State of the Art in Clinical and Anatomic Pathology Diagnosing Allergic Diseases in Children Practical Recommendations for Consulting Pathologists
● In the environment of managed care, children with al-
form of allergic disease.2–4 This estimate includes children
lergic diseases are increasingly likely to be evaluated by
with cutaneous disease (atopic dermatitis), gastrointesti-
nonallergist physicians. While the presumptive diagnosis of
nal disease, and allergic respiratory diseases (chronic oti-
an allergic disease can often be suspected on clinical
tis, allergic rhinitis, and asthma). According to recent data,
grounds, signs and symptoms are not reliable for establish-
more than 31 million individuals in the United States suf-
ing a definitive diagnosis or for deciding on management
fer from asthma, more than 9 million of whom are chil-
options. This article discusses the use of immunoglobulin E
dren.5 Recent epidemiological studies point to an alarm-
antibody tests to classify children with allergic symptoms.
ing increase in the incidence of asthma.2,3 Like many large
The information is intended for pathologists who offer con-
categories of disease, estimates of the total yearly cost of
sultative laboratory services to nonallergist physicians. Em- phasis is placed on defining the minimum number of tests
allergic diseases run to the tens of billions of dollars. Tak-
necessary to identify allergic children at different ages.
en collectively, allergic diseases are a major public health
(Arch Pathol Lab Med. 2004;128:1028–1031)
While these statistics are impressive in their magnitude,
they do not constitute a rationale for more diagnostic test-
Laboratory tests for allergic diseases have been available ing, and they do not point to a particular need for pa-
for more than 30 years.1 During this time, most pa-
thologists to become involved in the care of patients with
thologists have had little interest in the field of allergic
allergic diseases. The principal impetus for involving pa-
disease diagnosis nor could it be argued that detailed
thologists in the care of children with allergic diseases
knowledge of allergic diseases was required to function
comes from systematic changes in the way in which pa-
effectively as a practicing pathologist. Following their in-troduction in the 1970s, laboratory tests for allergic dis-
tients gain access to health care services. In past years, it
eases, including tests for immunoglobulin E protein (IgE)
was often possible for children with signs and symptoms
and allergen-specific IgE antibodies (IgE antibodies), were
suggestive of allergy to be seen by an allergy specialist
usually performed in physician’s office laboratories or
without prior medical evaluation. This is no longer true
commercial laboratories. Many hospital clinical laborato-
for many patients. In the current environment of managed
ries only performed measurements of IgE total protein,
care, it is customary for a patient to be seen initially by a
and pathologists were seldom called on to consult on the
primary care physician, who must decide to manage the
ordering of tests for IgE antibodies or the meaning of test
patient within the practice or seek a referral to an allergy
results. With this history, it is logical to ask, ‘‘What has
specialist for further evaluation. In this paradigm, labo-
changed, and why should practicing pathologists have
ratory tests that establish a high likelihood of allergic dis-
more knowledge of this field today than in the past?’’ This
ease take on increased importance, and pathologists have
article addresses these questions and provides practical
an important role as consultants to nonallergist physi-
information for pathologists who are called on to assist
cians, many of whom have limited knowledge about these
nonallergist physicians in the evaluation of children with
It is often not possible to make an accurate diagnosis of
BURGEONING CLINICAL NEEDS, CHANGING ACCESS
an allergic disease on clinical grounds alone. The results
TO CAREGIVERS, AND THE ROLE OF THE
of clinical studies suggest that the medical history and
CONSULTING PATHOLOGIST
physical examination alone lead to a correct diagnosis of
Allergic diseases are prevalent in children and adults.
allergic disease in only about 50% of cases.4 Clearly, ad-
Research indicates that up to 30% of children have some
ditional objective data are needed to establish the pre-sumptive diagnosis of an allergic disease or to rule it out.
Accepted for publication April 27, 2004.
It is in this context that pathologists can anticipate the
From the Department of Laboratory Medicine, Mayo College of Med-
following questions from nonallergist physicians: what is
icine and Mayo Graduate School of Medicine, Rochester, Minn.
the role of pretreatment diagnostic testing in children sus-
The author has no relevant financial interest in the products or com-
pected of having an allergic disease, which children
should be tested, which allergens should I choose, how do
Reprints: Henry A. Homburger, MD, Department of Laboratory Med-
icine, Mayo College of Medicine and Mayo Graduate School of Med-
the tests offered today differ from the previous genera-
icine, 210 Hilton Bldg, Rochester, MN 55905 (e-mail: homburger.
