H e a rt-rate turbulence after ventricular premature beats as a predictor of mortality after acute myocardial infarction Georg Schmidt, Marek Malik, Petra Barthel, Raphael Schneider, Kurt Ulm, Linda Rolnitzky, A John Camm,J Thomas Bigger Jr, Albert Schömig
after ventricular premature beats is a very potent
postinfarction risk stratifier that is independent of other
B a c k g r o u n d Identification of high-risk patients after acute
known risk factors and which is stronger than other
presently available risk predictors.
prophylactic therapy. The predictive accuracy of currently
L a n c e t 1999; 3 5 3 : 1 3 9 0 – 9 6
used risk predictors is modest even when several factors
are combined. Thus, establishment of a new powerful
method for risk prediction independent of the available
stratifiers is of considerable practical value.
I n t r o d u c t i o nClinical trials1 , 2 suggest that in high-risk patients with
The study investigated fluctuations of sinus-
ischaemic heart disease, mortality can be effectively
rhythm cycle length after a single ventricular premature beat
reduced by implantation of a cardioverter-defibrillator.
recorded in Holter electrocardiograms, and characterised
Since the selection of high-risk patients is a crucial part
the fluctuations (termed heart-rate turbulence) by two
of prophylaxis, risk stratification strategies are important.
numerical parameters, termed turbulence onset and slope.
In patients surviving acute myocardial infarction, the
The method was developed on a population of 100 patients
predictive value of currently used risk factors, such as
with coronary heart disease and blindly applied to the
population of the Multicentre Post-Infarction Program (MPIP;
577 survivors of acute infarction, 75 deaths during a
median follow-up of 22 months) and to the placebo
v a r i a b i l i t y ,8 and mean heart rate9 is modest1 0 even when
population of the European Myocardial Amiodarone Trial
several predictors are combined and methodological
(EMIAT; 614 survivors of acute myocardial infarction, 87
issues of such a combination solved.1 1 Establishment of a
deaths during median follow-up of 21 months). Multivariate
new risk predictor independent of the presently availablestratifiers is therefore of considerable practical value.
risk stratification was done with the new parameters and
We describe a new method for risk stratification based
on a simple expression of ventriculophasic sinus
F i n d i n g s One of the new parameters (turbulence slope) was
a r r h y t h m i a ,1 2 – 1 4 namely fluctuations of sinus-rhythm cycle
the most powerful stratifier of follow-up mortality in EMIAT
length after a single VPB. We term such fluctuations
and the second most powerful stratifier in MPIP: MPIP risk
heart-rate turbulence. In low-risk patients, we observed
ratio 3·5 (95% CI 2·2–5·5, p<0·0001), EMIAT risk ratio 2·7
that after a VPB, sinus shythm shows a characteristic
(1·8–4·2, p<0·0001). In the multivariate analysis, low left-
ventricular ejection fraction and turbulence slope were the
deceleration. Such a characteristic pattern does not
only independent variables for mortality prediction in MPIP
occur in high-risk patients. We propose to characterise
(p<0·001), whereas in EMIAT, five variables were
this phenomenon by two descriptors, both of which
independent mortality predictors: abnormal turbulence
contain independent information on the risk ofsubsequent mortality.
onset, abnormal turbulence slope, history of previous
The new risk predictors were developed in an open
infarction, low left-ventricular ejection fraction, and high
study with a training sample of 100 patients accumulated
mean heart rate (p<0·001). In both MPIP and EMIAT, the
at the medical department of the Technical University in
combination of abnormal onset and slope was the most
Munich and validated blind, in both univariate and
powerful multivariate risk stratifier: MPIP risk ratio 3·2
(1·7–6·0, p<0·0001), EMIAT risk ratio 3·2 (1·8–5·6,
populations of myocardial-infarction survivors, namely the
population of the Multicentre Post-Infarction Program
I n t e r p r e t a t i o n
(MPIP) study4 and in the placebo group of the EuropeanMyocardial Infarction Amiodarone Trial (EMIAT).1 5
Erste Medizinische Klinik (G Schmidt MD, P Barthel MD, R Schneider MEng, A Schömig MD); and Institut für Medizinische Statistik und Epidemiologie, Technischen Universität München, München, Germany (K Ulm PhD); Department of Cardiological
100 patients with coronary artery disease (78 of whom had a
Sciences, St George’s Hospital Medical School, London, UK
history of myocardial infarction and 26 a history of multiple
(M Malik PhD, A J Camm MD); and Division of Cardiology, Department
infarctions) and presenting with sinus rhythm and more than
of Medicine, Columbia University, NY, New York, USA (L Rolnitzky
ten VPBs per hour during 24 h Holter monitoring were used to
design the method and to optimise the risk prediction power of
Correspondence to: Dr Georg Schmidt, Erste Medizinische Klinik der
the new indices. Characteristics of these patients have
Technischen Universität München, Ismaniger Strae 22, 81675
previously been published1 6 and are listed in table 1. During a 2-
year follow-up period, 17 of these patients died.
(e-mail: [email protected])
In each patient, a 24 h Holter recording was obtained
THE LANCET • Vol 353 • April 24, 1999
Training sample MPIP population EMIAT population
Data are mean (SD) or number (%) of patients.
