0022-5347/99/1622-0421/0THE JOURNAL OF UROLOGY
Copyright 1999 by AMERICAN UROLOGICAL ASSOCIATION, INC.
PROSTATE BRACHYTHERAPY: TREATMENT STRATEGIES
From the Departments of Urology and Radiation Oncology, Mount Sinai School of Medicine, Mount Sinai Medical Center,
Purpose: Patients who present with localized and locally advanced prostate cancer may be
candidates for prostate brachytherapy. We evaluated the treatment outcomes in a diverse groupof prostate cancer patients who presented with low, moderate and high risk features.
Materials and Methods: A total of 301 patients who presented with T1 to T3 prostate cancer were
treated with brachytherapy alone or combined with hormonal therapy and/or external beam irradi-ation. Of these patients 109 at low risk with prostate specific antigen (PSA) 10 ng./ml. or less, Gleasonscore 6 or less and clinical stage T2a or less were treated with 125iodine alone, 152 at moderate riskwith PSA greater than 10 ng./ml., Gleason score greater than 6 or stage T2b or greater were treatedwith 125iodine or 103palladium or combined implant alone with 5 months of hormonal therapy, and 40at high risk with PSA greater than 15 ng./ml., Gleason 8 or greater, clinical stage T2c to T3 or positiveseminal vesicle biopsy (20) were treated with combination brachytherapy, external beam irradiationand 9 months of hormonal therapy. Patients with a positive seminal vesicle biopsy (T3c disease) andnegative pelvic lymph nodes were included in the high risk group, and the walls of the seminalvesicles were also treated with implantation. Followup was performed every 6 months with digitalrectal examination and ultrasound evaluation. Prostate biopsy was routinely recommended 2 yearsafter completion of the radiation. Failure was defined as PSA increase on 2 consecutive determina-tions above 1 ng./ml. or evidence of local recurrence on digital rectal examination, transrectalultrasound or biopsy. Kaplan-Meier projections were used to calculate progression-free survivalrates.
Results: Of the 109 patients at low risk followed from 1 to 7 years (median 18 months) 91%
were free of PSA failure at 4 years. No patient experienced urinary incontinence followingimplantation, although grade 1 to 2 radiation proctitis occurred in 5 (4.5%). Of the 152 patientsat moderate risk 73 received implantation and 79 received implantation combined with hormonaltherapy. The 4-year biochemical freedom from failure rate for the hormone group was 85% versus58% for the no hormone group (p ϭ 0.08). The difference was more significant for those withGleason score 7 or greater (90 versus 43%, p ϭ 0.01) and for those with PSA greater than 10ng./ml. (87 versus 59%, p ϭ 0.04). Grade 1 to 2 radiation proctitis occurred in 1 of the 79 patients(1.3%) receiving hormonal therapy and in 3 (4%) treated with implantation only. There were nocases of urinary incontinence. Of the 40 patients at high risk 71% were free of biochemical failureat 3 years. Of the 4 patients with failure (10%) 3 (75%) originally had positive seminal vesiclebiopsies. Five patients experienced gastrointestinal complications, although none was grade 3 or4. The actuarial freedom from grade 2 proctitis was 82%. No patient experienced urinaryincontinence. Prostate biopsies were negative in 87% of the low risk, 96.8 (hormone group) versus68.6% (no hormone group) of the moderate risk (p ϭ 0.0023) and 86% of the high risk patients.
Conclusions: Brachytherapy appears to offer comparable results to external beam irradiation
and radical prostatectomy when patients are stratified by disease extent. Adopting a strategy ofimplant alone, implant with hormonal therapy or implant with hormonal therapy and externalbeam irradiation in patients who present with low to high risk features can improve the overallresults in the more advanced cases.
KEY WORDS: prostatic neoplasms, brachytherapy, radiation
Reports on the efficacy and low morbidity of prostate
brachytherapy have generated increased interest in this new
Preplanned implant. Holm et al first described the use of
treatment modality for patients and physicians. With long-
transrectal ultrasound to plan seed placement,2 and physi-
term data recently becoming available, this procedure is now
cians at the Northwest Hospital perfected this technique
being widely embraced by urologists and radiation oncolo-
which uses axial images to generate a treatment plane.1, 3
gists.1 Selection of appropriate candidates for implant alone
The implant needles, guided by the preplan, are inserted
or combined with external beam irradiation and/or hormonal
through the template and perineum, and into the prostate.
therapy has not been adequately studied. We describe the
Transrectal ultrasound is used not to direct seed placement,
ultrasound guided approach to permanent prostate seed im-
but rather to recreate the preplan and ensure that the im-
plantation, and detail the efficacy and morbidity outcomes of
plant needles are placed accordingly. Seeds are inserted via
the procedure in a diverse group of patients with low, mod-
preloaded needles, polyglycolic acid strands or the Mick ap-
erate and high risk prostate cancer.
