Hum Psychopharmacol Clin Exp 2003; 18: 379–384. Published online 9 May 2003 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hup.490
Fluvoxamine versus fluoxetine in major depressive episode:a double-blind randomised comparison
1Hoˆpital Neurologique Pierre Wertheimer, F-69003 Lyon, France2University Hospital Maastricht, 6202 AZ Maastricht, The Netherlands
A double-blind, multinational study was conducted to compare the efficacy and safety of fluvoxamine and fluoxetine inoutpatients with major depressive episode; 184 patients were randomised to fluvoxamine (100 mg/day) or fluoxetine(20 mg/day) for 6 weeks. Both drugs were effective and there were no statistically significant differences between themin the area under the curve of change from baseline in the Hamilton depression rating scale (HAMD) total score. However,the percentage of HAMD responders (!50% decrease in HAMD total score) at week 2, the clinical global improvementseverity of illness score at week 2 and the depression subscale of the irritability, depression and anxiety scale at weeks1, 2 and 4, all showed significant advantages for fluvoxamine. During the last 2 weeks, fluvoxamine was significantlymore effective in improving the HAMD sleep disturbance scale. Both drugs were well tolerated and there were no markeddifferences in their side effect profiles which were typical of SSRIs. Fluvoxamine and fluoxetine have similar efficacy andsafety profiles in the treatment of major depressive episode; the findings of this study indicate that fluvoxamine may have afaster onset of action with respect to resolution of depressive symptoms and result in a better improvement in sleep quality. Copyright # 2003 John Wiley & Sons, Ltd.
key words — fluvoxamine; fluoxetine; selective serotonin reuptake inhibitor; depression
with another. However, available evidence suggeststhat all SSRIs do not share the same profile (Leonard,
Although tricyclic antidepressants are effective in the
1992; van Harten, 1993; Montgomery et al., 1994;
treatment of depression, they are associated with a
Wilde et al., 1993; DeVane, 1995; Hindmarch,
number of adverse events (such as dry mouth, tremor,
1995; van den Berg, 1995; Price et al., 1996; Lane,
low blood pressure and cardiovascular effects) that
1997; Waldinger et al., 1998). For example, there
hinder compliance and may occasionally be danger-
are considerable differences in their chemical struc-
ous. Selective serotonin reuptake inhibitors (SSRIs)
tures (van den Berg, 1995) and in their pharmacologi-
generally show comparable efficacy to the tricyclic
cal (Leonard, 1992) and pharmacokinetic (van Harten,
antidepressants (Anderson and Tomenson, 1994) but
1993) behaviour. Findings from meta-analyses have
have a more benign safety profile (Montgomery
suggested there may be differences in efficacy
between the SSRIs in certain patient subgroups, such
Despite a wealth of studies comparing the SSRIs
as those with severe depression (Anderson and
with other classes of antidepressant and placebo, there
Tomenson, 1994). There is also evidence that there
have been few studies directly comparing one SSRI
are differences in their safety profiles, with paroxetineand sertraline being associated with more sexual side-effects (Nemeroff et al., 1995; Lane, 1997; Waldingeret al., 1998) and fluoxetine being associated with
* Correspondence to: Dr J. Dalery, Unite´ de PsychologieMe´dicale et de Psychiatrie de Liaison, Hoˆpital Neurologique
more anxiety and nervousness (Aguglia et al., 1993).
Pierre Wertheimer, 59 Boulevard Pinel, F-69003 Lyon, France.
This study, the results have which have not pre-
Tel: þ33 472 11 80 64. Fax: þ33 472 35 71 09.
viously been published in full, was designed to
Contract/grant sponsor: Solvay Pharmaceuticals.
directly compare the efficacy and safety of two widely
Copyright # 2003 John Wiley & Sons, Ltd.
prescribed SSRIs, fluvoxamine and fluoxetine, in a
large, multicentre, randomised, double-blind study
The primary efficacy parameter was the area under the
in patients with a major depressive episode.
curve (AUC) of the change in 17-item HAMD totalscore from baseline (expressed as HAMD weeks).