Table 1: Patients’ characteristics
d u r i n g a stable phase of coronary artery disease (at least 3months after acute myocardial infarction). An Oxford ExcelHolter system (Oxford Instruments, Abingdon, UK) was usedto process the Holter recordings. After manual review andrevision, computer files were generated containing the durationof individual RR intervals and morphology classifications ofindividual QRS complexes (normal, supraventricular, andventricular
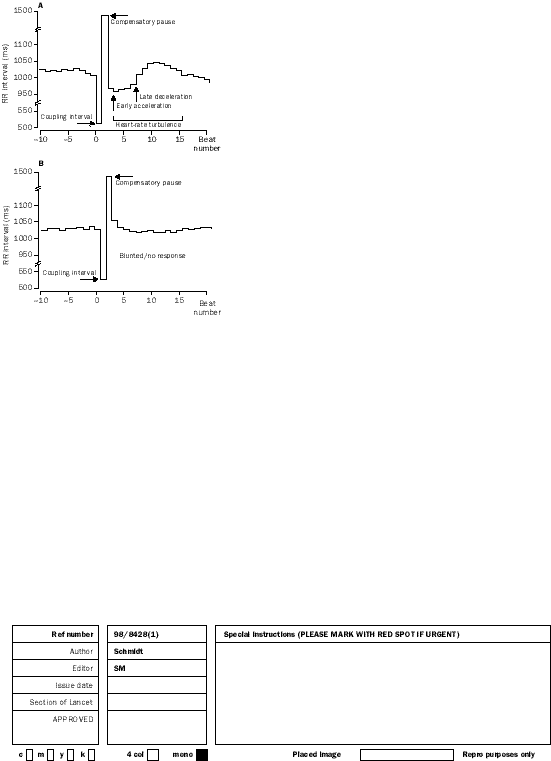
In patients surviving follow-up, we observed a typical pattern
of sinus-rhythm RR interval series following singular VPBs. TheVPBs were followed by an early acceleration and a latedeceleration of the sinus rhythm. Figure 1 A gives a typicalexample of this pattern in a long-term survivor. Theacceleration starts immediately after an ectopic beat and lastsfor only a few RR intervals. Subsequent decleration reaches amaximum between the third and seventh sinus cycle; the longestRR interval occurs usually near to the tenth cycle after a VPB. These variations are subtle and can be recognised only aftercomputer algorithm.
In patients who died during the follow-up period, the extent
of this turbulence response to VPBs was substantially smaller
Figure 1: Examples of heart-rate turbulence patterns in two patients from training sample
Numerical descriptors were investigated characterising both
A: Typical acceleration-deceleration sequence of RR intervals after
phases of the heart-rate turbulence (that is initial acceleration
coupling interval and compensatory pause of a VPB recorded in a 64-
and subsequent deceleration) with the aim of obtaining
year-old woman with anterior myocardial infarction who survived duringfollow-up. B: Almost random pattern recorded in a 77-year-old man with
descriptors that were independent each of the other, separated
inferior myocardial infarction who suddenly died 7 months after the index
patients who did and did not die during follow-up, and were
predictors of mortality independent of age, left-ventricular
group. The patients were survivors of a recent myocardial
ejection fraction (LVEF), and other Holter-based risk factors.
infarction with LVEF of 40% or less, aged 75 years or younger,
The numerical factors characterising the chronotropic
free of bradyarrhythmia, and free of contraindications to
response to VPBs were dichotomised into normal and abnormal
amiodarone therapy. Of these, 129 patients were excluded from
values. Cut-off points for the dichotomisation were determined
our analyses because of atrial fibrillation, no VPB during Holter
by the method of maximising the log-rank test statistic for all
monitoring, or because the Holter tape was not available. The
possible cut-off values within the 10–90 percentiles of each
remaining 614 patients were studied (table 1). During median
predictor. The approach is identical to recursive partitioning or
follow-up of 21 months, 87 patients died.
the use of classification and regression trials as introduced by
In the MPIP population, Holter recordings were done in the
Breiman and colleagues1 7 and adapted to use for survival data
second week after the index infarction; in the EMIAT
by LeBlanc and Crowley1 8 in the context of Cox’s proportional-
population, the recordings were obtained in the second or third
week after the infarction. Initially, the Holter tapes were
In each patient, LVEF was assessed either by radionuclide or
processed at Columbia University, New York (MPIP data) and
by EMIAT investigators. In both populations, a Laser Holter
respectively). Other recognised risk factors were obtained from
8000 System (Marquette Medical System, WI, USA) was used
the Holter recordings and included mean heart rate, frequency
to obtain, after visual inspection and manual editing, computer
of ventricular ectopathy, and 24 h heart-rate variability (HRV).
files listing RR interval duration (sampling frequency 128 Hz)
HRV was expressed by the so-called HRV triangular index, an
and QRS morphological classifications on a beat-to-beat basis.
established measure of global 24 h HRV that is, compared with
The RR interval and beat-type files of individual MPIP and
other measures, relatively insensitive to the precision with which
EMIAT Holter recordings were transferred to the Technical
University of Munich for the computation of characteristics ofheart-rate turbulence. The same dichotomies as derived from
the training samples were applied without knowledge of
The MPIP study4 enrolled 715 survivors of acute myocardial
patients’ characteristics and the results provided to the
infarction (age р70 years). Of these, 138 patients were excluded
collaborating centres (Columbia University, New York, for the
from the analysis of the heart-rate turbulence after VPBs
MPIP data, and St George’s Hospital Medical School, London,
because of atrial fibrillation, no VPB during Holter monitoring,
for the EMIAT data) who did the survival analyses.
missing LVEF, or because of technically insufficient or missing
To eliminate any possible bias, the centre in Munich has
Holter recordings. The remaining 577 patients were used in this
never received individual clinical data (clinical variables and
study (table 1). The patients were followed up for a median of
mortality) of the MPIP and EMIAT populations and the
22 months. During this period, 75 of the patients died.
collaborating centres were not aware of the principle of the
The EMIAT trial1 5 randomised 743 patients into the placebo
analysis and measurement involved until the statistical analyses
THE LANCET • Vol 353 • April 24, 1999
Variable Training sample MPIP population EMIAT population
*Due to inclusion criteria, arrhythmia on Holter was present in every patient of the training sample.