tions of tests, and how do I interpret the results? While
there are many nuances to this subspecialty area of clin-
1028 Arch Pathol Lab Med—Vol 128, September 2004
Diagnosing Allergic Diseases in Children—Homburger
ical pathology, the answers to these basic questions are
quent offending allergens in infants and children younger
than 3 years of age are foods, notably protein allergens incow’s milk, egg white, wheat, and soy.9,10 Immediate hy-
THE NATURAL HISTORY OF ALLERGIC DISEASES
persensitivity to food allergens in infancy is commonly
IN CHILDREN
associated with atopic dermatitis, gastrointestinal symp-
Implications for Diagnostic Testing
toms, chronic otitis, and wheezing. Less commonly, se-
Children who are genetically predisposed to develop
verely atopic children younger than 3 years may already
allergic diseases (so-called atopic children) often develop
have demonstrable IgE antibodies to house dust mites
symptoms and signs of disease in a predictable sequence
(Dermatophagoides farinae and Dermatophagoides pteronyssi-
as they progress throughout childhood. This concept has
nus). These inhalant allergens are a common cause of asth-
been called the ‘‘allergy march.’’ 6 In genetically predis-
ma in older children. Except for the rare occurrence of a
posed infants, eczema (atopic dermatitis) is often the first
child with anaphylaxis whose symptoms are strongly as-
manifestation of allergic disease. A pruritic rash that in-
sociated with the ingestion of a particular food, for ex-
volves the cheeks, neck, chest, and the extensor surfaces
ample, peanut, it is seldom necessary to test for additional
of the arms and legs characterizes this disease. Atopic in-
IgE antibodies if the results of tests to the common food
fants and children younger than 3 years of age may also
allergens are negative. In addition, allergic respiratory dis-
have gastrointestinal symptoms (colic, diarrhea, vomiting,
ease caused by common inhalant allergens, such as pol-
and abdominal pain) or suffer from chronic otitis. Less
lens and molds, is uncommon prior to age 3, and routine
commonly, children younger than 3 years may already
testing for IgE antibodies to these allergens is not rou-
suffer from recurrent wheezing. As the atopic child ma-
tinely useful. In the age group younger than 3 years, the
tures, cutaneous and gastrointestinal symptoms often give
presumptive diagnosis of an allergic disease can be estab-
way to worsening respiratory symptoms with develop-
lished with tests for IgE antibodies to common foods and
ment of allergic rhinitis and asthma. The entire sequence
dust mite allergens. Positive test results for IgE antibodies
of the allergy march is shown schematically in Figure 1.
to these allergens have dual significance; they establish a
Regardless of age, the presenting symptoms of allergic
strong likelihood of immediate hypersensitivity disease,
disease in children are not specific for immediate hyper-
and they indicate an increased risk of sensitization to ad-
sensitivity and are easily mistaken for other etiologies. It
ditional allergens later in childhood.9 For these reasons,
is in this context that laboratory testing is important to
the identification of IgE antibodies to common food aller-
make an accurate diagnosis and to guide optimum ther-
gens in symptomatic infants and children younger than 3
apy. The alternative is to treat empirically with no clear
years is important for making proper treatment choices
idea of the etiology of disease or to make referrals to an
and for deciding to seek a referral to an allergy specialist.
allergy specialist without first establishing a strong like-
In children younger than 3 years, it is often more con-
lihood of an allergic etiology. Increasingly, physicians have
venient to test sera for the presence of IgE antibodies than
recognized that empiric therapy of suspected allergic dis-
to perform skin-prick tests. The presence of widespread
eases is not acceptable because it often results in unnec-
cutaneous disease impairs the reliability of skin tests. The
essary or inappropriate treatment with antihistamines, in-
levels of IgE antibodies that predict clinically significant,
haled or systemic corticosteroids, and antibiotics. Worse
immediate hypersensitivity with high positive predictive
yet, empiric therapy allows the allergy march to proceed
values differ somewhat for different foods, and the clinical
unchecked by missing the opportunity to lessen exposure
significance of low levels of IgE antibodies to common
to offending allergens. While the results of clinical inves-
foods is limited (Figure 2).11 Nevertheless, it is clear from
tigations are not yet conclusive, there is strong suggestive
the relationships shown in Figure 2 that the higher the
evidence that avoidance of offending allergens and opti-
level of IgE antibodies, the greater the likelihood of clini-
mum pharmacotherapy may lessen the risk of sensitiza-
cally significant sensitivity to each food allergen. Note also
tion to additional allergens and interrupt the progression
that the levels of IgE antibodies are expressed on a con-
to serious allergic respiratory diseases later in childhood.7,8
tinuous scale in Figure 2. This reflects the fact that unlikeearly versions of the IgE antibody test, newer generations
WHICH CHILDREN SHOULD BE TESTED, WHICH TESTS
of this test available from some manufacturers yield quan-
SHOULD BE ORDERED, AND WHAT DO THE
titative results that are expressed in mass units of concen-
RESULTS MEAN?