For early implants uniform seed spacing was used,4 while
might best benefit from prostate brachytherapy.13–18 Even-
later implants were performed with peripheral weighting to
tually, an analysis of the effect of PSA, stage and grade on
decrease the dose to the urethra.5 The Northwest Hospital
outcome confirmed the same prognostic significance of these
series has the longest followup and compares favorably with
factors following brachytherapy.9 Based on these results, low
radical prostatectomy.6 Urinary complications can be signif-
risk patients who might best benefit with implant alone were
icant and result from the high dose delivered to the center of
identified. Low risk was defined as stage T2a or less, Gleason
the gland close to the urethra from the uniformly spaced
sum less than 7 and PSA 10 ng./ml. or less. These patients
seeds. Patients who undergone a prior transurethral resec-
had significantly improved outcome compared to higher risk
tion of the prostate and who were treated with this technique
patients when treated with 125I implant alone.19
had a 12% incontinence rate.6 Based on these data, such
Patients with more advanced localized disease were found
patients were not considered suitable for a preplanned uni-
to benefit from the addition of hormonal therapy to the ex-
form implant. In addition, pubic arch interference also lim-
ternal beam regimen.20, 21 While the addition of neoadjuvant
ited this technique. Rectal complications and erectile dys-
hormonal therapy appeared to offer an advantage in patients
with large prostates who underwent seed implantation, no
Real-time interactive prostate implantation. Real-time in-
substantial information was available to evaluate its benefit
teractive seed implantation is the newest technique to be
in high risk patients undergoing brachytherapy.22 The addi-
used for prostate brachytherapy and takes advantage of the
tion of neoadjuvant hormonal therapy in patients who pre-
ability of transrectal ultrasound to provide precision target-
sented with stage T2b or greater, PSA greater than 10 ng./ml.
ing.7–9 Before implantation the prostate volume is measured.
or Gleason score 7 or greater might yield similar favorable
Using an activity per volume table, the appropriate amount
results as seen in the combination hormonal therapy, exter-
of activity is ordered and brought to the operating room. With
nal beam studies. Also patients who presented with PSA
the patient in the dorsal lithotomy position and a Foley
greater than 20 ng./ml. responded poorly to implant alone.18
catheter in place, a C-arm fluoroscopic image intensifier is
Data on external beam irradiation and radical prostatectomy
positioned over the bladder and prostate. An electronic
revealed high recurrence rates in patients with poor prognos-
phased array biplanar probe is positioned in the rectum to
tic factors,13, 23, 24 and prostatectomy data indicated poor out-
ensure that the entire prostate is visible. The perineum is
comes for patients with pathologically involved seminal ves-
then prepared and the template is attached to the stepping
icle disease. Based on these data an aggressive treatment
unit. Using transverse imaging serial contours of the pros-
regimen was developed, which included hormonal therapy,
tate are measured at 5 mm. intervals from base to apex. This
brachytherapy and conformal external beam irradiation to
planimetry volume is used when calculating the amount of
treat patients with PSA greater than 15 ng./ml., Gleason
activity to implant. The treatment plan is created in the
score 8 to 10, clinical stage T2C to T3 or positive seminal
operating room. The total activity is divided by activity per
seed (usually 0.3 to 0.5 mCi. per seed for 125iodine [I] and 1.0to 1.5 mCi. per seed for 103palladium [Pd]) to give the total
number of seeds to implant. After the volume measurements
A total of 301 patients who presented with T1 to T3 pros-
are completed, imaging is switched to longitudinal, and meas-
tate cancer were treated with brachytherapy alone or com-
urements are made anterior and posterior to the urethra, and
bined with hormonal therapy and/or external beam irradia-
posterior from base to apex. These longitudinal meas-
tion (table 1). There were 109 patients at low risk with PSA
urements are used to determine the spacing between the
10 ng./ml. or less, Gleason score 6 or less and clinical stage
T2a or less treated with 125I alone, 152 at moderate risk with
Current isotope choices for permanent prostate seed im-
PSA greater than 10 ng./ml., Gleason score greater than 6 or
plantation are 125I and 103Pd. 125I is selected for patients
stage T2b or greater treated with 125I or 103Pd implant alone
with Gleason score 6 or less on biopsy and 103Pd is used in
or combined with 5 months of hormonal therapy, and 40 at
patients with Gleason 7 or greater. 103Pd is also selected for
high risk with PSA greater than 15 ng./ml., Gleason 8 or
high risk patients who are to receive a combination of seed
greater, or clinical stage T2c to T3 or positive seminal vesicle
implant and external beam irradiation (implant is done first
biopsy (20) treated with combination brachytherapy, exter-
with 67% of the full dose followed 2 months later with exter-
nal beam irradiation and 9 months of hormonal therapy. Low
nal beam at 45 Gy.). The details of this implant technique
risk patients were implanted with 125I to a dose of 160 Gy.
