Long-term cognitive profile and incidence of dementia after stn-dbs in parkinson's disease
Movement DisordersVol. 22, No. 7, 2007, pp. 974-981 2007 Movement Disorder Society
Long-Term Cognitive Profile and Incidence of Dementia After
Selma Aybek, MD,1 Aline Gronchi-Perrin,1 Alexandre Berney, MD,2 Sabina Catalano Chiuve´,3
Jean-Guy Villemure, MD,4 Pierre R. Burkhard, MD,3 and Franc¸ois J.G.Vingerhoets, MD1*
1Service de Neurologie, CHUV, Lausanne, Switzerland2Service de Psychiatrie, CHUV, Lausanne, Switzerland3Service de Neurologie, HUG, Gene`ve, Switzerland4Service de Neurochirurgie, CHUV, Lausanne, SwitzerlandAbstract: An effect of subthalamic nucleus deep brain stimu-
operative differences between PDD and PD included older age
lation (STN-DBS) on cognition has been suspected but long-
(69.2 Ϯ 5.8 years; 62.6 Ϯ 8 years), presence of hallucinations
term observations are lacking. The aim of this study was to
and poorer executive score (10.1 Ϯ 5.9; 5.5 Ϯ 4.4). The
evaluate the long-term cognitive profile and the incidence of
incidence of dementia over 3 years after STN-DBS is similar to
dementia in a cohort of Parkinson’s disease (PD) patients
the one reported in medically treated patients. The PDD pre-
treated by STN-DBS. 57 consecutive patients were prospec-
sented preoperative risk factors of developing dementia similar
tively assessed by the mean of a neuropsychological battery
to those described in medically treated patients. These obser-
over 3 years after surgery. Dementia (DSM-IV) and UPDRS I
vations suggest dementia being secondary to the natural evo-
to IV were recorded. 24.5% of patients converted to dementia
lution of PD rather than a direct effect of STN-DBS. 2007
over 3 years (incidence of 89 of 1,000 per year). This group of
patients cognitively continuously worsened over 3 years up to
Key words: dementia; subthalamic; DBS; Parkinson’s
fulfilling dementia criteria (PDD). The rest of the cohort re-
mained cognitively stable (PD) over the whole follow-up. Pre-
Subthalamic nucleus (STN) deep brain stimulation
disability with an almost 6-fold increased risk when
(DBS) for Parkinson’s disease (PD) has been validated:
compared with normal controls.8 Prevalence and inci-
STN deep brain stimulation (STN-DBS) provides good
dence of dementia in surgically treated patients is un-
motor outcome,1 and allows significant reduction of an-
known, as cognitive data on the long-term impact of
tiparkinsonian medication.2 There has been much debate
as to whether STN-DBS may cause adverse effects on
In this prospective study, we examined the long-term
cognition and behavior3-7 with suspicion of a negative
evolution of cognition after STN-DBS, including the
impact on cognition, particularly executive functions.
incidence of dementia, and we studied potential risk
In medically treated PD, the prevalence of dementia is
factors for postoperative cognitive decline.
now considered to be much higher than previously
thought, reaching 60% after 10 to 15 years of motor
We studied 57 (36 men, 21 women, age 63.8 Ϯ 8
years, PD duration 15.7 Ϯ 5 years) consecutive nonde-
*Correspondence to: Francois Vingerhoets, Service de Neurologie,
mented PD patients who underwent bilateral STN-DBS
CHUV, Rue Bugnon 44, 1011 Lausanne, Switzerland.
and who potentially reached at least their two years
follow-up. Inclusion criteria were the presence of PD
Received 4 December 2006; Revised 20 February 2007; Accepted 23
following the United Kingdom Parkinson’s1 Disease So-
Published online 18 April 2007 in Wiley InterScience (www.