tration. It is important to maximize the usefulness of test
In a recent consensus document, the European Acade-
results by choosing a method that provides quantitative
my of Allergy and Clinical Immunology made the follow-
results.12 The College of American Pathologists Diagnostic
Allergy Survey summarizes results reported by subscrib-ing laboratories on proficiency test samples. This survey
Generally, all individuals with severe, persisting or recurrent
is a useful guide to those methods that express results in
possible ‘‘allergic symptoms’’ and individuals with need for con-
mass units. For pathologists who are considering estab-
tinuous prophylactic treatment should be tested for specific al-
lishing IgE antibody testing in their own facilities, it is
lergy irrespective of the age of the child.
important to choose a quantitative method, and for those
Included in this description are children with cutaneous
pathologists who refer specimens to a commercial refer-
disease, gastrointestinal symptoms (colic, diarrhea, vom-
ence laboratory, it is important to verify that the method
iting, or failure to thrive), recurrent wheezing, otitis, rhi-
nitis, or asthma. Laboratory tests for IgE antibodies and
Allergic diseases in children older than 3 years typically
skin tests were considered essentially interchangeable for
manifest with respiratory signs and symptoms, including
the purpose of evaluating such children.
rhinitis, wheezing, and persistent cough (Figure 1). From
The selection of appropriate allergens for testing is de-
the standpoint of immediate hypersensitivity diseases, it
termined primarily by the age of the child. The most fre-
is useful to think of the entire respiratory tract as a single
Arch Pathol Lab Med—Vol 128, September 2004
Diagnosing Allergic Diseases in Children—Homburger 1029 Figure 1. Relationship of age and manifes- tations of allergic disease in children. Solid line indicates retrospective study; dashed line, prospective study. Figure 2. Probability of reacting to a food at a given concentration of immunoglobulin E (IgE) antibody.11 Solid line indicates retrospec- tive study; dashed line, prospective study. Selected Immunoglobin E Antibody Tests for Evaluating Children With Clinical Signs of Allergy Signs of Disease Allergens
Common foods: egg white, milk, wheat, soy; house
dust mites (Dermatophagoides farinae and Derma-tophagoides pteronyssinus)
Common perennial inhalants: house dust mites, cat
Common perennial inhalants, as above, plus pollen
target organ. Allergic rhinitis and asthma often accom-
small panels of individual inhalant allergens and use of
pany one another. Most asthmatic children also suffer
the multiallergen IgE antibody test to test for several an-
from rhinitis, and children with rhinitis often have asthma
that is either clinically apparent or subclinical.2 With the
The allergens chosen for testing in children with respi-
development of disease affecting the respiratory tract,
ratory diseases depend on the age of the child and the
tests for IgE antibodies to inhalant allergens become much
scope of clinical manifestations (Table). After age 3 or 4,
more important for clinical decision making.4 Since there
it is common in atopic children to develop IgE antibodies
are a vast number of different inhalant allergens available
to indoor inhalant allergens, including house dust mites,
for testing, it is important to be selective in the initial test-
animal epithelia (cat and dog), and cockroach. The last
ing of children with respiratory signs and symptoms to
allergen specificities to develop in children are IgE anti-
avoid unnecessary testing. Data from clinical investiga-
bodies to common outdoor inhalant allergens, including
tions support 2 complementary approaches: the use of
molds and pollen inhalants of trees, grasses, and weeds. 1030 Arch Pathol Lab Med—Vol 128, September 2004
Diagnosing Allergic Diseases in Children—Homburger
There is no universal agreement on the minimum number
that allergen sensitization and the clinical manifestations
of inhalant allergens that should be tested when evaluat-
of allergic disease occur in a predictable sequence directly
ing children with respiratory symptoms, but there is con-
related to age in children genetically predisposed to aller-
sensus that testing should include house dust mites, cat or
gy. The recommendations for testing reflect the conclu-
dog epithelium, a ubiquitous mold species (eg, Alternaria
sions of published, peer-reviewed clinical studies, and
tenuis), and appropriate pollen allergens.4 Testing for IgE
they recognize that nonallergist physicians perform the
antibodies to pollen allergens is indicated in older chil-
initial clinical evaluations of many children with possible
dren, especially if symptoms are seasonal and tests can
allergic diseases. Since the clinical diagnosis of allergic
be performed at the time that symptoms are manifest. It
disease is often not reliable, decisions about allergen
is well known that the levels of IgE antibodies to seasonal
avoidance and options for pharmacotherapy or allergen
inhalants vary with the seasons, and there is little utility
immunotherapy require objective confirmation of imme-
in performing tests for IgE antibodies to pollen inhalants
diate hypersensitivity and may require referral to an al-
when the allergens are not present in the environment,
lergy specialist. The widespread use of IgE antibody tests
since the results may be falsely negative. The multialler-
in this way by primary care physicians is relatively new.