have been previously described.7–9 A month after implanta-
(TG43 guidelines) and moderate risk patients were im-
tion the patient returns for evaluation with a 3-dimensional
planted with 125I for Gleason score of 6 or less or 103Pd to a
(D) computerized tomography (CT) dosimetric system. CT
dose of 115 Gy. for Gleason 7 or greater. Hormonal therapy
images of the prostate are taken at 3 to 5 mm. intervals from
was administered for 3 months before and for 2 months after
the base of the bladder to the sphincter to assess the quality
implant in 79 of the moderate risk patients, while 73 received
of the implant. These images are then digitized and recon-
implantation alone. High risk patients received an implant of
structed in 3-D to give dose volume histograms and dose
103Pd to a dose of 56 to 86 Gy. combined with external beam
surface histograms of the prostate, rectal wall and bladder
irradiation to a dose or 4,500 to 7,040 cGy. Conformal 3-D
base, respectively. This information is critically important for
external beam irradiation was delivered via 6 fields (2 ante-
evaluating the adequacy of the implant and helps newly
rior oblique, 2 posterior oblique and 2 lateral fields) with a 2
trained physicians assess and improve their technique.10
cm. margin to the prostate and seminal vesicles. High riskpatients were treated according to an institutional review
In the past few data were available to help guide patient
selection for brachytherapy. Cases were often staged with
TABLE 1. Clinical features of patients treated with brachytherapy
little more than a bone scan and CT. The addition of bilateral
ultrasound guided seminal vesicle biopsy and laparoscopic
lymph node dissection helped to identify further patientswith extraprostatic disease.11, 12 Studies reporting the prog-
nostic significance of prostate specific antigen (PSA) and
grade in predicting outcome after external beam irradiation
Low risk patients must have all features to be included in that category,
and prostatectomy also helped further define which patients
while moderate or high risk patients need only 1 feature present.
board approved 103Pd dose escalation study, and received 3months of hormonal therapy before implant and continuedandrogen withdrawal therapy for 6 months after implant(total 9 months). Patients on the institutional review boardprotocol also received a higher dose of external beam irradi-ation to 5,940 and 7,040 cGy. and the implant dose was alsoescalated from 56 to 76 to 86 Gy. as part of this protocol. Those patients with a positive seminal vesicle biopsy (T3cdisease) and negative pelvic lymph nodes were included inthe high risk group and additionally the walls of the seminalvesicles were also treated with implantation. Hormonal ther-apy was administered as a combination of leuprolide acetateand 250 mg. flutamide every 8 hours in all patients.
