Microsoft powerpoint - olt-hiv viral rebound_sf v.8. croi 2010 final
17th CROI 2010, San Francisco, CA - 2010 Background: Discontinuation of HAART in chronic HIV-1 infection is accompanied by a rapid rise in plasma HIV-1 RNA viral load (pVL) and a decrease in CD4+ T-cell counts. However, pVL and immunological dynamics following Poster 687: Short-term plasma HIV-1 RNA viral load
transitory cessation of HAART after OLT in HIV-1–infected patients on immunosuppressive therapy has not been wel characterized. The aim of this study is to describe the short-term (4 weeks) dynamics of pVL and CD4/CD8
and immunological changes following temporary
subset changes after discontinuation of HAART. discontinuation of HAART after liver transplantation Methods: We included 25 consecutive HCV/HIV-coinfected patients who underwent OLT between 2002-2006 and had on HAART a pVL below detection levels (BDL, <50 copies/mL) at OLT, who transiently discontinued cART and (OLT) in HIV-1–infected recipients
restarted it at least 7 days later. Plasma HIV-1 RNA viral load and T cell subsets were determined before after cART discontinuation. Data were obtained from the FIPSE OLT-HIV-05-GESIDA 45-05 database. Results: Ten patients were off cART at 6-9 days of OLT, 11 after 10-17 days and 4 after 28 days. The 25 cases had been on cART for a median (IQR) of 4.80 (1.04-8.56) years. Median (IQR) pre-HAART pVL was 4.63 (3.29; 5.03) log
José M. Miró,1 Juan González,2 Pilar Miralles,3 Miguel Montejo,4 Juan C. Meneu,5
10 copies/mL. cART based on efavirenz, a protease inhibitor or other combinations at OLT was taken in 8, 7 and 10
Antonio Rafecas,6 Montserrat Tuset,1 Elisa Cordero,7 Iñaki Pérez,1 Antonio
cases, respectively. Median (IQR) CD4+ and CD8+ T-cell counts before discontinuation were 321 (200-408) and 487 (297;724) cells/mm3, respectively. A cyclosporine A (CsA)–based immunosuppressive regimen was started in
Rimola,1 and the GESIDA/FIPSE OLT in HIV-Infected Patients Research Group
40% patients and a tacrolimus-based regimen in 60%. A rebound in pVL was detected at 6-17 days in 6 out of 24 patients (25%; 95% CI 12%;45%). Only one of the patients on CsA had a pVL rebound at 2 weeks (P=.18). pVL
1Hosp. Clínic - IDIBAPS. Univ. of Barcelona, Barcelona; 2Hosp. Univ. La Paz, Madrid; 3Hosp. Univ.
rebound was higher than 10,000 copies/mL at 6-9, 10-17 and 28 days in only 1, 1 and none case, respectively.
Gregorio Marañón, Madrid; 4Hosp. Univ. Cruces, Baracaldo; 5Hosp Univ. 12 de Octubre, Madrid;
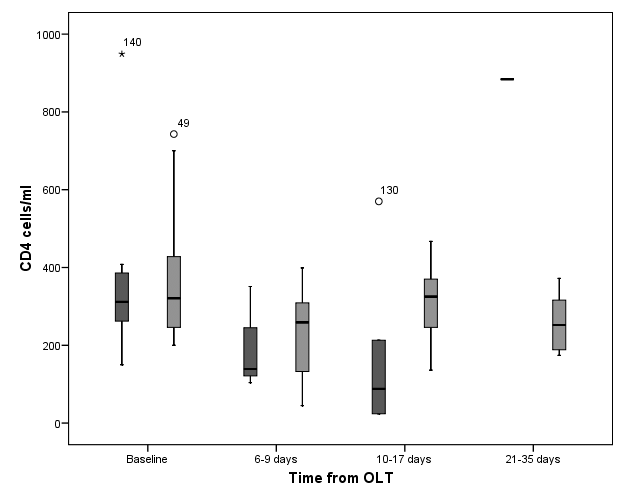
Median CD4+ T-cell counts at 6-9, 10-17 and 28 days were 231 (104;342), 229 (88;356) and 316 (241;608),
6Hosp. Bellvitge - IDIBELL. Univ. Barcelona, Barcelona; 7 Hosp. Univ. Virgen del Rocio, Sevilla;
respectively (P<.05 at 6-9 and 10-17 days in comparison with baseline). Plasma VL returned to undetectable levels
following reintroduction of cART in all cases Conclusions: pVL remained BDL or rebounded at a very low level of viremia in most HCV-HIV OLT recipients after
2-4 weeks off HAART, probably due to the reduction in the T-cell immune activation induced by OLT immunosuppressive therapy. PATIENTS & METHODS
Discontinuation of combined antiretroviral therapy (cART) in
• We included 25 HCV/HIV-coinfected patients on cART who
chronic HIV-1 infection (CHI) is accompanied by a rapid rise in
underwent OLT between 2002-2006 and had a pVL below
plasma HIV-1 RNA viral load (pVL) and a decrease in CD4+ T-
detection levels (<50 copies/mL) at OLT, and who temporarily
cell counts (Garcia F et al. AIDS. 1999; 13:F79-F86). However,
pVL and immunological dynamics following temporary
discontinuation of cART after OLT in HIV-1–infected patients on
• Plasma HIV-1 RNA viral load and T-cell subsets were
immunosuppressive therapy has not been well characterized.