ciety Brain Bank Criteria, with untreatable motor fluc-
interscience.wiley.com). DOI: 10.1002/mds.21478
tuations and dyskinesia, without any sign atypical for PD
*Use of different variant of the same tests at each evaluation (see
at clinical examination and with at least 25% improve-
COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
ment of the Unified Parkinson’s Disease Rating Scale
cific cognitive domains, i.e., language, praxis, visual
(UPDRS) motor scale by levodopa (L-dopa) tests.2 Ex-
perception, calculation, memory, and executive func-
clusion criteria included overt ongoing psychiatric dis-
tions, using standardized tests (see Appendix) were as-
ease, severe depression (MADRS Ͼ 19), general contra-
sessed. Potential test–retest bias was considered minimal
indication to surgery, and dementia following DSM-IV
because of the large time interval between each assess-
criteria (i.e., memory impairment plus decline in one
ment. In addition, we used different variant of the same
other cognitive field with impact on daily living) or
tests at each evaluation, when available. For internation-
severe impairment (score below the 5th percentile of the
ally validated tests and for locally developed tests (“Ex-
healthy population: ՅC5) in two or more tested domains
amen Neuropsychologique du CHUV”: French version
commercially available at Division Autonome de Neu-
Clinical evaluations were made prior to surgery (mean
ropsychologie Lausanne, Switzerland),11,12 the impair-
1.7 Ϯ 2.4 months) during the “on” medication state and
ment criterion was based on the distribution (percentile)
at 3, 6, 12, 18, 24, and 36 months and once a year
of a corresponding normative sample stratified by age,
postoperation with STN-DBS turned on and under the
education, and gender. Standardization of our test battery
current medication. UPDRS I to IV and the total L-dopa
was performed on 10 healthy subjects for each decade,
equivalent dose (LED) were computed2: 100 mg* L-dopa
from 20 to 80 years old and for each education level;
with dopa-decarboxylase inhibitor ϭ 130 mg controlled
level I: Ͻ9 years of education, level II: 9 to 12 years,
release L-dopa* preparations ϭ 83 mg L-dopa with dopa-
level III: Ͼ12 years. To obtain comparable categorical
decarboxylase and COMT inhibitors (i.e., the L-dopa
data for each test we defined a 0 to 3 score: 0 ϭ normal
dosages marked by * were increased by 20% when an
performances (ϾC25: above the 25th percentile of the
inhibitor of COMT was associated) ϭ 1 mg pergolide ϭ
healthy population), 1 ϭ limited performances (ϾC10 –
1.5 mg cabergoline ϭ 1 mg lisuride ϭ 1 mg
C25: between the 25th and the 10th percentile of the
pramipexole ϭ 10 mg bromocriptine ϭ 3 mg ropinirole.
healthy population); 2 ϭ moderate impairment (ϾC5–
Presence of hallucination was assessed with the UPDRS
C10: between the 10th and the 5th percentile), 3 ϭ
I (item 2) (scores 0 and 1 ϭ absence of hallucinations,
severe impairment (ՅC5: below the 5th percentile). Fi-
scores 2, 3, and 4 ϭ presence of hallucination). This
nally, for each cognitive domain, we obtained a Cogni-
dichotomization was done since vivid dreams (score 1)
tive Index (CI), corresponding to the sum of the related
seem less specific for PD and more related to medica-
subtests. In 19 PD patients who underwent both assess-
tion.10 At each follow-up, clinical criteria for dementia
ments the same day (including 11 of the present study),
were reviewed by the neurologist and the impact of
our CI correlated linearly (r ϭ 0.89) with the Mattis
cognition on daily living was carefully discussed with
dementia rating scale (MDRS); based on this correlation,
estimated MDRS of all patients at inclusion in the
Neuropsychological tests were performed at baseline
for the 57 patients, at 6 months (5.1 Ϯ 2.3 months, range:
A trained psychiatrist made a structured clinical eval-
1.1–11.2 months) for 53 patients and at 3 years (34.3 Ϯ
uation and scored patients on the Hamilton Anxiety
13.5 months, range: 13.0 –73.9 months) for 50 patients
Rating Scales (HARS) and the Montgomery Asberg De-
(Fig. 1) by the same trained neuropsychologist. Six spe-
Statistical Analyses
Results are presented as mean Ϯ standard deviation.
Student t tests were used for normally distributed para-metric values, the Wilcoxon signed-rank test and Mann–Whitney U test were used for nonparametric data. Bon-feroni correction was applied for multiple comparisons. Significance level was established at P Ͻ 0.05. Thecumulative proportion of patients becoming dementedwas estimated using Kaplan–Meier survival analysis. The event of interest was the occurrence of dementia. The proportion of patients “surviving” at each time point
FIG. 1. Follow-up of patients. E, evaluated with detailed neuropsy-
was the proportion of patients not demented at that time.
chological testing; NE, nonevaluated with detailed neuropsychologicaltesting; PD, patients without dementia; PDD, patients with dementia.
