetate alone or in conjunction with hyaluronic acid is most often used. The duration of action of this treatment is variable and depends on
many factors including the severity of disease and the intensity of work the horse is performing. In some cases benefit may only be seen for as little as a few weeks,
whereas in other cases the effect may last for a year or more.
The horse owner and competitive rider will eventually face the question of "to
inject or not to inject". As a veterinarian, I often see clients struggle with this
question and express concern about what they might be doing to their horse. This reaction is justified, as there are certainly some negative implications associated with joint injections. If we take a step back and ask the question "why has this horse
become sore?", the answer is often "because it is being asked to perform strenuous work". If medication is injected into the joint, its primary effect is to reduce
inflammation in the joint and therefore reduce pain. It will also have some beneficial effects in reducing the joint degeneration that occurs with chronic arthritis. However,
if the horse continues to perform at the same level, the stresses placed upon the joint may continue to cause "wear and tear" type injury, leading to an eventual
return of joint inflammation and pain. A scenario of repetitive joint injections of increasing frequency being needed in order to keep a horse going may develop, leading to concern about the long term health of the joint.
The important point to remember when discussing injection of the lower hock
joints is that they are "low motion" joints. If the arthritic condition is affecting a
"high motion" joint such as the coffin joint or the fetlock, ongoing joint degeneration can lead to permanent lameness. When the arthritic condition is affecting the lower
hock joints, this is not necessarily the case. These joints are not as functionally important to the movement of the horse as high motion joints are. In some cases of
advanced degenerative joint disease, one or both of the lower hock joint may actually fuse, which is a desirable result as it does not have a great impact on the
function of the leg but it does result in relief from the pain, as there is no longer a joint to be painful. In fact, in some cases surgical techniques have been used to cause accelerated fusion of these joints.
So although there are reasons to be concerned about the risks and potential
negative effects of joint injection in any situation, in the case of the lower hock joints the advantages of this treatment seem to outweigh the disadvantages, particularly if
the objective of treatment is to reduce the discomfort that horse is experiencing and allow it to continue to perform.
ADMINISTRATIVE AGREEMENT July 1, 2007 June 30, 2010 I. Recognition Clause The East Detroit Board of Education recognizes the East Detroit Schools Administrators Association (EDSAA) the American Federation of School Administrators (AFSA), Local 89, AFL-CIO in accordance with the applicable provisions of Act 379, P.A. of 1965 as amended as the sole and exclusive representatives of a
REPORT TO: CIAT and all Latin America FROM: Iván Allende (Paraguay) Jaime Argueta (El Salvador) Lourdes Kusunoki ( Peru ) SUBJECT: World CAB 3 Meeting DATE: London , July13-14, 2006 Access to second line antiretroviral regimens Financed by the International Treatment Preparedness Coalition in cooperation with HIV i-Base List of participants: Mohamed Amin India . Jaime Argueta El Salvador. Iryna
 Sore Hocks: To inject or not to inject?
Sore Hocks: To inject or not to inject?