Secondary efficacy variables comprised: the numberof 17-item HAMD responders (i.e. the number of
This was a prospectively randomised, double-blind,
patients with at least a 50% improvement in 17-item
fixed-dose, parallel-group study conducted according
HAMD total score); the clinical global impression
to the principles of good clinical practice in 24 Eur-
(CGI) (Guy, 1976) severity of illness and global
improvement scores; the clinical anxiety scale(CAS) score; the irritability, depression and anxiety
scale (IDAS) total score and subscores; the Beck’sscale for suicide ideation (SSI) score; sleep evaluation
Outpatients of either sex, aged 18–70 years old, meet-
and the 17-item HAMD total and subtotal scores.
ing DSM-III-R (American Psychiatric Association,
The 17-item HAMD was determined at screening,
1987) criteria for major depressive episode and having
baseline and after 1, 2, 4 and 6 weeks (or upon prema-
a total score of 17 or more on the 17-item Hamilton
ture termination) of treatment; all other efficacy vari-
depression rating scale (HAMD) (Hamilton, 1967)
ables were determined at all visits except screening.
were included in the study. Patients were excluded if
Adverse events were documented at baseline and at
they had: acute suicidal ideation or a serious suicide
each subsequent visit; vital signs and weight were
attempt in the previous 6 months; dementia; a history
measured at baseline and at the final visit and a phy-
of epilepsy or seizures; concurrent or recent (6
sical examination was conducted at screening and at
months) alcoholism, other psychoactive substance
abuse or drug-induced psychosis; were pregnant, lac-tating or of childbearing potential and not taking ade-quate contraceptive measures; or if they had clinically
uncontrolled hepatic, renal, pulmonary, endocrine orcollagen disease. Also excluded were patients who
Efficacy was assessed using the intent-to-treat (ITT)
had previously failed SSRI therapy or who required
efficacy sample (i.e. patients who received at least
concomitant lithium, warfarin, hepatically metabo-
one dose of study medication and provided at least
lised antivitamin K agents, carbamazepine, theophyl-
one valid post-baseline efficacy evaluation on study
line, insulin or hypoglycaemic agents. Patients were
medication) and the per-protocol (PP) sample (i.e.
required not to receive monoamine oxidase inhibitors
subset of ITT patient sample who did not have any ser-
or electroconvulsive therapy (ECT) in the 2 weeks
ious deviation from the study protocol). Analyses of
prior to the study. All patients provided written or
secondary efficacy variables were performed on the
verbally witnessed informed consent.
ITT efficacy sample only. All analyses were per-formed using visit-wise (observed cases; OC) andlast observation carried forward (LOCF) data. The
Wilcoxon two-sample test was used to analyse both
All patients entered a 7-day placebo run-in period that
the primary and the secondary efficacy variables. All
enabled previous antidepressant therapy to be with-
tests were two-sided. Differences with p values
drawn and identified any patients who were likely to
0.05 were considered to be statistically significant.
respond to placebo. Eligible patients were then rando-mised to receive oral fluvoxamine (100 mg/day) or
fluoxetine (20 mg/day) for 6 weeks; fluvoxamine(Solvay Pharmaceuticals) was given at a dose of
One-hundred and eighty-four patients were rando-
50 mg/day for the first 7 days of the study. Doses were
mised to treatment, 90 to fluvoxamine (33 male, 57
as recommended by the respective manufacturers for
female; mean age 42 years) and 94 to fluoxetine
the treatment of major depressive episode.
(35 male, 59 female; mean age 42.1 years); there were
Oxazepam or nitrazepam were permitted as neces-
no significant differences between the two treatment
sary for night-time sedation; no other psychothera-
groups with respect to gender, race, age distribution,
peutic treatments or ECT were permitted during the
body weight or height. Four patients in the fluvoxa-
mine group and three in the fluoxetine group had no
Copyright # 2003 John Wiley & Sons, Ltd.
Hum Psychopharmacol Clin Exp 2003; 18: 379–384.
post-baseline assessment and were therefore excludedfrom the ITT efficacy sample (86 fluvoxamine patientsand 91 fluoxetine patients). A further four patients inthe fluvoxamine group and seven in the fluoxetinegroup had major deviations from the protocol andwere excluded from the PP sample (82 fluvoxaminepatients and 84 fluoxetine patients). Reasons forexclusion were failure to meet inclusion or exclusioncriteria (3 fluvoxamine, 3 fluoxetine patients), disal-lowed prior medication (1 fluvoxamine and 3 fluoxe-tine patients) and baseline HAMD less than 17(I fluoxetine patient). Sixteen patients in the fluvoxa-mine group and ten in the fluoxetine group withdrewfrom the study prematurely.