The timing variable was the time from baseline to the
Movement Disorders, Vol. 22, No. 7, 2007
visit at which dementia was diagnosed and to the last
12.3% (Fig. 1). Incidences of dementia in the 50 patients
who underwent serial detailed neuropsychological exam-ination are 214 of 1,000 per year at 6 months and 98 of
1,000 per year (Fig. 2) at 3-years with prevalences of 9.4
At baseline, except for poor executive performance as
usually encountered in advanced PD, cognitive perfor-
At 6 months, the cognitive profile for the 53 patients
mances were normal (Table 1), and, by definition, no
who underwent neuropsychological testing declined in
patient was demented according to DSM-IV, in particu-
executive functions (especially for initiation, inhibition,
lar their cognitive status did not interfere with daily
and reasoning), for encoding and free recall capacities
living activities and they did not present significant im-
(Table 1). The 5 patients who converted to dementia
pairment in more than one cognitive field.
worsened in almost all cognitive domains, significantly
At 6-months evaluation, 5 of 57 patients (prevalence
for the global memory score (1.8 Ϯ 1.3; 7.4 Ϯ 4.2; P Ͻ
8.7%) fulfilled dementia criteria when examined by the
0.05). They ended up significantly worse than nonde-
neurologist. This represents an incidence of 202 of 1,000
mented PD in all fields (Table 2) except for the direct
per year. At 3-years, fourteen patients (prevalence of
digit span and ideomotor praxis. The 48 nondemented
24.5%) were demented, representing an incidence of 89
patients worsened in executive functions only (6.2 Ϯ 5.0;
of 1,000 per year from baseline. Between 6 months and
7.3 Ϯ 5.2; P Ͻ 0.05) [particularly initiation (1.7 Ϯ 2.1,
3 years, 5 patients died without having the long-termdetailed neuropsychological evaluation. They were clin-
ically evaluated in average 8.5 months before their death:
At 3-years, the 50 patients who underwent neuropsy-
none presented DSM-IV criteria of dementia at that time.
chological testing worsened significantly in memory,
They did neither differ from PD for the cognitive profile
particularly encoding capacities and inverse digit span,
at baseline and at 6 months, nor for its evolution between
executive functions, inhibition, attention, and in con-
structive praxis (Table 1). The 14 patients who converted
Four of the nondemented patients were not examined
to dementia significantly worsened from baseline in all
with detailed neuropsychological testing at the 6-months
tested functions (Table 2) except for the language, direct
follow-up (3 refused, 1 had systemic infection): all were
digit span, and calculation; they performed significantly
examined at 3-year and were not demented at that point.
worse than PD in all fields (Table 2). After excluding
At 3-years, 7 patients were not examined in detail (5
these 14 patients, the remaining 36 PD patients who did
died, 1 refused, 1 moved to another country), represent-
not develop dementia had a neuropsychological profile
ing a drop out for detailed neuropsychological testing of
(Table 2) similar to the preoperative evaluation except
TABLE 1. Cognitive profile of the whole cohort
aP Ͻ 0.05 compared to baseline.
bP Ͻ 0.05 comparing 6 mo to 3 yr.
cP Ͻ 0.01 compared to baseline.
dP Ͻ 0.01 comparing 6 mo to 3 yr. CI, cognitive index; ϾC10, with scores above the 10th percentile. Movement Disorders, Vol. 22, No. 7, 2007COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
The 14 patients developing dementia worsened in allcognitive fields, significantly for constructive praxis,ideomotor praxis, calculation, inverse digit span, mem-ory (particularly encoding). The rest of the cohortshowed only a significant worsening for executive func-tions (inhibition) and inverse digit span.
Patients who developed dementia were similar to the
rest of the cohort for gender, duration of PD, baselineUPDRS III, LED, psychiatric profiles (except hallucina-tions) and the preoperative cognitive evaluation exceptexecutive functions (Table 2). The two groups had sim-ilar evolution for anxiety (HARS), depression (MADRS)and motor outcomes (Table 3). Correct electrodes posi-tioning were confirmed in the 12 patients who developeddementia and who were controlled by postoperative MRI(performed routinely since 2000). No persistent compli-cation occurred in either group. Transient complicationscomprised 4 confusions (1 in PDD, 3 in PD), one hypo-natremia and one acute paranoid state, both in PD.
At baseline, patients who subsequently developed de-
Kaplan-Meier curve of the incidence of dementia. y-axis:
mentia differed from the rest of the cohort only by an
Proportion of PD without dementia; x-axis: Time course after the
older age, presence of more hallucinations, and poorer
operation (months). Each step down represents one patient who devel-oped dementia and each cross represents the time point of the last
executive functions especially inhibition and initiation
follow-up for each patient who did not develop dementia.