Table 2: Statistical association of risk variables with mortality
intervals immediately after compared with immediately
In both MPIP and EMIAT populations, LVEF was assessed
before a VPB and is termed here the turbulence onset.
by radionuclide ventriculography,4 , 1 5 mean heart rate was taken
The speed of the subsequent deceleration was quantified
as the mean of all sinus rhythm cycles in the Holter recordings,
by the steepest regression line between the RR interval
and HRV triangular index expressing the global 24 h HRV was
count and duration. The corresponding factor is termed
calculated from the Holter recording by previously described
here the turbulence slope. In precise numerical terms, we
For the purpose of multivariate analysis, age (dichtomised at
<65 years v s 65 years), history of previous myocardial
Turbulence onset is defined as the difference between
infarction, LVEF (dichtomised at 30% v s <30%), arrhythmia
the mean of the first two sinus RR intervals after a VPB
sign on Holter (defined as ten or more VPBs per h or at least
and the last two sinus RR intervals before the VPB
one non-sustained ventricular tachycardia of three or more
divided by the mean of the last two sinus RR intervals
beats on the Holter recording), mean heart rate (dichotomised
at >75 beats per min v s 75 beats per min), and HRV (HRVtriangular index dichotomised at >20 v s 20 units) were also
assessed. Their cut-off points were based on previous risk
stratification investigations.4 , 9 , 1 5 , 2 0
where RR is the i-th sinus rhythm after (i>0) the
compensatory pause of the VPB or preceding (i<0) the
The endpoint of the study was total mortality. Continuous and
coupling interval of the VPB. For convenience, the value
categorical variables were compared by the Kruskal-Wallis test
of turbulence onset is expressed as a percentage. For
and the 2 test, respectively. Kaplan-Meier survival functions
instance, in figure 1A, the coupling interval of the
were calculated to test the association of heart-rate turbulence
ectopic is preceded by RR intervals of 1017 ms and 1014
characteristics with total mortality. The main survival analyseswere done with the Cox proportional-hazards model with a
ms and its compensatory pause is followed by RR
intervals of 974 ms and 963 ms. Thus, in this case,
In MPIP and EMIAT datasets, sensitivity, specificity, and
positive and negative predictive accuracy of follow-up mortality
prediction were also evaluated for conventional and heart-rate-
turbulence-based predictors of mortality (with dichotomies asa b o v e ) .
Results of all survival analyses are presented as relative risks
These measurements were first performed for each
with corresponding 95% CI. A significance level of 0·05 was
individual singular VPB and then averaged to obtain the
value characterising the patient. Positive values ofturbulence onset mean sinus rhythm deceleration after a
VPB, and negative turbulence onset means sinus rhythm
Of the number of possibilities tested, two factors were
Turbulence slope is defined as the maximum positive
selected to characterise the chronotropic response of
slope of a regression line assessed over any sequence of
five subsequent sinus-rhythm RR intervals within the
acceleration was quantified by the relative change of RR
first 20 sinus-rhythm intervals after a VPB. The value of
Training sample MPIP population AMIAT population Variable Age >65 years Combined turbulence onset 7·4 (3·1–17·3) <0·0001 and slope*
MI=myocardial infarction. *Turbulence onset у0 and turbulence slope р2·5 per RR interval; Sen=sensitivity, Spc=specificity, Ppa=positive predictive accuracy, Npa=negative predictiveaccuracy (%).
Table 3: Association of risk variables with total mortality in a univariate analysis
THE LANCET • Vol 353 • April 24, 1999
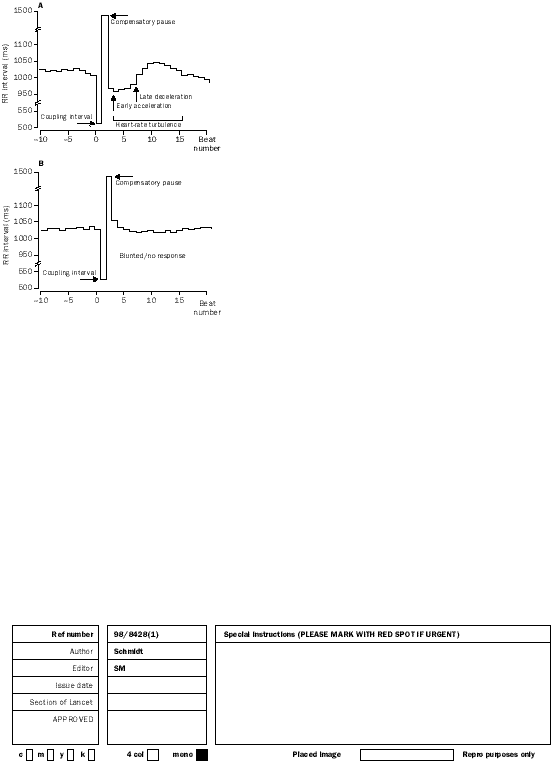
Figure 2: Kaplan-Meier survival curves in MPIP and EMIAT patients stratified to those with turbulence onset <0 and
0 (A, B) and stratified to those with turbulence slope >2·5 and 2·5 per RR interval (C, D) The numbers of patients of the individual groups involved in the analysis at 0, 6, 12, 18, and 24 months are shown under each graph: the top and bottom row corresponds to the upper and bottom survival curve, respectively.
turbulence slope is expressed in ms per RR interval and
second strongest univariate mortality predictor after low
for each recording, it was obtained from the tachogram
LVEF (table 3). Simultaneous use of turbulence onset
R R , RR , RR . . . , R R , where RR is the average of i- t h
and slope provided highest relative risks in both the
sinus-rhythm RR interval after the compensatory pause
MPIP population (5·0 [95% CI 2·8–8·8]) and the
of a singular VPB. The log-rank test statistics for all
EMIAT population (4·4 [2·6–7·5], table 3).