determined before resumption of cART (at 1, 2 or 4 weeks).
Clinical, virological, and immunological data were obtained
from the FIPSE OLT-HIV-05-GESIDA 45-05 database.
The aim of this study is to describe the short-term (4 weeks)
• pVL rebound was compared with a historical cohort of 8
dynamics of pVL and CD4/CD8 subset changes after
patients with CHI who stopped cART after 1 year of effective
treatment (Garcia F. AIDS. 1999;13:F79-F86). STATISTICAL ANALYSIS Patient Characteristics (I)
• Continuous variables were assessed using the t test for normally
distributed data or the Mann-Whitney U test for non-normally
distributed data. Categorical variables were compared using the Fisher exact test.
The analysis was performed using SAS version 9.1.3 software (SAS
Institute, Cary, NC, USA) and the level of significance was
HIV-risk factors Immunosuppressive regimen
•Data from Garcia F et al., AIDS 1999;13:F79-F86. All patients were treated with a
ritonavir-boosted PI-based regimen; ** Median (IQR); NA=not applicable. Patient Characteristics (II) cART Before and After OLT (I) Antiretroviral regimen When cART was restarted
* T20+SQV+3TC — T20+TDF+FPV — DDI+EFV+SQV/r
* Data from Garcia F et al. AIDS 1999;13:F79-F86; ** Median (IQR). cART Before and After OLT (II) Plasma HIV-1 RNA Viral Load Rebound After OLT
• Plasma HIV-1 RNA viral load rebound (>200 cp/mL) after 6-
17 days of cART discontinuation was detected in 6 out of 24 patients (25%; 95% confidence interval, 12%-45%). Only
pVL >200 c/mL after cART D/C
one had a VL rebound >500,000 cp/mL.
• Median (IQR) time for restarting cART after OLT was 16 (13;
pVL rebound >4 log10/mL
Twelve patients (48%) received the same cART regimen.
• All patients reached a plasma HIV-1 RNA viral load below
detectable levels following reintroduction of cART.
* Data from Garcia F et al. AIDS 1999;13:F79-F86; NA=not applicable. Plasma HIV-1 RNA Viral Rebound After OLT Predictors of Plasma VL Rebound > 200 cp./mL Variable No. +ve/Total (%) P value Immunosuppressive regimen Antiretroviral regimen Length of cART before OLT CD4+ T-cell count before OLT Peak VL before starting cART Days after OLT Evolution of CD4 and CD8 in Patients With/out Evolution of CD4 and CD8 Counts in Patients With/out cART Discontinuation After OLT (≤ 4 Weeks) cART Discontinuation After OLT (≤ 4 Weeks) Off cART after OLT On cART after OLT CD4+ T-cell counts CD8+ T-cell counts
* P<.05 at 6-9 and 10-17 days in comparison with baseline. CONCLUSIONS SITES AND INVESTIGATORS (I)
• Plasma HIV-RNA viral load remained below detectable levels
HOSP. DE BELLVITGE – U.B. (BARCELONA)
or rebounded at a very low level of viremia in most HCV/HIV-
A. Rafecas, FX Xiol, J.Fabregat, J.Carratálá, N. Fernández, R. Lastra et al. HOSP. RAMON Y CAJAL (MADRID)
coinfected OLT recipients after 2-4 weeks off cART in
R. Barcena, J. Fortún, C. Quereda, S. Moreno, P. Martín, M. García, AM. Moreno,
comparison with chronically HIV-infected patients who
HOSP. VALL D´HEBRON – U.A.B. (BARCELONA)
V. Vargas, Ll. Castells, E. Ribera, A. Pahissa, JI. Esteban, J. Gavaldá, R. Charco, O. Len.
HOSP. DE CRUCES (VIZCAYA)
pVL returned to undetectable levels following reintroduction of
M. Montejo, A. Valdivieso, M. Gastaca, P. Ruiz, A. Ventoso, J. Gonzalez, M. Testillano,
cART in all cases, suggesting that no mutations associated
J. Bustamante, M.J. Suarez, J.R. Fernandez, E. Montejo, J. Ortiz de Urbina. HOSP. CLINIC - IDIBAPS – U.B. (BARCELONA)
with antiretroviral resistance had been selected.