(Tables 2 and 3). However, there was important overlapsbetween PDD and PD groups for these scores preventing
for inhibition, which significantly worsened (3.2 Ϯ 2.7;
them to be good preoperative predictors (Fig. 3). Even
score combining these three risk factors did not reach
Over the 28 Ϯ 14 months between the two postoper-
40% sensitivity for prediction of postoperative dementia.
ative follow-ups, the whole cohort had a worsening of
We analyzed the risk profile of the 5 patients who died
inhibition, inverse digit span, memory (particularly rec-
before the long-term neuropsychological testing; they were
ognition), constructive praxis, and calculation (Table 1).
older (mean 68.6 years), none of them had hallucinations. TABLE 2. Cognitive differences between PD and PDD at 6 mo and at 3 yr
aP Ͻ 0.05 between PD and PDD.
bP Ͻ 0.01 between PD and PDD.
cP Ͻ 0.05 compared to baseline. Movement Disorders, Vol. 22, No. 7, 2007TABLE 3. Neurological and psychiatric data
aP Ͻ 0.05 comparing PD and PDD. DISCUSSION
cognitive tests potentially leading to different exclusion
We found that, in spite of current selection criteria,
criteria for cognition. However, CAPSIT17 criteria, pub-
excluding demented patients from STN-DBS, 28% de-
lished after we started our long-term prospective follow-
veloped dementia over three-year follow-up, leading to a
up, proposed a cut-off score of 120 on the MDRS. This
postoperative dementia incidence between 89 and 98 of
corresponds to a clinical state of dementia that is very
1,000 per year (clinical versus detailed neuropsycholog-
similar to what we obtain by applying the DMS-IV
ical evaluation). Potential confounders, such as depres-
criteria for dementia in addition to our extensive battery
sion or anxiety,13 were excluded by psychiatric exami-
of neuropsychological tests (patients with a severe deficit
nations and mood scores. These estimated incidences are
(ՅC5) in more than one domain being excluded).
higher than those reported in other studies with a range
Such variability in the estimates of dementia incidence
between 24 and 46 of 1,000 per year over 3 to 5
in PD has also been observed, with similar range, in
years.1,9,14 An explanation for such differences relies in
studies dealing with medically treated patients (42.6 to
the average age of these cohorts (55 to 59 years),
112 of 1,000 per year).8 Even if comparison with com-
younger than our (64 year): age being one of the main
munity-based studies should be regarded cautiously,
determinant for the future development of dementia.15,16
such similarities of incidence estimates may suggest that
Another possible factor involves the use of different
the occurrence of dementia after STN-DBS corresponds
FIG. 3. Baseline findings associated with postoperative dementia. Patients who did not develop dementia (PD: black circles) are compared with those who developed it (PDD), at 6 months (white circles) or thereafter (crosses). (A) Base- line Executive function score; (B) Base- line Hallucination score; (C) Age at op- eration. Although means (black squares) and SD (error bars) lead to significant differences, there is a substantial overlap, preventing discrimination between the two groups. In addition, there is no dif- ference between PDD developing de- mentia at 6 months and those developing it at 3 years. Movement Disorders, Vol. 22, No. 7, 2007COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
to the natural evolution of PD rather than as a conse-
Stroop test. Here again the interpretation of this execu-
quence of the surgery. This is also supported by the
tive decline in operated PD should be cautious as med-
stability over 3 years of the neuropsychological profile in
ically treated patients may also display such a decline
patients not developing dementia with only minimal im-
and the operation may have only precipitated it.
pairment of executive functions as can be expected from
With such potential precipitating effect of STN-DBS
the natural evolution of medically treated nondemented
on dementia in at-risk patients, it might be desirable to
refine selection criteria to avoid operating patients at risk
In contrast to the long term follow-up results, we
of such poor cognitive outcome. We were not able to
found that 9.4% of patients developed dementia within 6
identify predictors of early dementia (6 months) and this
months from implantation (36% developing postopera-
might be due to the small number of patients involved
tive dementia) representing an incidence of 214 of 1,000
(Fig. 3). For long-term dementia (3 years) the patients
per year, twice as high as the biggest rate ever reported
who will develop dementia were significantly older,
in medically treated patients. Those early-demented pa-
scored worse in executive functions and presented more
tients did not suffer from specific surgery complication
frequently hallucinations preoperatively than those who
(transient confusion or infection) and this raises the ques-
did not develop dementia. These risk factors are similar
tion of a direct impact of STN-DBS on cognition, at least
to those predicting dementia in medically treated PD.20,27
in some patients. Such early postoperative increase of
However none of them allows discriminating between
dementia incidence has been reported in other series with
pre-PDD and PD patients, as substantial overlap exists
figures between 5.8% at 13 weeks postop21 and 30% at 3
(Fig. 3). Even the combination of 3 risk factors allowed
months.6 Direct comparison to medically treated PD has
prediction of only part of the occurrence of dementia
also recently confirmed a larger decline in executive
when excluding any nondemented PD was avoided. As
function at 6 months in DBS treated patients,22 in keep-
we found hallucinations, based only on UPDRS defini-
ing with our observation. In this latter study, three cases
tion, having the better discriminating potential, an ex-
of dementia resulted from surgical complications (2 elec-
panded evaluation of this risk factor seems desirable in
trode misplacements, 1 hemorrhage) but the larger de-
cline in DBS treated patients was maintained after ex-
Such potential baseline predictors may help us in the
clusion of these patients. These results suggest that the
evaluation of the risk for further development of demen-
operation itself may trigger the occurrence of dementia
tia after STN-DBS to better inform patients and caregiv-
in at-risk patients. Such effect might be nonspecific as
ers. They should not be understood yet as exclusion
cognition has been showed to be altered in all types of
criteria, since such criteria should also take into account
surgery (not only brain surgery)23 leading to a transient
global evaluation of quality of life and daily function of
cognitive decline followed by a recovery at 2 years in
patients and balance these risks with the benefits from
healthy elderly populations. With PD leading to progres-
motor improvement. Our study does not include such
sive cognitive decline in the vast majority of patients,
systematic analysis but 5 of the patients who developed
such return to the baseline of the cognitive status cannot
dementia where included in our recently published pro-
be expected in our patients but rather a return to the
spective study28; in contrast to the improvement of qual-
natural evolution, including persistence of dementia.