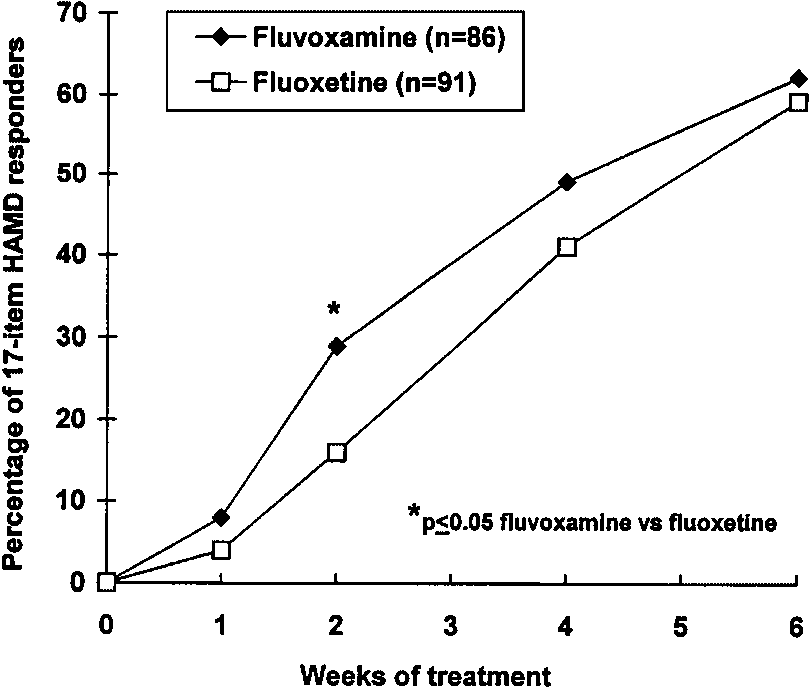
Figure 1. Percentage of 17-item HAMD responders (ITT sample;LOCF analysis)
Fluvoxamine and fluoxetine both resulted in a signifi-cant improvement in depressive symptoms.
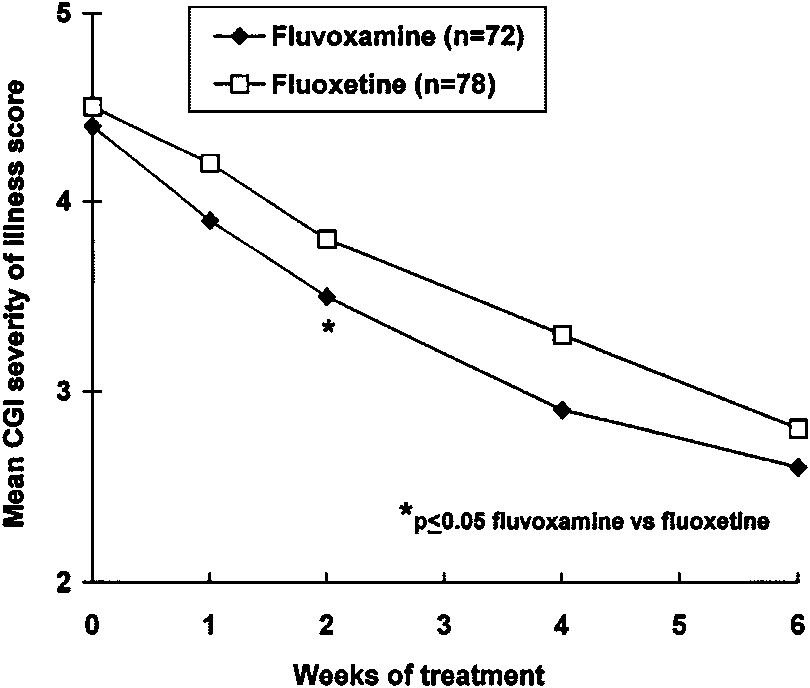
CGI severity of illness score. The overall severity ofillness was progressively reduced in both groups from
Primary variable. The mean AUC of the change from
‘moderately to markedly ill’ to ‘borderline to mildly
baseline in 17-item HAMD total score decreased
ill’. However, the reduction in the mean score was
progressively during the study in both groups. After 6
greater with fluvoxamine than with fluoxetine at all
weeks of treatment, the mean AUC value was À189
assessments, the difference achieving statistical sig-
HAMD weeks in the fluvoxamine group and À175
nificance ( p 0.05) at week 2 (Figure 2).