possible cut-off points revealed optimal dichotomies of 0
Figure 2 shows Kaplan-Meier cumulative survival
for turbulence onset and 2·5 ms per RR interval for
curves for turbulence onset and slope in MPIP and
turbulence slope. In the training sample, there were
EMIAT patients. In the MPIP patients, those with
significant associations of turbulence onset and slope
turbulence onset of less than zero had a 2-year mortality
of 11% versus 20% in patients with turbulence onset ofzero or higher. In the EMIAT patients, the mortality
rates were 11% and 24%, respectively. In the MPIP
In univariate analyses of both MPIP and EMIAT
patients, those with turbulence slope greater than 2·5 ms
populations, we noted a strong and significant
had a 2-year mortality of 9% versus 27% in patients
association of turbulence onset and slope with total
w i t h turbulence slope of 2·5 ms or less. In the EMIAT,
mortality both when used as continuous variables and
these mortalities were 9% and 26%, respectively.
when dichotomised at the predefined cut-off points. In
T h e differences in cumulative survival were highly
MPIP data, the LVEF, HRV triangular index, and
turbulence slope provided the most significant difference
Figure 3 shows Kaplan-Meier cumulative survival
between numerical values in survivors and non-survivors;
curves for the combinations of turbulence onset and
in EMIAT data, the differences in numerical values of
slope in MPIP and EMIAT. In the MPIP population,
turbulence slope were most significant (table 2). In
the 2-year mortality rates were 9%, 15%, and 32% in
EMIAT, the turbulence slope was the strongest
patients with both factors normal, patients with either
univariate mortality predictor; in MPIP, it was the
factor abnormal, and patients with both factors
THE LANCET • Vol 353 • April 24, 1999
Figure 3: Kaplan-Meier survival curves in MPIP and EMIAT patients stratified to three groups Turbulence onset <0 and turbulence slope >2·5 ms/RR interval (both factors normal); either turbulence onset 0 or turbulence slope 2·5 ms/RR interval (one of the factors abnormal); turbulence onset 0% and turbulence slope 2·5 ms/RR interval (both factors abnormal). The numbers of patients of the individual groups involved in the analysis at 0, 6, 12, 18, and 24 months are shown under each graph: the order of the rows corresponds to the order of the survival curves.
abnormal, respectively. In EMIAT, these figures were
p<0·0001, respectively). The relative hazard for LVEF
9%, 18%, and 34%, respectively. Again, the differences
(30% v s <30%) was 2·9; the relative hazard of the
in cumulative survival were highly significant.
turbulence onset/slope combination (slope >2·5 and
In both MPIP and EMIAT, the combination of
onset <0% v s slope 2·5 and onset 0) was 3·2. In
turbulence onset greater than zero and turbulence slope
EMIAT, four variables were independent predictors: the
o f 2·5 ms per RR interval or less yielded a positive
strongest predictor was the combination of turbulence
predictive accuracy (33% and 31%, respectively), that
onset and slope with a relative hazard of 3·2, while the
was higher than the positive predictive accuracy of any
other significant predictors were history of previous
conventional predictor while maintaining the same level
myocardial infarction, LVEF, and mean heart rate with
relative hazards between 1·7 and 1·8. Patients with
abnormal turbulence onset and abnormal turbulence
Table 4 presents the results of the stepwise,
slope are not infrequent; in the MPIP and EMIAT
multivariate, Cox regression analysis with turbulence
population, there were 70 (12·1%) and 80 (13·0%) such
onset and slope as separate variables. In the MPIP
population, LVEF and turbulence slope were the onlyindependent variables (p<0·001) and their relative
hazards were almost identical (3·0 and 2·5). In EMIAT,
The results of this study clearly show that heart-rate
five variables were independent predictors of mortality,
namely turbulence onset and slope, history of previous
deceleration of sinus rhythm after a singular VPB) is a
myocardial infarction, LVEF, and mean heart rate.
consistent phenomenon in low-risk patients with
Table 5 presents the results of the stepwise,
multivariate, Cox-regression analysis on a combination
phenomenon indicates a significantly increased risk of
of turbulence onset and slope. In both MPIP and
subsequent mortality. The two measures for quantifying
EMIAT populations, the combination of abnormal
heart-rate turbulence were developed in one population
turbulence onset (0) and an abnormal turbulence slope
(2·5 ms per RR interval) was the strongest mortality
prospectively tested with masking in two large and
predictor. In the MPIP population, LVEF and the
combination of turbulence onset and slope were the only
postinfarction trials MPIP and EMIAT. Therefore, we
believe that our analysis proves the clinical relevance of
MPIP population EMIAT population MPIP population EMIAT population
Table 5: Relative hazards of individual variables in a
Table 4: Relative hazards of significant and independent risk multivariate analysis involving combination of turbulence onset variables in a multivariate analysis and slope
THE LANCET • Vol 353 • April 24, 1999
the new phenomenon. Because of the treatment practice
manifestation of this protection may be captured when
changes, more patients in EMIAT than in MPIP
responding to a potentially proarrhythmic VPB. If the
received thrombolysis -blockers, and inhibitors of
erratic or absent response to VPBs in patients with high
values of turbulence onset and low values of turbulence
differences show that our finding is independent of
slope is a manifestation of lost antiarrhythmic protection,
modern management of postinfarction patients. The
the chronotropic response to VPBs might be the
MPIP population was also an unselected population of
mechanistic link between impaired autonomic balance
postinfarction patients, whereas only patients with low
LVEF were enrolled in the EMIAT trial. Consequently,
The limitations of our approach have to be recognised.