JM Miró, A. Rimola, A. Moreno, C. Manzardo, M. Laguno, F.Aguero, M. López-Dieguez, M. Tuset,
C. Cervera, M. Monras, J. Mallolas, J. Blanch, C. Lanaspa, I. Pérez, E. de Lazzari, JM Gatell.
This low level of viremia was probably due to the reduction in
HOSP. UNIV. GREGORIO MARAÑON (MADRID)
the T-cell immune activation induced by immunosuppressive
R. Bañares, P. Miralles, M. Salcedo, J. Cosín, JC López Bernaldo de Quirós, J. Berenguer et al. HOSP. UNIV. VIRGEN DEL ROCIO (SEVILLA)
E. Cordero, JM. Cisneros, MA. Gómez, M. Sayago, JM. Pascasio, C. Bernal, JM. Sousa et al. SITES AND INVESTIGATORS (II) ACKNOWLEDGEMENTS HOSP. UNIV. LA FE (VALENCIA)
M. Blanes, M. Prieto, J. López, M. Berenguer et al.
HOSP. UNIV. REINA SOFIA (CORDOBA)
- Fundación para la Investigación y Prevención del SIDA en España
J.Torre-Cisneros, M. de la Mata, JJ Castón, S. Rufian, P. López, A. Rivero,
A. Camacho, C. Natera, E. Vidal, R. Lara et al. HOSP. UNIV. CENTRAL DE ASTURIAS (OVIEDO)
- Grupo de Estudio de Sida (GESIDA/SEIMC).
M. Rodríguez, I. González-Pinto, V. Asensi, MP. Alonso , ML. González-Diéguez.
- Sociedad Española de Trasplante Hepático (SETH). HOSP. UNIV. VIRGEN DE LA ARRIXACA (MURCIA)
- Grupo de Estudio de Infecciones en Trasplantados.
HOSP. CARLOS HAYA (MALAGA)
M. Jiménez, JM. Rodrigo, J. Santoyo, JL. Fernández, J. de la Cruz et al. HOSP. 12 DE OCTUBRE (MADRID)
M. Abradelo, F. Pulido, R. Rubio, E. Moreno, S. Olivares et al.
- Secretaria del Plan Nacional del Sida (SPNS) del Ministerio de
HOSP. UNIV. JUAN CANALEJO (LA CORUÑA)
JD. Pedreira, F. Suárez, S. López, P. Vázquez, MA. Castro. HOSP. UNIV. MARQUES DE VALDECILLA (SANTANDER)
- Organización Nacional de Trasplante (ONT).
MC. Fariñas, JD. García, S. Echevarría, E. Fábrega, F. Casafont et al. HOSP. UNIV. SANTIAGO DE COMPOSTELA (LA CORUÑA)
A. Antela, E. Losada, E. Varo, J. Fernández. HOSP. CLINICO LOZANO BLESA (ZARAGOZA)
R. Lozano, E. Tejero, S. Letona,, JJ. Araiz, P. Luque, A. Navarro et al.
Welcome to Princess Street Group Practice . Please carefully complete this registration form. Your answers will help us to plan services that can help to improve your health. If you have any problems completing this form please ask reception for help. We may have some questions to ask you regarding your answers so a member of the reception team will go through your completed form with you.
SINEMET® & SINEMET® CR Carbidopa/levodopa PRESCRIBING INFORMATION Refer to Summary of Product Characteristics (SPC) before prescribing Adverse events should be reported. Reporting forms and information can be found at . Adverse events should also be reported to MSD (tel: 01992 467272). PRESENTATION Sinemet 12.5 mg/50 mg Tablets contains 12.5 mg of anh
 Evolution of CD4 and CD8 in Patients With/out
Evolution of CD4 and CD8 in Patients With/out 
 SITES AND INVESTIGATORS (II)
SITES AND INVESTIGATORS (II)