HAMD weeks in the fluoxetine group. HAMD scoreswere reduced from a mean of 22.3 and 22.2 at baseline
CGI global improvement score. Again, a continuous
in the fluvoxamine and fluoxetine groups respectively
improvement was seen in both groups; at the end of
to 10.0 and 11.3, respectively, at day 42. There were
the study, the mean score was 2.0 (much improved) in
no statistically or clinically significant differences
the fluvoxamine group and 2.2 (minimally to much
between the treatments at any point or in any of the
improved) in the fluoxetine group. There were no
significant differences between the treatments at anypoint.
Secondary variables. The secondary efficacy vari-ables confirmed the overall effectiveness of fluvox-amine and fluoxetine, but revealed some benefits offluvoxamine over fluoxetine. The data are presentedfor the LOCF analysis; similar results were obtainedfrom the OC analysis.
Percentage of 17-item HAMD responders. A patientwas considered to be a responder if they had areduction in 17-item HAMD total score of at least50% from baseline. Patients appeared to respondbetter to fluvoxamine than to fluoxetine, especiallyduring the early stages of treatment (Figure 1); after 2weeks of treatment, the percentage of patients whoresponded was significantly higher with fluvoxaminethan with fluoxetine (29% vs 16%; p 0.05). At theend of the study, the majority (approximately 60%) ofpatients in both groups were considered to be
Figure 2. Mean CGI severity of illness score (ITT sample; LOCF
Copyright # 2003 John Wiley & Sons, Ltd.
Hum Psychopharmacol Clin Exp 2003; 18: 379–384.
Mean change in IDAS total and subscores (ITT sample;
ap 0.05 fluvoxamine versus fluoxetine.
Figure 3. Mean change in sleep evaluation score (ITT sample;LOCF analysis)
CAS total score. The mean score decreased progres-sively in both groups. In the fluvoxamine group, themean score fell from 12.6 at baseline to 6.9 at the end
(25% in the fluvoxamine group and 30% in the
of the study; the corresponding reduction in the
fluoxetine group) which was allowed in the protocol
fluoxetine group was from 13.1 to 7.7. There were nosignificant differences between the treatments at any
17-item HAMD total and subtotal scores. The mean
total score decreased progressively in both groups; atthe end of the study, the mean score had fallen from
IDAS total score and subscores. The IDAS total and
22.3 to 10.0 in the fluvoxamine group and from 22.2 to
subscores, which assess levels of irritability, depres-
11.3 in the fluoxetine group. There were no significant
sion and anxiety, all fell progressively during the
differences between the treatments at any point.
study. As shown in Table 1, the reduction in the mean
Fluvoxamine was associated with a greater reduc-
total score was greater with fluvoxamine than with
tion in anxiety/somatisation and cognitive disturbance
fluoxetine at all time points. Mean changes in the
subscores, although there were no statistically signifi-
anxiety, irritability and depression subscores were
cant differences between the groups. The improvement
also greater with fluvoxamine at all time points; a
in the retardation subscore was similar in each group.
statistically significant difference being achieved with
However, in agreement with the sleep evaluation score,
the depression subscore at weeks 1, 2 and 4.
fluvoxamine was more effective than fluoxetine atimproving the quality of sleep. The improvement in
Beck’s SSI score. The mean score decreased progres-
the sleep disturbance subtotal was statistically signifi-
sively in both groups; at the end of the study, it had
cantly greater with fluvoxamine than with fluoxetine at
fallen from 4.7 to 1.6 in the fluvoxamine group and
week 4 (À2.3 vs À1.6; p 0.05) and at the end of the
from 5.4 to 2.1 in the fluoxetine group. There were no
study (À2.4 vs À1.8; p 0.05) and was of borderline
significant differences between the treatments at any
significance ( p ¼ 0.052) at week 1 (Figure 4).
Sleep evaluation. There was a gradual improvement inmean sleep evaluation scores in both groups over the
Fluvoxamine and fluoxetine were both well tolerated.
course of the study. As shown in Figure 3, the
There was a similar incidence of adverse events in each
improvement in the quality of sleep was more pro-
group, the majority of which were mild or moderate.
nounced with fluvoxamine at weeks 4 and 6, although
The most frequently reported treatment-emergent
the differences did not achieve statistical significance.
signs and symptoms (TESS) in both groups were nau-
Overall, slightly more than half of all patients (51% in
sea (24% with fluvoxamine and 20% with fluoxetine)
both groups) used a hypnotic drug during the study.
and headache (13% with fluvoxamine and 14% with
The most frequently used hypnotic was oxazepam
fluoxetine). No other TESS occurred in more than
Copyright # 2003 John Wiley & Sons, Ltd.
Hum Psychopharmacol Clin Exp 2003; 18: 379–384.