All cases were staged with routine bone scans and CT. All
patients with PSA greater than 10 ng./ml., Gleason 7 orgreater or clinical stage T2b or greater also underwent bilat-eral seminal vesicle biopsy. Those patients with PSA greaterthan 15 ng./ml., Gleason score greater than 7 or a positiveseminal vesicle biopsy underwent laparoscopic pelvic lymphnode dissection before treatment,22, 23 and those with posi-tive nodes were excluded from implantation. Followup was
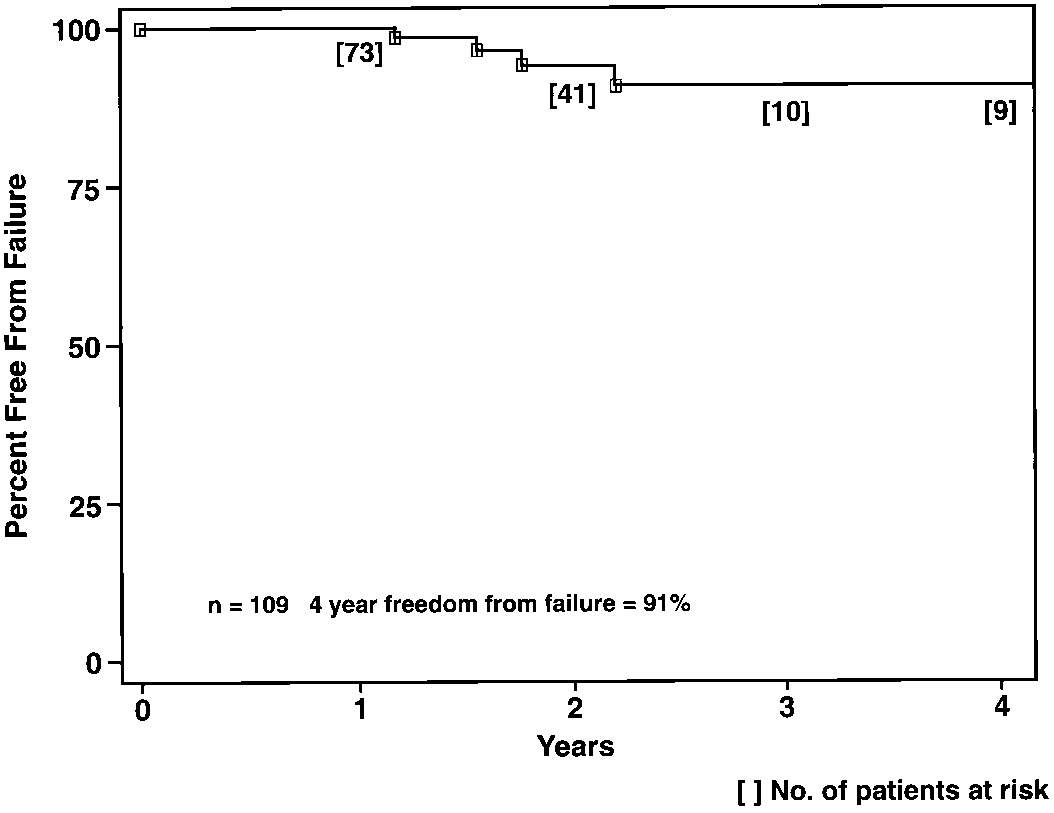
FIG. 1. Four-year freedom from PSA failure in low risk patients
performed every 6 months with PSA, digital rectal examina-
with PSA 10 ng./ml. or less, Gleason 6 or less and clinical stage T2a
tion and ultrasound evaluation. Prostate biopsies, including
6 from the prostate and 6 from the seminal vesicles forpatients with a positive seminal vesicle biopsy, were rou-
TABLE 3. Clinical features of 152 moderate risk patients
tinely recommended 2 years after completion of treatment
regardless of disease status. Followup was started at comple-
tion of therapy (date of implant or completion of external
beam irradiation). PSA failure was defined as 2 elevations
above 1 ng./ml. Comparisons between survival rates were
calculated using the log rank test, and differences in propor-
tions were tested using the Pearson chi-square method.
The 109 patients at low risk received 125I alone, and fol-
lowup ranged from 1 to 7 years (median 18 months). PSA
ranged from 1.3 to 10 ng./ml. (median 6.4), a third of the
patients had Gleason scores 2 to 4 and an equal number had
T1c and T2a lesions (table 2). The 4-year freedom from PSA
Hormonal group was treated for 3 months before and 2 months after implant
failure rate was 91% (fig. 1). No patient experienced urinary
incontinence following implantation. Grade 1 to 2 radiationproctitis occurred in 5 men (4.5%) and there were no cases of
of grade 3 or 4 radiation proctitis and no cases of urinary
The 152 patients at moderate risk were followed a median
The 40 patients at high risk underwent a combination of
of 27 months (range 12 to 74) and were treated with either
hormonal therapy and 103Pd implantation followed by exter-
implantation alone (73) or implant combined with hormonal
nal beam irradiation. PSA ranged from 2.1 to 202 ng./ml.
therapy (79). The patients were equally distributed with
(median 20), 32 had Gleason score 7 or greater (80%) and 34
regard to stage, PSA and Gleason score (table 3). The 4-year
had clinical stage T2b or greater (85%). Of the 40 patients 20
biochemical freedom from failure rate for the hormone group
had biopsy confirmed seminal vesicle involvement (table 4).
was 85% versus 58% for the no hormone group (p ϭ 0.08, fig.