ity of life as measured by the Parkinson’s disease Ques-
In addition to such potential effect of the intervention,
tionnaire (39)29 reported by the other PD patients, the 5
we found a slow worsening of executive functions in the
patients who developed dementia reported a trend to
whole cohort over the 3 years, in agreement with other
authors. Saint-Cyr et al. evaluated eleven patients be-
In conclusion, the 3-year cognitive follow-up of our
tween 3 and 12 months postoperation5 and demonstrated
longitudinal cohort revealed an incidence of dementia
a negative impact of STN-DBS on executive functions,
after STN-DBS similar to those reported in medically
mostly letter fluency (initiation) and Trail making test
treated patients. However, 36% of patients developing
(TMT) B (inhibition). Those two functions have been
dementia did so within 6 months from implantation sug-
reported to be sensitive to STN-DBS implantation since
gesting a precipitating effect of the stimulation either
it might interfere with frontal cortico-subcortical loops24
nonspecifically or by interference with the frontal cog-
as shown by PET studies.25 However a direct effect of
nitive loops. The identification of predictors (older age,
the stimulation itself is still a matter of controversy22,26
presence of hallucination, and poorer baseline executive
since no differences were seen when stimulation was
functions) may help a better patient selection and infor-
turned OFF to ON, 3 and 12 months postoperatively for
mation concerning the risk of poor cognitive outcome.
verbal fluency and even an improvement was seen in
However the low sensitivity of the prediction calls for
Movement Disorders, Vol. 22, No. 7, 2007
further studies to better delineate risk factors for devel-
Reasoning: Similarities subtest of the WAIS-III, Piaget’s
reasoning task (patient is asked to draw the liquid levelof four bottles in different positions). APPENDIX REFERENCES Cognitive Assessment
1. Krack P, Batir A, Van Blercom N, et al. Five-year follow-up of
bilateral stimulation of the subthalamic nucleus in advanced Par-kinson’s disease. N Engl J Med 2003;349:1925-1934.
Part I (reading) and Part II (naming) of the animal Stroop
2. Vingerhoets FJ, Villemure JG, Temperli P, Pollo C, Pralong E,
Ghika J. Subthalamic DBS replaces levodopa in Parkinson’s dis-ease: two-year follow-up. Neurology 2002;58:396-401.
Boston Naming Test (number of items correctly stated)*
3. Alegret M, Junque C, Valldeoriola F, et al. Effects of bilateral
subthalamic stimulation on cognitive function in Parkinson dis-
ease. Arch Neurol 2001;58:1223-1227.
4. Ardouin C, Pillon B, Peiffer E, et al. Bilateral subthalamic or
Constructive praxis: copy from four ADAS figures
pallidal stimulation for Parkinson’s disease affects neither memory
nor executive functions: a consecutive series of 62 patients. Ann
Ideomotor praxis: four pantomime of object use (number
5. Saint-Cyr JA, Trepanier LL, Kumar R, Lozano AM, Lang AE.
Neuropsychological consequences of chronic bilateral stimulationof the subthalamic nucleus in Parkinson’s disease. Brain 2000;123
6. Dujardin K, Defebvre L, Krystkowiak P, Blond S, Destee A.
Discrimination of four overlapping figures (Poppel-
Influence of chronic bilateral stimulation of the subthalamic nu-
reuter) (number of items correctly stated)*
cleus on cognitive function in Parkinson’s disease. J Neurol 2001;248:603-611.