Fluvoxamine also appeared to have a more benefi-
cial effect on sleep quality, especially after 4 weeks oftreatment. The reduction in sleep disturbance was sig-nificantly greater with fluvoxamine than with fluoxe-tine from week 4 onwards according to the 17-itemHAMD sleep disturbance score. Moreover, fluvoxa-mine was clearly superior to fluoxetine on the sleepevaluation score from week 4 onwards. Patients trea-ted with fluvoxamine showed a progressive improve-ment in sleep quality throughout the study, whilstthose given fluoxetine showed little improvementafter the second week. These findings are consistentwith clinical experience suggesting that fluvoxaminecauses less sleep disturbance and is less activating thanfluoxetine (Baldessarini and Marsh, 1990; Rickels andSchweizer, 1990; Freeman, 1991; Aguglia et al.,
Figure 4. Mean change in 17-item HAMD sleep disturbance
Both treatments improved anxiety symptoms, irrit-
ability, suicidal ideation, retardation and cognitive
10% of patients in either group. Sexual dysfunction
disturbance. A somewhat greater improvement in
was reported by one patient in the fluvoxamine group
anxiety, irritability and cognitive disturbance was
(ejaculatory abnormality) and two in the fluoxetine
observed with fluvoxamine, but these differences
group (ejaculatory abnormality and impotence).
did not achieve statistical significance. Again, this is
There were four patients with serious adverse
consistent with the propensity of fluoxetine to cause
events. One (anxiety and alcohol intoxication) occur-
activation (Baldessarini and Marsh, 1990; Rickels
red in the fluvoxamine group and was considered
and Schweizer, 1990; Aguglia et al., 1993; Lane
unrelated to treatment and three occurred in the
fluoxetine group (anorexia and stomach complaints
There are a number of clear differences between
that were considered highly probably related to treat-
fluvoxamine and fluoxetine. They have completely
ment in one patient, a suicide attempt that was consi-
different chemical structures and pharmacokinetic
dered possibly related to treatment in another and a
and pharmacological profiles. For example, fluoxetine
suicide attempt that was considered unrelated to treat-
has a considerably longer half-life than fluvoxamine
(2–4 days vs 17–22 h) (Preskorn, 1997) and is the only
There were no clinically significant changes in vital
SSRI with a metabolite that has significant clinical
signs, body weight or physical condition in either
activity (Lane et al., 1995). In addition, fluoxetine
reduces dopamine synthesis (Baldessarini and March,1990) whilst fluvoxamine has no effect on dopaminer-gic neurotransmission.
However, there have been very few studies directly
Fluvoxamine (100 mg/day) and fluoxetine (20 mg/day)
comparing the efficacy of one SSRI with another. This
both resulted in a progressive, clinically significant
direct, double-blind comparison of fluvoxamine and
improvement in 17-item HAMD total score over the
fluoxetine in patients with a major depressive episode
course of treatment. However, analysis of secondary
was therefore designed to provide data on potential
efficacy parameters indicated that fluvoxamine may
areas of differentiation between the efficacy of the
have some advantage over fluoxetine during the early
two treatments. Thus, a wide range of variables were
phase of treatment: the percentage of 17-item HAMD
selected in order to assess all the characteristic symp-
responders, the CGI severity of illness score and the
toms of major depressive episode including depres-
IDAS depression subscore all showed a significantly
sion, sleep disturbance, irritability, anxiety, cognitive
greater improvement with fluvoxamine after 2 weeks
disturbance, retardation and suicidal ideation.
of treatment. However, whilst the differences between
A number of previous studies have suggested that
the two treatments were maintained after 4 weeks of
the SSRIs may show some differences in their safety
treatment, they remained statistically significant only
profiles. Thus, sertraline (Nemeroff et al., 1995) and
paroxetine (Waldinger et al., 1998) appear to be
Copyright # 2003 John Wiley & Sons, Ltd.
Hum Psychopharmacol Clin Exp 2003; 18: 379–384.
associated with more sexual side-effects than fluvox-
Freeman CP. 1991. Fluvoxamine: clinical trials and clinical use.
amine, whilst fluoxetine (Aguglia et al., 1993; Stokes,
J Psychiatr Neurosci 16(Suppl. 1): 19–25.