Followup ranged from 6 to 42 months (median 13). The
2, A). The difference was more significant for those with
3-year biochemical freedom from failure rate in these high
Gleason score 7 or greater (90 versus 43%, p ϭ 0.01, fig. 2, B)
risk patients was 71% (fig. 3). Of the 4 patients (10%) with
and for those with PSA greater than 10 ng./ml. (87 versus
failure 3 (75%) originally had positive seminal vesicle biop-
59%, p ϭ 0.04, fig. 2, C). Grade 1 to 2 radiation proctitis
sies. The time to failure in these 4 patients ranged from 226
occurred in 1 patient receiving hormonal therapy (1.3%) and
to 712 days (mean 446). The last PSA value in the 36 patients
in 3 treated only with implantation (4%). There were no cases
without failure was less than 0.05 ng./ml. in 21 (58.3%), 0.05to 0.2 in 13 (36.1%) and greater than 0.2 to 0.5 in 2 (5.6%). All5 patients who received 5,940 cGy. external beam dose hadgastrointestinal complications. There were no grade 3 or
TABLE 2. Clinical features of 109 low risk patients
4 gastrointestinal complications. The actuarial freedom from
grade 2 proctitis was 82%. No patient experienced urinary
incontinence. Prostate biopsies were negative in 87% of the
low risk, 96.8 (hormone group) versus 68.6% (no hormone
group) of the moderate risk (p ϭ 0.0023) and 86% of the high
The rationale for using brachytherapy alone in low risk
patients evolved from the experience at several centers
FIG. 2. Effect of hormonal therapy on PSA failure. Four-year biochemical freedom from failure for moderate risk patients treated with or
without hormones (p ϭ 0.08, A), with Gleason 7 or greater (p ϭ 0.01, B) and with PSA 10 ng./ml. or greater (p ϭ 0.04, C).
TABLE 4. Clinical features of 40 high risk patients
FIG. 3. Three-year freedom from PSA failure in high risk patients
with PSA greater than 15 ng./ml., Gleason 8 or greater, or clinical
stage T2c to T3 or positive seminal vesicle biopsy treated with
combination brachytherapy, external beam irradiation and 9 monthsof hormonal therapy.
The highest dose given was combination of 86 Gy. of 103Pd followed by 5,940
cGy. external beam irradiation in 6 patients.
TABLE 5. Prostate biopsy results in low to high risk patients
where implants have been performed for a considerable time.
Ragde et al reported on 126 men followed a mean of 69
months who received a 125I implant.6 While the results were
not stratified by the presenting risk factors, most of their
cases would fit into the definition of low risk. Median PSA
The difference in positive biopsy results between the moderate risk patients
treated with and without hormonal therapy was significant (p ϭ 0.0023).
was 5.0 ng./ml., which is similar to the low risk median 6.4ng./ml. in our study. In addition, 85.3% of their patients hadclinical T2a or less disease, all had Gleason 6 or less and78.7% had PSA 10 ng./ml. or less. One might argue that their
group defined as PSA greater than 4 to 10 ng./ml. and
patients represented an even more favorable group than ours
Gleason score 4 or less. The 2-year PSA failure-free survival
because 44.3% had PSA from 0 to 4 ng./ml. compared to only
was 87% for the radical prostatectomy cases with organ con-
15.6% in our series. Nonetheless, the 7-year actuarial PSA
fined disease and 92% for those who received external radi-
progression-free outcome was 87% for PSA 1.0 ng./ml. or less
ation. Vicini et al performed an extensive review of patients
and 79% for PSA 0.5 ng./ml. or less. These numbers compare
who received external beam irradiation and analyzed the
favorably to our own report of 91% freedom from PSA pro-
data by presenting PSA.28, 29 Biochemical control rates for 6
gression. The progression-free results in these low risk pa-
centers that reported data for patients who presented with
tients treated with 125I alone also compare favorably to what
initial PSA 4.0 ng./ml. or less ranged from 69 to 93%. For
has been reported for similar groups of patients treated with
patients with PSA 4 to 10 ng./ml. the success rate was 44 to
radical prostatectomy or external beam irradiation. In a
84%. They also analyzed 5 brachytherapy series with pre-
group of clinically similar patients who underwent radical
senting PSA between 4 and 10 ng./ml. and found a 55 to 90%
retropubic prostatectomy, Catalona and Bigg reported a 78%
success rate (PSA 0.6 ng./ml. or less) at 5 years,25 and Partin
Patients who present with moderate risk disease do not do as
et al reported an 83% freedom from PSA failure rate (PSA 0.3
well as those with low risk disease regardless of the treatment
modality. D’Amico et al defined an intermediate risk category
D’Amico et al evaluated the effect of presenting risk fea-
as PSA greater than 4 to 10 ng./ml. and Gleason score 5 to 7 or
tures on 867 and 757 consecutive prostate cancer patients
PSA greater than 10 to 20 ng./ml. and Gleason score 7 or less.27
treated with external beam irradiation or radical retropubic
The 2-year success rate for radiation therapy and radical pros-
prostatectomy.27 Patients were separated into a low risk
tatectomy was 81 and 77%, respectively. Kupelian et al re-
ported a 60 to 70% 5-year success rate with these 2 treatment
recognize that followup for biochemical control in this study
modalities when cases were stratified by PSA greater than 10 to
is relatively short and that longer followup will be needed to
20 ng./ml.30, 31 Biochemical control rates for patients with PSA
substantiate these findings. Brachytherapy also has few side
greater than 10 to 20 ng./ml. reported in 6 conventional radia-
effects, even when combined with conventional doses of ex-
tion therapy series ranged from 27 to 72%.28, 29 The same study
reported brachytherapy results from 5 centers with reportedsuccess rates ranging from 45 to 89%. Our own data also sug-gest inferior results compared to patients with low risk disease.