gen IgE antibody test is an efficient way to screen for the
Accordingly, there is a role for pathologists as consultants
presence of IgE antibodies to pollen allergens. This test
to nonallergist physicians. Pathologists are a resource to
makes use of allergen reagents that have more than 1 al-
clinicians who need information about efficacious ap-
lergen coupled to the surface of the same solid phase. For
proaches to testing and access to modern quantitative test
example, as many as 5 or 6 different pollen allergens of a
particular type, such as grass pollens, can be coupled with
References
the same solid-phase reagent. A positive result indicates
1. Wide L, Bennich H, Johansson SGO. Diagnosis of allergy by an in vitro test
the presence of IgE antibodies to at least 1 of the allergens
for allergen antibodies. Lancet. 1967;2:1105–1107.
2. Sly RM. Changing prevalence of allergic rhinitis and asthma. Ann Allergy
on the solid phase, but is not specific for a particular al-
lergen. As such, a positive result is useful in identifying
3. Downs SH, Marks GB, Sporik R, Belosuova EG, Car NG, Peat JK. Continued
patients who might benefit from further testing with in-
increase in the prevalence of asthma and atopy. Arch Dis Child. 2001;84:20–23.
4. Host A, Andrae S, Charkin S, et al. Allergy testing in children: why, who,
dividual allergen reagents. This is particularly true if re-
when and how? Eur J Allergy Clin Immunol. 2003;58:1–11.
ferral to an allergy specialist is likely, since further testing
5. Weiss KB, Sullivan SD. The health economics of asthma and rhinitis, I: as-
will be needed to identify individual allergens for inclu-
sessing the economic impact. J Allergy Clin Immunol. 2001;107:3–8.
6. Wahn U. What drives the allergic march? Allergy. 2000;55:591–599.
sion in an allergen immunotherapy regimen. A final ad-
7. Wahn U. Allergic factors associated with the development of asthma and
vantage of the multiallergen test is the availability of com-
the influence of cetirizine in a double-blind, randomised, placebo-controlled trial:
mercial test reagents consisting of inhalant allergens
first results of ETACா. Pediatr Allergy Immunol. 1998;9:116–124.
8. Platts-Mills TAE. Allergen avoidance in the treatment of asthma and rhinitis.
found in different geographic regions (northern grass pol-
lens, southern weed pollens, etc). These reagents facilitate
9. Nickel R, Kulig M, Forster J, et al. Sensitization to hen’s egg at the age of
the appropriate selection of tests for pollen inhalant sen-
twelve months is predictive for allergic sensitization to common indoor and out-door allergens at the age of three years. J Allergy Clin Immunol. 1997;99:613–
sitivity by nonallergist physicians.
10. Sampson HA. Utility of food-specific IgE concentrations in predicting
CONCLUSIONS
symptomatic food allergy. J Allergy Clin Immunol. 2001;107:891–896.
11. Sampson HA, Ho DG. Relationship between food-specific IgE concentra-
This review has focused on the use of small groups of
tions and the risk of positive food challenges in children and adolescents. J AllergyClin Immunol. 1997;100:444–451.
tests for IgE antibodies to common allergens to establish
12. Yunginger JW, Ahlstedt S, Eggleston P, et al. Quantitive IgE antibody assays
the presumptive diagnosis of allergic disease in children
in allergic diseases. J Allergy Clin Immunol. 2000;105(6, pt 1):1077–1084.
presenting with signs and symptoms compatible with al-
13. Ownby DR, Anderson JA, Jacob GL, Homburger HA. Development and
comparative evaluation of a multiple-antigen RAST as a screening test for inhalant
lergy (Table). The rationale for this approach is the finding
allergy. J Allergy Clin Immunol. 1984;73:466–472.