Guy W. 1976. ECDEU Assessment Manual for Psychopharmacol-
1993; DeVane, 1995) has been reported to cause more
ogy. National Institute of Mental Health, US Department of
anxiety and nervousness than the other SSRIs. Simi-
Health, Education and Welfare: Washington, DC.
larly, in accordance with its pharmacological profile,
Hamilton M. 1967. Development of a rating scale for primary
paroxetine (Dunbar, 1989; Kiev and Feigher, 1997)
depressive illness. Br J Soc Clin Psychol 6: 278–296.
Hindmarch I. 1995. The behavioural toxicity of the selective sero-
tends to be associated with a higher incidence of
tonin reuptake inhibitors. Int Clin Psychopharmacol 9(Suppl. 4):
anticholinergic effects (such as sedation, sweating
and dry mouth) than the other SSRIs. However,
Kiev A, Feiger A. 1997. A double-blind comparison of fluvoxamine
neither fluvoxamine nor fluoxetine have adverse car-
and paroxetine in the treatment of depressed outpatients. J Clin
diac side-effects, as measured using both ECG and
Lane RM. 1997. A critical review of selective serotonin reuptake
echocardiography, a more direct reflection of cardiac
inhibitor-related sexual dysfunction: incidence, possible aetiol-
functioning (Strik et al., 1998). In the current study,
ogy and implications for management. J Psychopharmacol 11:
fluvoxamine and fluoxetine were equally well toler-
ated and had very similar safety profiles. Nausea
Lane R, Baldwin D, Preskorn S. 1995. The SSRIs: advantages, dis-
advantages and differences. J Psychopharmacol 9(Suppl.): 163–
and headache were the most common adverse events
and were reported by similar proportions of patients
Leonard BE. 1992. Pharmacological differences of serotonin
reuptake inhibitors and possible clinical relevance. Drugs
In conclusion, fluvoxamine 100 mg/day is at least
as effective and safe as fluoxetine 20 mg/day in the
Montgomery SA, Henry J, McDonald G, et al. 1994. Selective ser-
otonin reuptake inhibitors: meta-analysis of discontinuation
treatment of major depressive episode and may be
rates. Int Clin Psychopharmacol 9: 47–53.
superior in terms of onset of action and improvement
Nemeroff CB, Ninan PT, Ballenger J, et al. 1995. Double-blind mul-
ticenter comparison of fluvoxamine versus sertraline in the treat-ment of depressed outpatients. Depression 3: 163–169.
Preskorn SH. 1997. Clinically relevant pharmacology of selective
serotonin reuptake inhibitors. Clin Pharmacokinet 32(Suppl. 1):
The study was supported by a grant from Solvay Phar-
Price JS, Waller PC, Wood SM, et al. 1996. A comparison of the
postmarketing safety of four selective serotonin reuptake inhibi-
tors including the investigation of symptoms occurring on with-drawal. Br J Clin Pharmacol 42: 757–763.
Rickels K, Schweizer E. 1990. Clinical overview of serotonin reup-
take inhibitors. J Clin Psychiatry 51(Suppl. B): 9–12.
Stokes PE. 1993. Fluoxetine: a five-year review. Clin Ther 15:
Aguglia E, Casacchia M, Cassano GB, et al. 1993. Double-blind
study of the efficacy and safety of sertraline versus fluoxetine
Strik JJMH, Honig A, Lousberg R, et al. 1998. Cardiac side-effects of
in major depression. Int Clin Psychopharmacol 8: 197–202.
two selective serotonin reuptake inhibitors in middle-aged
American Psychiatric Association. 1987. Diagnostic and Statistical
and elderly depressed patients. Int Clin Psychopharmacol 13: 1–5.
Manual of Mental Disorders 3rd revised edn (DSM-III-R).
van den Berg SJ. 1995. Comparing SSRIs: from chemistry to clin-
American Psychiatric Association: Washington, DC.
ical choice. Hum Psychopharmacol 10: S199–S209.
Anderson IM, Tomenson BM. 1994. The efficacy of selective sero-
Van Harten J. 1993. Clinical pharmacokinetics of selective seroto-
tonin reuptake inhibitors in depression: a meta-analysis of studies
nin reptake inhibitors. Clin Pharmacokinet 24: 203–220.
against tricyclic antidepressants. J Psychopharmacol 8: 238–249.
Waldinger MD, Hengeveld MW, Zwinderman AH, et al. 1998. The
Baldessarini RJ, Marsh E. 1990. Fluoxetine and side effects. Arch
effect of SSRI antidepressants on ejaculation: a double-blind,
randomised, placebo-controlled study with fluoxetine, fluvoxa-
DeVane CL. 1995. Comparative safety and tolerability of selective
mine, paroxetine and sertraline. J Clin Psychopharmacol 18:
serotonin reuptake inhibitors. Hum Psychopharmacol 10(Suppl.