The 4-year success rate for the implant alone cases was only58% which contrasted to 85% for those treated with a combina-
1. Ragde, H., Elgamal, A. A., Snow, P. B., Brandt, J., Bartolucci,
A. A., Nadir, B. S. and Korb, L. J.: Ten-year disease free
tion of hormonal therapy and seed implantation. The difference
survival after transperineal sonography-guided iodine-125
was more significant in patients with PSA greater than 10
brachytherapy with or without 45-gray external beam irradi-
ng./ml. (87 versus 59%, p ϭ 0.04) and in patients with Gleason
ation in the treatment of patients with clinically localized, low
score 7 or greater (90 versus 43%, p ϭ 0.01).
to high grade prostate carcinoma. Cancer, 83: 989, 1998.
The most difficult cases to treat successfully are those with
2. Holm, H. H., Juul, N., Pedersen, J. F., Hansen, H. and Stoyer, I.:
locally advanced prostate cancer at presentation. We previ-
Transperineal 125 iodine seed implantation in prostatic carci-
ously reported a 58% 2-year and 34% 4-year freedom from
noma guided by transrectal ultrasonography. J. Urol., 130:
biochemical progression in men who presented with initial
PSA greater than 20 ng./ml. treated with implant alone with
3. Blasko, J. C., Wallner, K., Grimm, P. D. and Ragde, H.: PSA
based disease control following ultrasound guided I-125 im-
or without hormonal therapy.9, 19 Freedom from failure rates
plantation for stage T1/T2 prostatic carcinoma. J. Urol., 154:
for similar patients treated with conventional external beam
irradiation or conformal radiation therapy range from 8 to
4. Quimby, E. H.: The grouping of radium tubes in packs and
37%.22, 27, 28 Radical prostatectomy success rates in these
plaques to produce the desired distribution of radiation. AJR,
high risk patients are equally disappointing, as Kupelian et
27: 18, 1932.
al reported a 25% likelihood of freedom from failure at 5
5. Paterson, R. and Parker, H. M.: A dosage system for gamma-ray
therapy, Parts 1 and 2. Brit. J. Rad., 7: 592, 1943.
We elected to combine brachytherapy with external beam
6. Ragde, H., Blasko, J. C., Grimm, P. D., Kenny, G. M., Sylvester,
irradiation and neoadjuvant and adjuvant hormonal therapy
J. E., Hoak, D. C., Landin, K. and Cavanagh, W.: Interstitialiodine-125 radiation without adjuvant therapy in the treat-
to attempt to improve the poor results in these high risk
ment of clinically localized prostate cancer. Cancer, 80: 442,
patients. The rationale for the combination of seed implant
and external beam irradiation evolved from the dose re-
7. Stone, N. N., Stock, R. G., DeWyngaert, J. K. and Tabert, A.:
sponse data in high risk patients treated with external beam
Prostate brachytherapy: improvements in prostate volume
alone and from the initial favorable reports of combination
measurements and dose distribution using interactive ultra-
irradiation from several centers.31–34 The addition of com-
sound guided implantation and three-dimensional dosimetry.
plete hormonal therapy also evolved from randomized stud-
Rad. Oncol. Invest., 3: 185, 1995.