the numbers of VPBs differed in these populations, but
We have merely taken measures averaged over 24 h and
not investigated the spontaneous variability of the
Turbulence onset and slope are both predictors of
chronotropic response. We have not made any detailed
mortality containing information additional to each other
distinction between VPBs with and without retrograde
and to other established risk factors. The combination of
conduction but, judging from the compensatory pauses
turbulence onset and slope was a very strong risk
with both present and absent heart-rate turbulence
predictor in patients of the MPIP trial and of the placebo
(figure 1), the phenomenon we describe is unlikely to be
group of EMIAT, even when adjusted for other
related solely to such a distinction. We have not
established mortality predictors, such as LVEF,
investigated the effect of therapy on heart-rate
arrhythmia count, heart-rate variability, mean heart rate,
turbulence, especially the effects of thrombolytic
therapy, -blockade, an ACE inhibition, which are
Turbulence onset and slope in combination was by far
currently frequent in patients surviving acute myocardial
the strongest Holter-based risk predictor.
infarction. However, the observations made in the data
It has long been known that a ventricular systole can
of the MPIP study in which these therapeutic
influence the rate of sinus nodal discharge, even in the
absence of retrograde atrioventricular conduction. As
observations are not merely a by-product of modern
early as 1909, first observations of the so-called
therapeutic interventions. Our method is clearly
ventriculophasic sinus arrhythmia were made in
inapplicable to patients without any VPBs but, as such
experimental atrioventricular block.2 1 The first clinical
patients are generally at low risk, this limitation is of no
description was made in 1914 by Hecht,2 2 who observed
practical consequence. We also do not know whether the
ventriculophasic sinus arrhythmia in a child with Adams-
response to several VPBs needs to be averaged, as was
Stokes syndrome. Later on, ventriculophasic arrhythmia
the case in this study, to obtain a sensible measure of
was observed in patients with ventricular-inhibited
heart-rate turbulence. Although the averaging process in
p a c i n g .2 3 To our knowledge, however, only one case
recordings with multiple VPBs helps to overcome the
report exists on ventriculophasic sinus arrhythmia
difficulties with precision of RR-interval measurement,
the assessment of turbulence onset and slope depends on
Various pathophysiological mechanisms have been
the sampling frequency of long-term ECGs. Still, our
discussed to explain the ventriculophasic mechanisms,
results show that even the contemporary precision of
including changes in autonomic tone,1 2 – 1 4 , 2 5 , 2 6 traction on
Holter reading is sufficient for assessment of turbulence
the atrium as well as atrial appendages, atrioventricular
onset and slope, possibly because the precision issue
junction, and the sinus nodal region,1 2 , 2 3 , 2 7 , 2 8 and transient
concerns mainly patients with very few VPBs who are
improvement of the blood supply to the sinus node.1 2 , 2 9 , 3 0
Some authors even speculated that the character of
Despite the limitations of our approach, the masked
ventriculophasic phenomena will eventually gain an
tests of this study prove clearly that the absence of the
characteristic heart-rate patterns after VPBs is a very
Although it is plausible to expect the cardiac
potent postinfarction risk stratifier that is independent of
autonomic status to influence heart-rate turbulence, it is
other known risk factors and is stronger than other
also plausible to expect the physiological background of
the turbulence to be different from that of heart-rate
variability, which reflects, partly, the modulations of the
G Schmidt did the conceptual design of heart-rate turbulence, designed
cardiac autonomic status. Long-term, such as 24 h,
the investigations of this study, supervised the testing sample and data
heart-rate variability probably mostly reflects autonomic
analyses. M Malik designed the investigations of this study, hadresponsibility for the evaluation of the EMIAT data, data exchange
responses to environmental and external stimuli that
between the centres, and supervision of the text of the manuscript.
activate a broad variety of physiological reflexes. By
P Barthel and R Schneider did the computer implementation and
contrast heart-rate turbulence is a phenomenon triggered
maintenance of the heart-rate technology. K Ulm did statistical analyses. L Rolnitzky and J T Bigger had responsibility for the MPIP trial data and
by a minimum endogenous stimulus to which the reflex
their evaluations. A J Camm had responsibility for the EMIAT data.
responses are possibly more organised and systematic.
A Schomig supervised the study overall.
This might also be the explanation why the risk-
predictive power of heart-rate turbulence appears to be
This study was supported in part by grants from the Bundesministerium
superior to that of heart-rate variability.
für Bildung, Wissenschaft, Forschung und Technologie (13N7073/7, to
The mechanisms linking the absence of heart-rate
G Schmidt), and the Bund der Freunde der Technischen UniversitätMünchen (to G Schmidt).
turbulence to mortality are not obvious. Probably, theturbulence onset and slope assessment reflects specificaspects of cardiac autonomic status. The preserved vagal
R e f e r e n c e s
tone is known to be antiarrhythmic3 1 , 3 2 and probably
Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with animplanted defibrillator in patients with coronary disease at high risk
constitutes autonomic antiarrhythmic protection. Thus,
for ventricular arrhythmia: Multicenter Automatic Defibrillator
by measurement of the heart-rate turbulence, a direct
Implantation Trial Investigators. N Engl J Med 1996; 3 3 5 : 1 9 3 3 – 4 0 .
THE LANCET • Vol 353 • April 24, 1999
Guidelines for risk stratification after myocardial infarction. A n n
premature complexes and mortality risk. Pacing Clin ElectrophysiolIntern Med 1997; 1 2 6 : 5 5 6 – 6 0 .
1996; 1 9 : 9 7 6 – 8 0 .
Sanz G, Castaner A, Betriu A, et al. Determinants of prognosis in
1 7 Breimann L, Friedman JH, Ohlsen RA, Stone CJ. Classification and
survivors of myocardial infarction: a prospective clinical angiographic
regression trees (CART). Belmont, CA: Wadsworth International
study. N Engl J Med 1982; 3 0 6 : 1 0 6 5 – 7 0 .