Wilde MI, Plosker GL, Benfield P. 1993. Fluvoxamine: an updated
Dunbar GC. 1989. An interim overview of the safety and tolerability
review of its pharmacology, and therapeutic use in depressive ill-
of paroxetine. Acta Psychiat Scand 80(Suppl. 350): 135–137.
Copyright # 2003 John Wiley & Sons, Ltd.
Hum Psychopharmacol Clin Exp 2003; 18: 379–384.
D-DAY, FIRSTHAND Survivors of the Allied invasion recall the fear and exhilaration of 60 years ago D. M. GIANGRECO and KATHRYN MOORE The Kansas City Star, June 6, 2004 “The movie ‘Saving Private Ryan' captured the intensity of the battle but think of those first 19 minutes actually lasting four hours.” — Chief Petty Officer Jerry Markham, who landed on Omaha Beach Sixty year
 post-baseline assessment and were therefore excludedfrom the ITT efficacy sample (86 fluvoxamine patientsand 91 fluoxetine patients). A further four patients inthe fluvoxamine group and seven in the fluoxetinegroup had major deviations from the protocol andwere excluded from the PP sample (82 fluvoxaminepatients and 84 fluoxetine patients). Reasons forexclusion were failure to meet inclusion or exclusioncriteria (3 fluvoxamine, 3 fluoxetine patients), disal-lowed prior medication (1 fluvoxamine and 3 fluoxe-tine patients) and baseline HAMD less than 17(I fluoxetine patient). Sixteen patients in the fluvoxa-mine group and ten in the fluoxetine group withdrewfrom the study prematurely.
post-baseline assessment and were therefore excludedfrom the ITT efficacy sample (86 fluvoxamine patientsand 91 fluoxetine patients). A further four patients inthe fluvoxamine group and seven in the fluoxetinegroup had major deviations from the protocol andwere excluded from the PP sample (82 fluvoxaminepatients and 84 fluoxetine patients). Reasons forexclusion were failure to meet inclusion or exclusioncriteria (3 fluvoxamine, 3 fluoxetine patients), disal-lowed prior medication (1 fluvoxamine and 3 fluoxe-tine patients) and baseline HAMD less than 17(I fluoxetine patient). Sixteen patients in the fluvoxa-mine group and ten in the fluoxetine group withdrewfrom the study prematurely.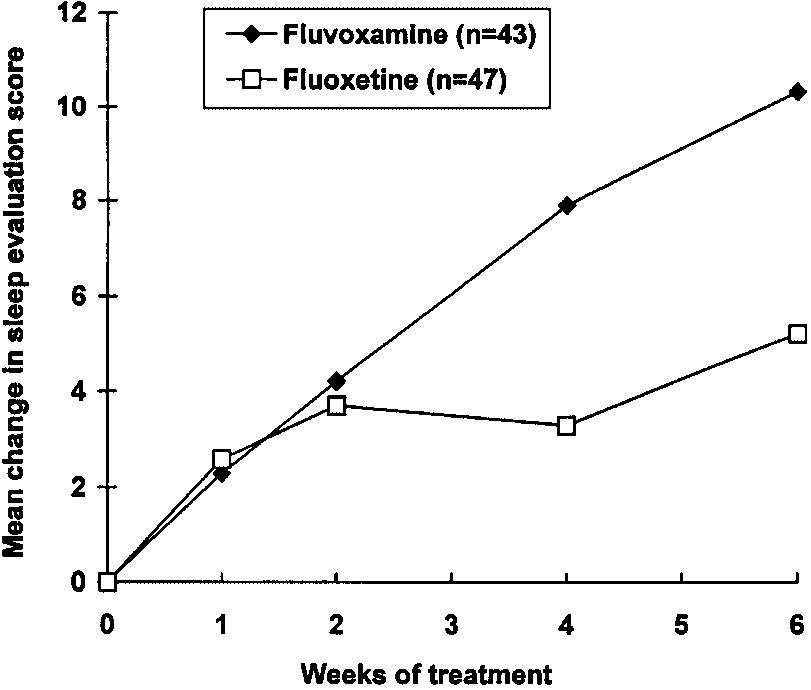 Mean change in IDAS total and subscores (ITT sample;
ap 0.05 fluvoxamine versus fluoxetine.