ies documenting the advantage of androgen withdrawal in
8. Stock, R. G., Stone, N. N., Wesson, M. F. and DeWyngaert, J. K.:
locally advanced prostate cancer treated with external beam
A modified technique allowing interactive ultrasound guided
irradiation.20, 21 The favorable 3-year freedom from PSA fail-
three-dimensional transperineal prostate implantation. Int. J. Rad. Oncol. Biol. Phys., 32: 219, 1995.
ure in this group of high risk patients (50% of whom had
9. Stock, R. G., Stone, N. N., DeWyngaert, J. K., Lavagnini, P. and
biopsy proved T3c disease) suggests that tri-modal therapy
Unger, P. D.: Prostate specific antigen findings following in-
(seeds plus external beam plus hormonal therapy) may offer
teractive ultrasound guided transperineal brachytherapy for
a significant improvement over standard monotherapy with
early stage prostate carcinoma. Cancer, 77: 2386, 1996.
radiation or radical prostatectomy alone. The data also sug-
10. Stock, R. G., Stone, N. N., Tabert, A., Iannuzzi, C. and
gest that this treatment is successful at eradicating all local
DeWyngaert, K.: A dose response study for I-125 prostate
disease with a 2-year negative biopsy rate of 86%.
implants. Int. J. Rad. Oncol. Biol. Phys., 41: 101, 1998.
Our data also suggest that brachytherapy can be accom-
11. Stock, R. G., Stone, N. N., Ianuzzi, C. and Unger, P.: Seminal
plished with low morbidity. No patient had incontinence,
vesicle biopsy and laparoscopic pelvic lymph node dissection:implications for patient selection in the radiotherapeutic man-
cystitis or significant radiation proctitis (grade 3 or higher).
agement of prostate cancer. Int. J. Rad. Oncol. Biol. Phys., 33:
The incidence of grade 1 to 2 radiation proctitis in the low to
moderate risk patients ranged from 1.3 to 4.5%. Patients who
12. Stone, N. N., Stock, R. G. and Unger, P.: Indications for seminal
received a combination of seeds and external beam irradia-
vesicle biopsy and laparoscopic pelvic lymph node dissection in
tion had an actuarial 18% incidence of grade 1 to 2 proctitis.
men with localized carcinoma of the prostate. J. Urol., 154:
There was no grade 2 proctitis in 11 of the 40 patients who
received external beam irradiation to a dose of less than
13. Zeitman, A. L., Coen, J. J., Shipley, W. U., Willet, C. G. and
5,940 cGy. Thus, this higher incidence of grade 2 proctitis
Efrid, J. T.: Radical radiation therapy in the management of
was only found in those patients receiving high doses of
prostatic adenocarcinoma: the initial prostate specific antigen
external beam irradiation. This study is part of an ongoing
value as a predictor of treatment outcome. J. Urol., 151: 640, 1994.
institution review board approved dose escalation trial to
14. Zagars, G. K.: Prostate specific antigen as an outcome variable
determine whether an external dose beyond the conventional
for T1 and T2 prostate cancer treated by radiation therapy.
dose of 4,500 cGy. offers an advantage in these high risk
J. Urol., 152: 1786, 1994.
15. Lee, W. R., Hanks, G. E., Schultheiss, T. E., Corn, B. W. and
Hunt, M. A.: Localized prostate cancer treated by externalbeam radiotherapy alone: serum prostate-specific antigen
driven outcome analysis. J. Clin. Oncol., 13: 464, 1995.
Brachytherapy appears to offer comparable results to ex-
16. Hanks, G. E., Lee, W. R. and Schultheiss, T. E.: Clinical and
ternal beam irradiation and radical prostatectomy when
biochemical evidence of control of prostate cancer at 5 years after external beam radiation. J. Urol., 154: 456, 1995.
cases are stratified by disease extent. Adopting a strategy of
17. Zagars, G. K. and Pollack, A.: Radiation therapy for T1 and T2
implant alone, implant with hormonal therapy or implant
prostate cancer: prostate-specific antigen and disease control.
with hormonal therapy and external beam irradiation in
Urology, 45: 476, 1995.
patients who present with low to high risk features can
18. Zeitman, A. L., Edelstein, R. A., Coen, J. J., Babayan, R. K. and
improve the overall results in the more advanced cases. We
Krane, R. J.: Radical prostatectomy for adenocarcinoma of the
prostate: the influence of preoperative and pathologic findings
analysis of clinical and pathological factors that predict for
on biochemical disease free outcome. Urology, 43: 828, 1994.
prostate specific antigen failure after radical prostatectomy for
19. Stock, R. G. and Stone, N. N.: The effect of prognostic factors on
prostate cancer. J. Urol., 154: 131, 1995.
therapeutic outcome following transperineal prostate brachy-
28. Vicini, F. A., Horwitz, E. M., Kini, V. R., Stromber, J. S. and
therapy. Sem. Surg. Oncol., 13: 454, 1997.