Multicenter Postinfarctions Research Group. Risk stratification and
1 8 LeBlanc M, Crowley J. Relative risk trees for censored survival data.
survival after myocardial infarction. N Engl J Med 1983; 3 0 9 : B i o m e t r i c s 1993; 4 8 : 4 1 1 – 2 5 .
1 9 Cox DR. Regression models and life-tables. J R Stat Soc 1972; 3 4 :
Bigger JJ, Fleiss JL, Kleiger R, Miller JP, Rolnitzky LM. The
relationships among ventricular arrhythmias, left ventricular
2 0 Task Force of the European Society of Cardiology and the American
dysfunction, and mortality in the 2 years after myocardial infarction.
Society of Pacing and Electrophysiology. Heart rate variability:
C i r c u l a t i o n 1984; 6 9 : 2 5 0 – 5 8 .
Standards of measurement, physiological interpretation, and clinical
Moss AJ, DeCamilla JJ, Davis HP, Bayer L. Clinical significance of
use. C i r c u l a t i o n 1996; 9 3 : 1 0 4 3 – 6 5 .
ventricular extopic beats in the early posthospital phase of myocardial
2 1 Erlanger J, Blackman JR. Further studies in the physiology of heart
infarction. Am J Cardiol 1977; 3 9 : 6 3 5 – 4 0 .
block in mammals: chronic auriculo-ventricular heart-block in the
Simson MB. Use of signals in the terminal QRS complex to identify
dog. H e a r t 1909; 1 : 1 7 7 .
patients with ventricular tachycardia after myocardial infarction.
2 2 Hecht AF. Das Morgani-Adams-Stokes Syndrome im Kindesalter
C i r c u l a t i o n 1981; 6 4 : 2 3 5 – 4 2 .
und seine Behandlung. Wien med Wch schr 1914; 6 4 : 1 7 8 .
Kleiger RE, Miller JP, Bigger JJ, Moss AJ. Decreased heart rate
2 3 Chung EK, Jewson DV. Ventriculophasic sinus arrhythmia in the
variability and its association with increase mortality after acute
presence of artificial pacemaker induced ventricular rhythm.
myocardial infarction. Am J Cardiol 1987; 5 9 : 2 5 6 – 6 2 . C a r d i o l o g y 1970; 5 5 : 6 5 – 6 8 .
Copie X, Hnatkova K, Staunton A, Fei L, Camm AJ, Malik M.
2 4 Döhlemann C, Murawski P, Theissen K, Haider M, Forster C,
Predictive power of increased heart rate versus depressed left
Poppl SJ. Ventriculophasische Sinusarrhythmie bei ventrikulärer
ventricular ejection fraction and heart rate variability for risk
Extrasystolie. Z Kardiol 1979; 6 8 : 5 5 7 – 6 5 .
stratification after myocardial infarction: results of a two-year follow- up study. J Am Coll Cardiol 1996; 27: 2 7 0 – 7 6 .
2 5 Roth IR, Kirsch B. The mechanism of irregular sinus rhythm in
auriculoventricular heart block. Am Heart J 1948; 3 6 : 2 5 7 – 7 6 .
1 0 Odemuyiwa O, Malik M, Farrell T, Bashir Y, Poloniecki J, Camm J.
Comparison of the predictive characteristics of heart rate variability
2 6 Rosenbaum M, Lepeschkin E. The effect of ventricular systole on
index and left ventricular ejection fraction for all-cause mortality,
auricular rhythm in auriculoventricular block. C i r c u l a t i o n 1955; 1 1 :
arrhythmic events and sudden death after acute myocardial
infarction. Am J Cardiol 1991; 6 8 : 4 3 4 – 3 9 .
2 7 Kappagoda CT, Linden RJ, Saunders DA. The effect on heart rate of
1 1 Redwood SR, Odemuyiwa O, Hnatkova K, et al. Selection of
distending the atrial appendages in the dog. J Physiol Lond 1972; 2 2 5 :
dichotomy limits for multifactorial prediction of arrhythmic events
and mortality in survivors of acute myocardial infarction. Eur Heart J
2 8 Kappagoda CT, Linden RJ, Snow HM. A reflex increase in heart rate
1997; 1 8 : 1 2 7 8 – 8 7 .
from distension of the junction between the superior vena cava and
1 2 Parsonnet AE, Miller R. Heart block. The influence of ventricular
the right atrium. J Physiol Lond 1972; 2 2 0 : 1 7 7 – 9 7 .
systole upon the auricular rhythm in complete and incomplete heart
2 9 Wenckebach KF, Winterberg H. Die unregelmäßige Herztätigkeit.
block. Am Heart J 1944; 27: 6 7 6 – 8 7 .
1 edn. Leipzig: Verlag von Wilhelm Engelmann, 1927.
1 3 Jedlicka J, Martin P. Time course of vagal effects studies in clinical
3 0 Hashimoto K, Tanaka S, Hirata M, Chiba S. Responses of the sino-
electrocardiograms. Eur Heart J 1987; 8 : 7 6 2 – 7 2 .
atrial node to change in pressure in the sinus node artery. Circ Res
1 4 Skanes AC, Tang ASL. Ventriculophasic modulation of
1967; 2 1 : 2 9 7 – 3 0 4 .
atrioventricular nodal conduction in humans. C i r c u l a t i o n 1998; 9 7 :
3 1 Lown B, Verrier RL. Neural activty and ventricular fibrillation. N Engl J Med 1976; 2 9 4 : 1 1 6 5 – 7 0 .