Recognition of five famous faces (number of items cor-
7. Trepanier LL, Kumar R, Lozano AM, Lang AE, Saint-Cyr JA.
Neuropsychological outcome of GPi pallidotomy and GPi or STN
Pointing at the location of five main cities on the map of
deep brain stimulation in Parkinson’s disease. Brain Cogn 2000;42:324-347.
Switzerland (number of items correctly stated)
8. Aarsland D, Andersen K, Larsen JP, Lolk A, Nielsen H, Kragh-
Sorensen P. Risk of dementia in Parkinson’s disease: a community-
based, prospective study. Neurology 2001;56:730-736.
9. Funkiewiez A, Ardouin C, Caputo E, et al. Long term effects of
Four elementary oral calculations and one written mul-
bilateral subthalamic nucleus stimulation on cognitive function,
tiplication (number of items correctly stated)*
mood, and behaviour in Parkinson’s disease. J Neurol NeurosurgPsychiatry 2004;75:834-839.
10. Aarsland D, Larsen JP, Cummins JL, Laake K. Prevalence and
clinical correlates of psychotic symptoms in Parkinson disease: a
Immediate memory: direct digit span (number of maxi-
community-based study. Arch Neurol 1999;56:595-601.
11. Assal G. Batterie des examens Neuropsychologiques du CHUV.
Division Autonome de Neuropsychologie, 1985.
Working memory: inverse digit span (number of maxi-
12. Bindschaedler C, Assal G, de Tribolet N. Cognitive sequelae
following rupture of aneurysms of the anterior communicatingartery and the anterior cerebral artery. Retrospective study of 56
Encoding, retrieval capacities and recall memory capac-
cases. Rev Neurol (Paris) 1997;153:669-678.
ities: Rey’s auditory-verbal learning test (number of
13. Troster AI, Stalp LD, Paolo AM, Fields JA, Koller WC. Neuro-
items encoded after repeated trials, number of items
psychological impairment in Parkinson’s disease with and withoutdepression. Arch Neurol 1995;52:1164-1169.
recognized, number of items spontaneously recalled)*
14. Rodriguez-Oroz MC, Obeso JA, Lang AE, et al. Bilateral deep
brain stimulation in Parkinson’s disease: a multicentre study with
4 years follow-up. Brain 2005;128 (Part 10):2240-2249.
15. Athey RJ, Porter RW, Walker RW. Cognitive assessment of a
Initiation: Verbal fluency: literal (M words) and categor-
representative community population with Parkinson’s disease
ical (animals) (number of items stated in 1 min),
(PD) using the Cambridge Cognitive Assessment-Revised (CAM-
Nonverbal fluency: drawing of different figures (num-
16. Hobson P, Meara J. Risk and incidence of dementia in a cohort of
older subjects with Parkinson’s disease in the United Kingdom.
Inhibition and planning: Stroop naming part III (time
scored), Visual antisaccades (10 stimuli on each side),
17. Defer GL, Widner H, Marie RM, Remy P, Levivier M. Core
assessment program for surgical interventional therapies in Parkin-
TMT (part B) (time and error scored), Luria graphic
son’s disease (CAPSIT-PD). Mov Disord 1999;14:572-584.
sequences (number of items consecutively correctly
18. Marinus J, Visser M, Verwey NA, et al. Assessment of cognition
in Parkinson’s disease. Neurology 2003;61:1222-1228.
19. Jacobs DM, Marder K, Cote LJ, Sano M, Stern Y, Mayeux R.
Attention: TMT part A (time scored), Code subtest of the
Neuropsychological characteristics of preclinical dementia in Par-
kinson’s disease. Neurology 1995;45:1691-1696. Movement Disorders, Vol. 22, No. 7, 2007COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
20. Stern Y, Tang MX, Jacobs DM, et al. Prospective comparative
25. Schroeder U, Kuehler A, Haslinger B, et al. Subthalamic nucleus
study of the evolution of probable Alzheimer’s disease and Par-
stimulation affects striato-anterior cingulate cortex circuit in a
kinson’s disease dementia. J Int Neuropsychol Soc 1998;4:279-
response conflict task: a PET study. Brain 2002;125 (Part 9):1995-
21. Morrison CE, Borod JC, Perrine K, et al. Neuropsychological
26. Pillon B, Ardouin C, Damier P, et al. Neuropsychological changes
functioning following bilateral subthalamic nucleus stimulation
between “off” and “on” STN or GPi stimulation in Parkinson’s
in Parkinson’s disease. Arch Clin Neuropsychol 2004;19:165-
27. Mahieux F, Fenelon G, Flahault A, Manifacier MJ, Michelet
22. Smeding HM, Speelman JD, Koning-Haanstra M, et al. Neuropsy-
D, Boller F. Neuropsychological prediction of dementia in
chological effects of bilateral STN stimulation in Parkinson dis-
Parkinson’s disease. J Neurol Neurosurg Psychiatry 1998;64:
ease: a controlled study. Neurology 2006;66:1830-1836.