Mean change in IDAS total and subscores (ITT sample;
ap 0.05 fluvoxamine versus fluoxetine.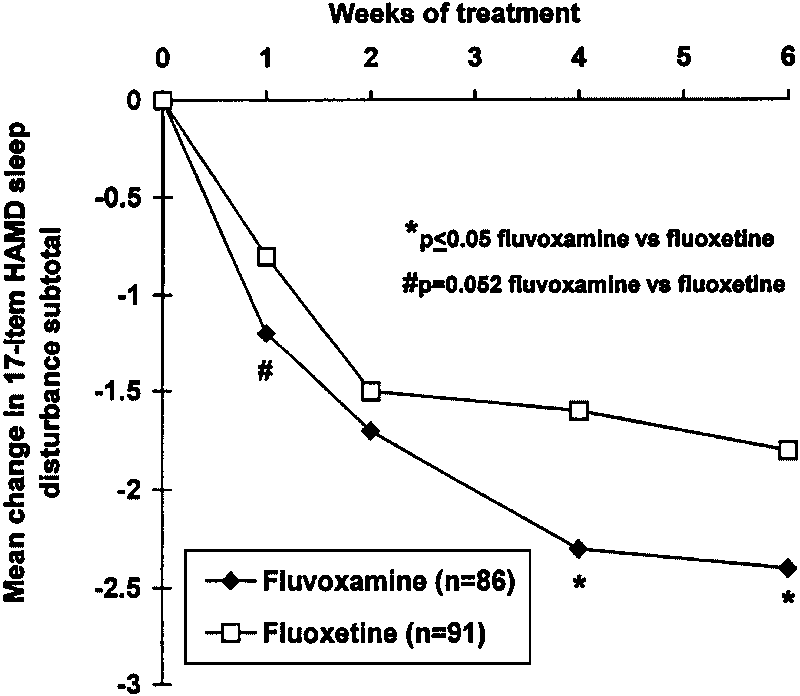 Fluvoxamine also appeared to have a more benefi-
cial effect on sleep quality, especially after 4 weeks oftreatment. The reduction in sleep disturbance was sig-nificantly greater with fluvoxamine than with fluoxe-tine from week 4 onwards according to the 17-itemHAMD sleep disturbance score. Moreover, fluvoxa-mine was clearly superior to fluoxetine on the sleepevaluation score from week 4 onwards. Patients trea-ted with fluvoxamine showed a progressive improve-ment in sleep quality throughout the study, whilstthose given fluoxetine showed little improvementafter the second week. These findings are consistentwith clinical experience suggesting that fluvoxaminecauses less sleep disturbance and is less activating thanfluoxetine (Baldessarini and Marsh, 1990; Rickels andSchweizer, 1990; Freeman, 1991; Aguglia et al.,
Figure 4. Mean change in 17-item HAMD sleep disturbance
Both treatments improved anxiety symptoms, irrit-
ability, suicidal ideation, retardation and cognitive
10% of patients in either group. Sexual dysfunction
disturbance. A somewhat greater improvement in
was reported by one patient in the fluvoxamine group
anxiety, irritability and cognitive disturbance was
(ejaculatory abnormality) and two in the fluoxetine
observed with fluvoxamine, but these differences
group (ejaculatory abnormality and impotence).
Fluvoxamine also appeared to have a more benefi-
cial effect on sleep quality, especially after 4 weeks oftreatment. The reduction in sleep disturbance was sig-nificantly greater with fluvoxamine than with fluoxe-tine from week 4 onwards according to the 17-itemHAMD sleep disturbance score. Moreover, fluvoxa-mine was clearly superior to fluoxetine on the sleepevaluation score from week 4 onwards. Patients trea-ted with fluvoxamine showed a progressive improve-ment in sleep quality throughout the study, whilstthose given fluoxetine showed little improvementafter the second week. These findings are consistentwith clinical experience suggesting that fluvoxaminecauses less sleep disturbance and is less activating thanfluoxetine (Baldessarini and Marsh, 1990; Rickels andSchweizer, 1990; Freeman, 1991; Aguglia et al.,
Figure 4. Mean change in 17-item HAMD sleep disturbance
Both treatments improved anxiety symptoms, irrit-
ability, suicidal ideation, retardation and cognitive
10% of patients in either group. Sexual dysfunction
disturbance. A somewhat greater improvement in
was reported by one patient in the fluvoxamine group
anxiety, irritability and cognitive disturbance was
(ejaculatory abnormality) and two in the fluoxetine
observed with fluvoxamine, but these differences
group (ejaculatory abnormality and impotence).