1 5 Julian DG, Camm AJ, Frangin G, et al. Randomised trial of effect of
3 2 Corr PB, Yamada KA, Witkowski FX. Mechanisms controlling
amiodarone on mortality in patients with left-ventricular dysfunction
cardiac autonomic function and their relation to arrhythmogenesis.
after recent myocardial infarction: EMIAT. L a n c e t 1997; 3 4 9 :
In: Fozzard HA, Haber E, Jennings RB, Katz AN, Morgan HE, eds.
The heart and cardiovascular system. New York: Raven Press, 1986:
1 6 Schmidt G, Morfill GE, Barthel P, et al. Variability of ventricular
THE LANCET • Vol 353 • April 24, 1999
Top 10 Human Medications That Poison Our Petshttp://www.aspca.org/pet-care/poison-control/top-10-human-me. Top 10 Human Medications That Poison Our Pets Although pet parents are well aware of poisons lurking around their home,many don’t realize that some of the biggest culprits are sitting right on theirown nightstands. In 2007, the ASPCA Animal Poison Control Center received89,000 call
Available online at www.sciencedirect.comJingping Zhang, Man Ye, Haishan Huang, Lezhi Li, and Aiyun YangOdds of major depression have significantly increased among adults withchronic diseases. However, the diagnosis of depression is often unrecognizedin China.To know the prevalence of depression in medical inpatients with differ-ent chronic diseases and to assess the level of unrecognized depres
 Training sample
Training sample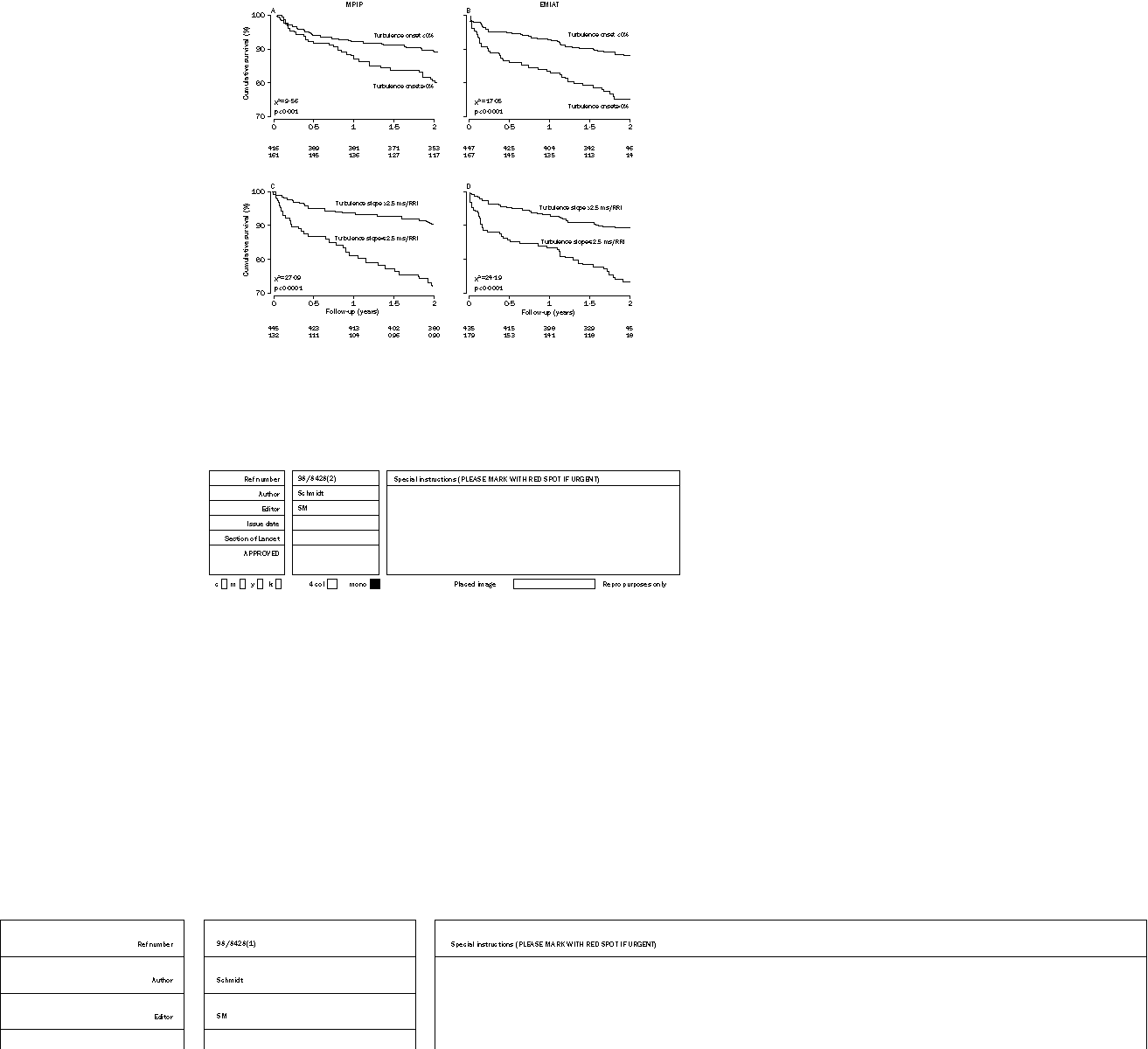
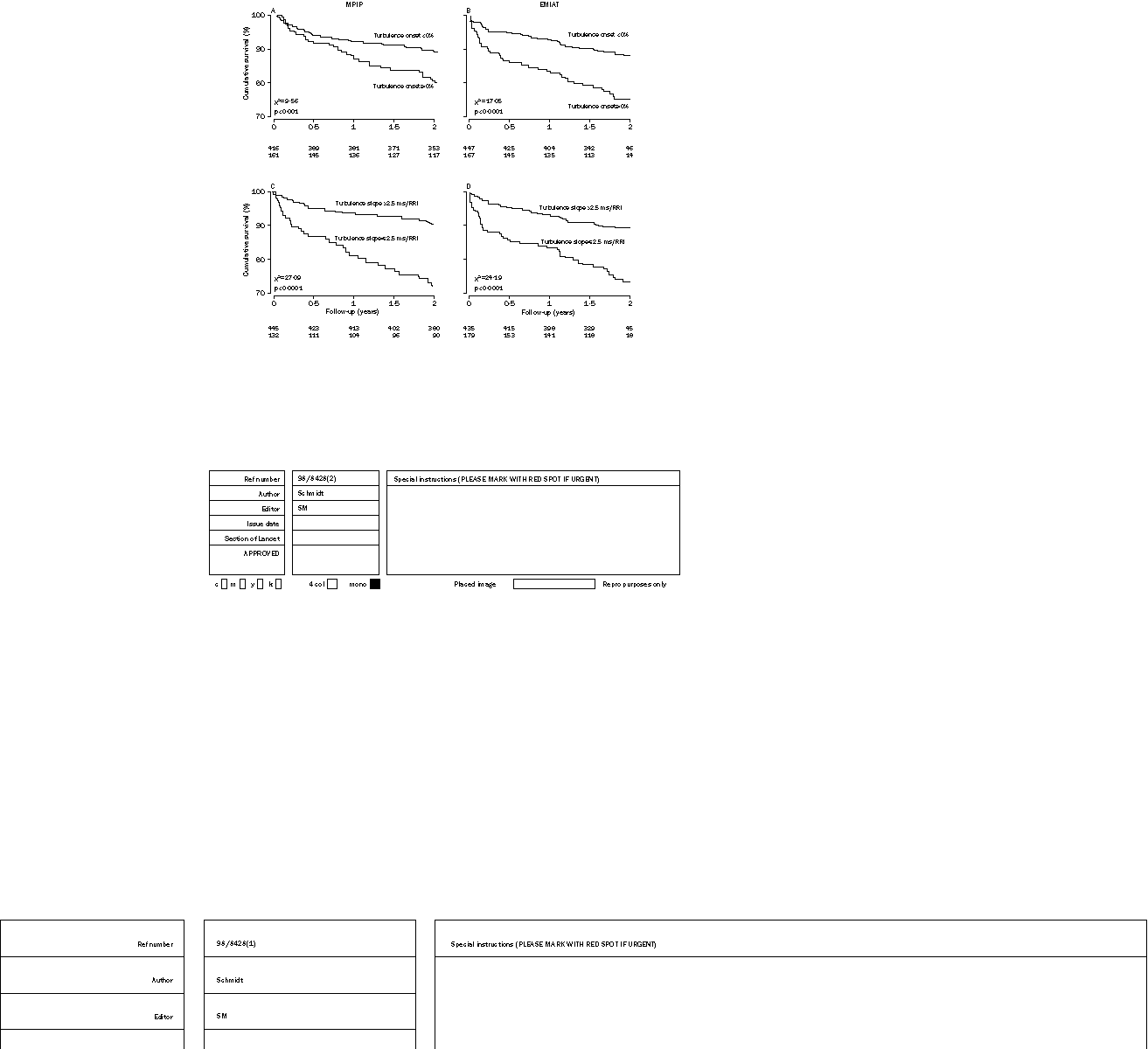 Figure 2: Kaplan-Meier survival curves in MPIP and EMIAT patients stratified to those with turbulence onset <0 and
Figure 2: Kaplan-Meier survival curves in MPIP and EMIAT patients stratified to those with turbulence onset <0 and 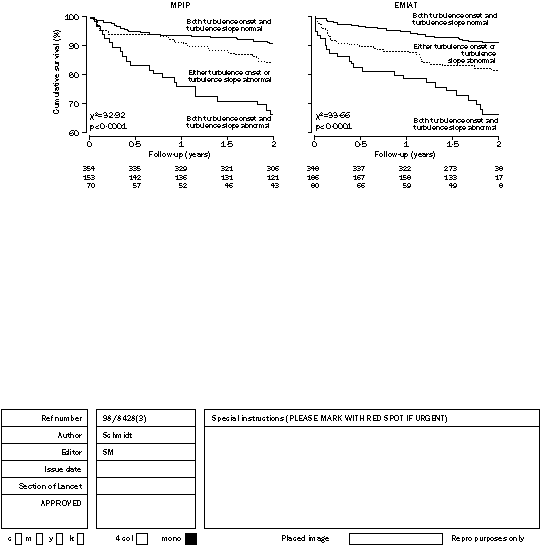
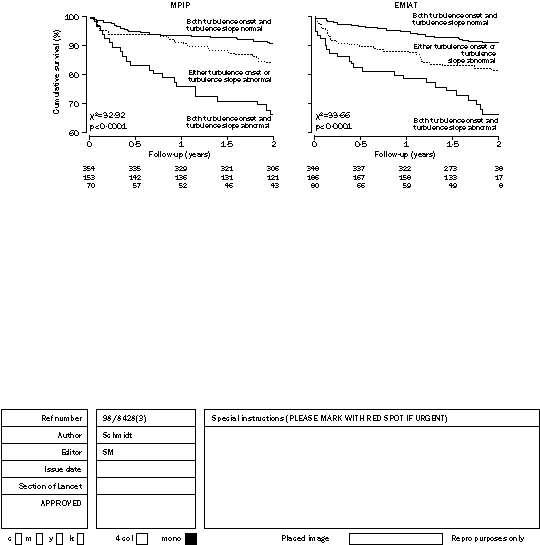 Figure 3: Kaplan-Meier survival curves in MPIP and EMIAT patients stratified to three groups
Figure 3: Kaplan-Meier survival curves in MPIP and EMIAT patients stratified to three groups