23. Abildstrom H, Rasmussen LS, Rentowl P, et al. Cognitive dys-
function 1-2 years after non-cardiac surgery in the elderly. IS-
28. Gronchi-Perrin A, Viollier S, Ghika J, et al. Does subthalamic
POCD group. International Study of Post-Operative Cognitive
nucleus deep brain stimulation really improve quality of life in
Dysfunction. Acta Anaesthesiol Scand 2000;44:1246-1251.
Parkinson’s disease? Mov Disord 2006;21:1465-1468.
24. Schroeder U, Kuehler A, Lange KW, et al. Subthalamic nucleus
29. Auquier P, Sapin C, Ziegler M, et al. Validation of the French
stimulation affects a frontotemporal network: a PET study. Ann
language version of the Parkinson’s Disease Questionnaire - PDQ-
39. Rev Neurol (Paris) 2002;158:41-50. Movement Disorders, Vol. 22, No. 7, 2007
Marginal annotations on the classification of plants found in Christoph Jakob Trew’s Plantae selectae (1750-1773) [Norimbergae] [Nuremberg]: s.n., 1750 (-1773). The annotations are found in copy 1 of this work. NB. Plates 101-120 form the Supplementum to Plantae Selectae (1790) Trew’s title Annotations in copy 1 Modern name if different Cedrus foliis rigidis acumina
REPUBLICA DE CHILE PADRON ELECTORAL AUDITADO - ELECCIONES PRESIDENCIAL, PARLAMENTARIAS Y DE CONSEJEROS REGIONALES 2013 SERVICIO ELECTORAL AISEN DEL GRAL. CARLOS IBAÑEZ LAGO VERDE PROVINCIA COYHAIQUE C.IDENTIDAD SEX DOMICILIO ELECTORAL CIRCUNSCRIPCION ABUFHELE BORQUEZ VALERIE CONSTANZA 15.758.097-3 CARMEN ARIAS N° 18 VILLA AMENGUAL LA TAPERA LA TAPERA A
 COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
ment of the Unified Parkinson’s Disease Rating Scale
cific cognitive domains, i.e., language, praxis, visual
(UPDRS) motor scale by levodopa (L-dopa) tests.2 Ex-
perception, calculation, memory, and executive func-
clusion criteria included overt ongoing psychiatric dis-
tions, using standardized tests (see Appendix) were as-
ease, severe depression (MADRS Ͼ 19), general contra-
sessed. Potential test–retest bias was considered minimal
indication to surgery, and dementia following DSM-IV
because of the large time interval between each assess-
criteria (i.e., memory impairment plus decline in one
ment. In addition, we used different variant of the same
other cognitive field with impact on daily living) or
tests at each evaluation, when available. For internation-
severe impairment (score below the 5th percentile of the
ally validated tests and for locally developed tests (“Ex-
healthy population: ՅC5) in two or more tested domains
amen Neuropsychologique du CHUV”: French version
commercially available at Division Autonome de Neu-
Clinical evaluations were made prior to surgery (mean
ropsychologie Lausanne, Switzerland),11,12 the impair-
1.7 Ϯ 2.4 months) during the “on” medication state and
ment criterion was based on the distribution (percentile)
at 3, 6, 12, 18, 24, and 36 months and once a year
of a corresponding normative sample stratified by age,
postoperation with STN-DBS turned on and under the
education, and gender. Standardization of our test battery
current medication. UPDRS I to IV and the total L-dopa
was performed on 10 healthy subjects for each decade,
equivalent dose (LED) were computed2: 100 mg* L-dopa
from 20 to 80 years old and for each education level;
with dopa-decarboxylase inhibitor ϭ 130 mg controlled
level I: Ͻ9 years of education, level II: 9 to 12 years,
release L-dopa* preparations ϭ 83 mg L-dopa with dopa-
level III: Ͼ12 years. To obtain comparable categorical
decarboxylase and COMT inhibitors (i.e., the L-dopa
data for each test we defined a 0 to 3 score: 0 ϭ normal
dosages marked by * were increased by 20% when an
performances (ϾC25: above the 25th percentile of the
inhibitor of COMT was associated) ϭ 1 mg pergolide ϭ
healthy population), 1 ϭ limited performances (ϾC10 –
1.5 mg cabergoline ϭ 1 mg lisuride ϭ 1 mg
C25: between the 25th and the 10th percentile of the
pramipexole ϭ 10 mg bromocriptine ϭ 3 mg ropinirole.
COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
ment of the Unified Parkinson’s Disease Rating Scale
cific cognitive domains, i.e., language, praxis, visual
(UPDRS) motor scale by levodopa (L-dopa) tests.2 Ex-
perception, calculation, memory, and executive func-
clusion criteria included overt ongoing psychiatric dis-
tions, using standardized tests (see Appendix) were as-
ease, severe depression (MADRS Ͼ 19), general contra-
sessed. Potential test–retest bias was considered minimal
indication to surgery, and dementia following DSM-IV
because of the large time interval between each assess-
criteria (i.e., memory impairment plus decline in one
ment. In addition, we used different variant of the same
other cognitive field with impact on daily living) or
tests at each evaluation, when available. For internation-
severe impairment (score below the 5th percentile of the
ally validated tests and for locally developed tests (“Ex-
healthy population: ՅC5) in two or more tested domains
amen Neuropsychologique du CHUV”: French version
commercially available at Division Autonome de Neu-
Clinical evaluations were made prior to surgery (mean
ropsychologie Lausanne, Switzerland),11,12 the impair-
1.7 Ϯ 2.4 months) during the “on” medication state and
ment criterion was based on the distribution (percentile)
at 3, 6, 12, 18, 24, and 36 months and once a year
of a corresponding normative sample stratified by age,
postoperation with STN-DBS turned on and under the
education, and gender. Standardization of our test battery
current medication. UPDRS I to IV and the total L-dopa
was performed on 10 healthy subjects for each decade,
equivalent dose (LED) were computed2: 100 mg* L-dopa
from 20 to 80 years old and for each education level;
with dopa-decarboxylase inhibitor ϭ 130 mg controlled
level I: Ͻ9 years of education, level II: 9 to 12 years,
release L-dopa* preparations ϭ 83 mg L-dopa with dopa-
level III: Ͼ12 years. To obtain comparable categorical
decarboxylase and COMT inhibitors (i.e., the L-dopa
data for each test we defined a 0 to 3 score: 0 ϭ normal
dosages marked by * were increased by 20% when an
performances (ϾC25: above the 25th percentile of the
inhibitor of COMT was associated) ϭ 1 mg pergolide ϭ
healthy population), 1 ϭ limited performances (ϾC10 –
1.5 mg cabergoline ϭ 1 mg lisuride ϭ 1 mg
C25: between the 25th and the 10th percentile of the
pramipexole ϭ 10 mg bromocriptine ϭ 3 mg ropinirole.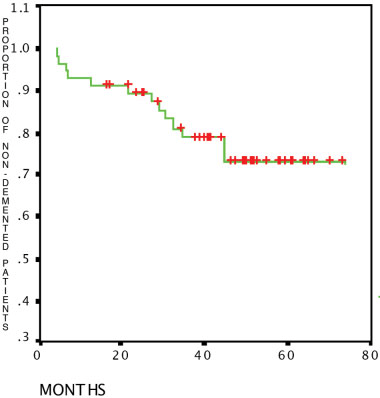 COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
The 14 patients developing dementia worsened in allcognitive fields, significantly for constructive praxis,ideomotor praxis, calculation, inverse digit span, mem-ory (particularly encoding). The rest of the cohortshowed only a significant worsening for executive func-tions (inhibition) and inverse digit span.
COGNITIVE PROFILE AND INCIDENCE OF DEMENTIA
The 14 patients developing dementia worsened in allcognitive fields, significantly for constructive praxis,ideomotor praxis, calculation, inverse digit span, mem-ory (particularly encoding). The rest of the cohortshowed only a significant worsening for executive func-tions (inhibition) and inverse digit span.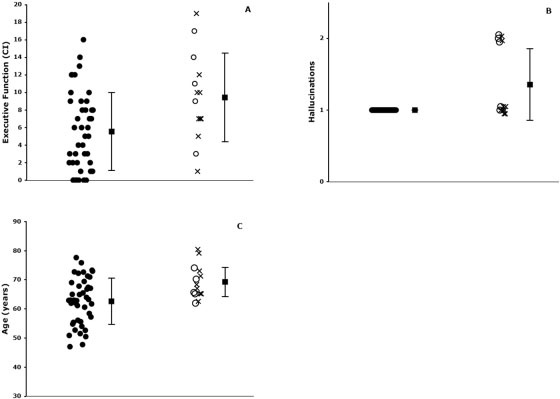 TABLE 3. Neurological and psychiatric data
TABLE 3. Neurological and psychiatric data