Arch Pathol Lab Med—Vol 128, September 2004
Diagnosing Allergic Diseases in Children—Homburger 1031
Vitamin D RevisitedPosted November 20th, 2012 by Dan | http://www.dansplan.com/blog/Getting vitamin D the natural wayToday we feature a new article from, JD Moyer of the blog Systems for Living Well:Recently a few articles and studies have come to my attention that have expanded my understanding of vitamin D metabolism, and raised a few questions as well. As previous posts on this blog have advoc
(Aspetti fisiologici, monitoraggio, diagnosi e patologie della Medico Veterinario Libero Professionista Specialista in Malattie dei Piccoli Animali Past-President SIRVAC (Società It. di Riproduzione Veterinari Animali da Compagnia) Ambulatorio Veterinario Majolino – Ranieri, Vicolo Del Forno 5, 43044 Collecchio (Pr) Fisiologia della Gravidanza In seguito all’ ovulazione e alla formazione
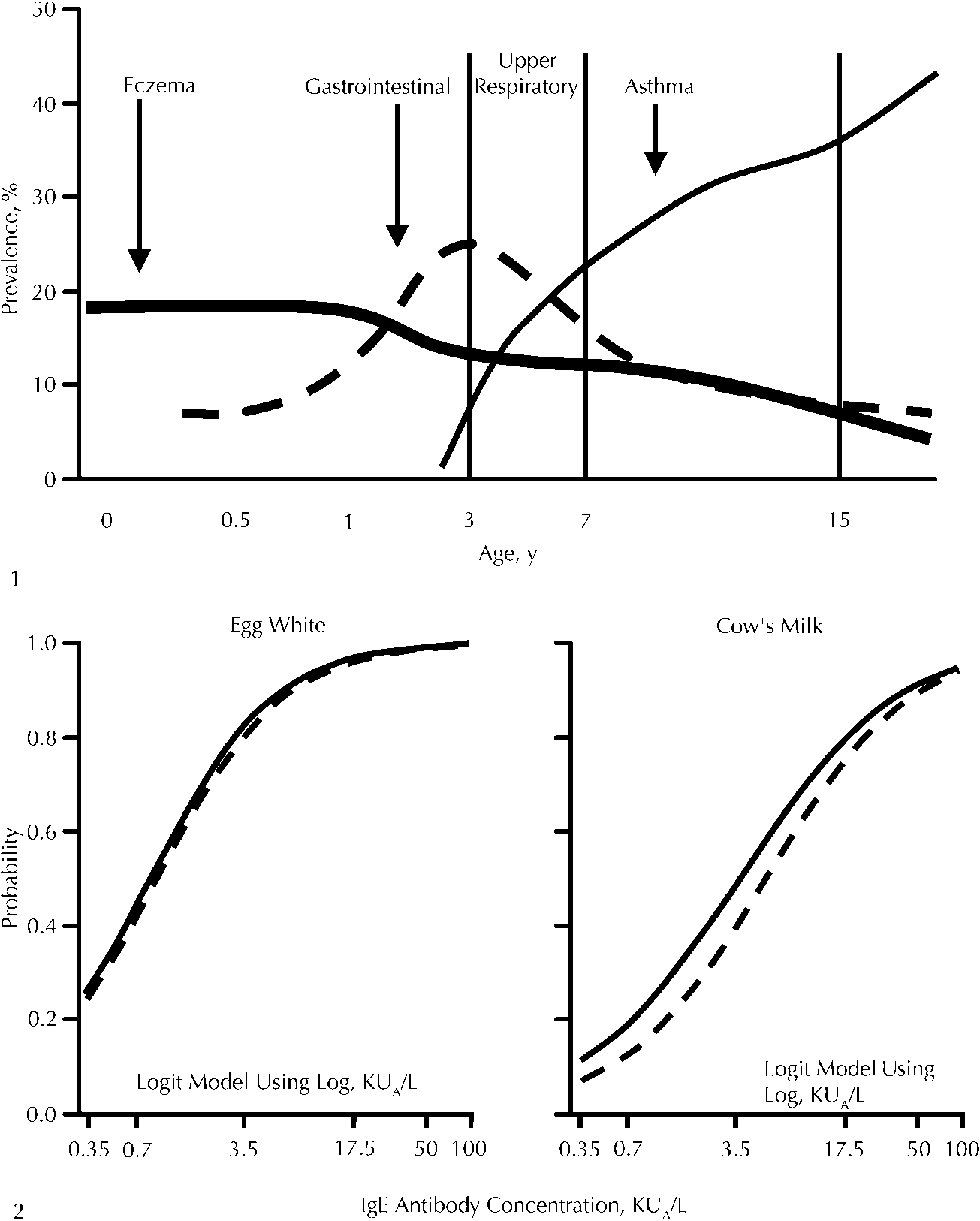 Figure 1. Relationship of age and manifes-
Figure 1. Relationship of age and manifes-