Martinez, A. A.: Radiotherapy options for localized prostate
20. Pilepich, M. V., Krall, J. M., Al-Sarraf, M., Madhu, J. J., Doggett,
cancer based upon pretreatment serum prostate-specific anti-
R. L. S., Sause, W. T., Lawton, C. A., Abrams, R. S., Rotman,
gen levels and biochemical control: a comprehensive review of
M., Rubin, P., Shipley, W. U., Grignon, D., Caplan, R. and Cox,
the literature. Int. J. Rad. Oncol. Biol. Phys., 40: 1101, 1998.
J. D.: Androgen deprivation with radiation therapy compared
29. Vicini, F. A., Horwitz, E. M., Gonzalez, J. and Martinez, A. A.:
with radiation therapy alone for locally advanced prostatic
Treatment options for localized prostate cancer based upon
carcinoma: a randomized comparative trial of the radiation
pretreatment prostate specific antigen levels. J. Urol., 158:
therapy oncology group. Urology, 45: 616, 1995.
21. Laverdiere, J., Gomez, J. L., Cusan, L., Suburu, E. R., Diamond,
30. Kupelian, P., Katcher, J., Levin, H., Zippe, C. and Klein, E. I.:
P., LeMay, M., Canadas, B., Fortin, A. and Labrie, F.: Benefi-
Correlation of clinical and pathologic factors with rising
cial effect of combination therapy administered prior and fol-
prostate-specific antigen profiles after radical prostatectomy
lowing external beam radiation therapy in localized prostate
alone for clinically localized prostate cancer. Urology, 48: 249,
cancer. Int. J. Rad. Oncol. Biol. Phys., 37: 247, 1997.
22. Blasko, J. C., Ragde, H., Grimm, P. D., Sylvester, J. and
31. Kupelian, P., Katcher, J., Levin, H., Zippe, C., Suh, J., Macklis,
Cavanagh, W.: Potential for neoadjuvant hormonal therapy
R. and Klein, E.: External beam radiotherapy versus radical
with brachytherapy for prostate cancer. Mol. Urol., 1: 207,
prostatectomy for clinical stage T1–2 prostate cancer: thera-
peutic implications of stratification by pretreatment PSA lev-
23. Hanks, G. E., Hanlon, A. L., Hudes, G., Lee, W. R., Winlove, S.
els and biopsy Gleason scores. Cancer J. Sci. Amer., 3: 78,
and Schultheiss, T.: Patterns of failure analysis of patientswith high pretreatment prostate-specific antigen levels
treated by radiation therapy. The need for improved systemic
32. Hanks, G. E., Martz, K. L. and Diamond, J. J.: The effect of dose
and regional therapy. Int. J. Rad. Oncol. Biol. Phys., 14: 1093,
on local control of prostate cancer. Int. J. Rad. Oncol. Biol.
Phys., 15: 1299, 1988.
24. Kuban, D. A., El-Mahdi, A. M. and Schellhammer, P. F.:
33. Critz, F. A., Levinson, A. K., Williams, W. H. and Holloday, D. A.:
Prostate-specific antigen for pretreatment and post-treatment
Prostate-specific antigen nadir: the optimum level after irra-
evaluation of outcome after definitive irradiation for prostate
diation for prostate cancer. J. Clin. Oncol., 14: 2893, 1996.
cancer. Int. J. Rad. Oncol. Biol. Phys., 32: 307, 1995.
34. Dattoli, M., Wallner, K., Sorace, R., Koval, J., Cash, J., Acosta,
25. Catalona, W. J. and Bigg, S. W.: Nerve-sparing radical prosta-
R., Brown, C., Ethridge, J., Binder, M., Brunelle, R., Kirwan,
tectomy: evaluation of results after 250 patients. J. Urol., 143:
N., Sanchez, S., Stein, D. and Wasserman, S.: Pd-103 brachy-
therapy and external beam irradiation for clinically localized,
26. Partin, A. W., Pound, C. R., Quentin Clemens, J., Epstein, J. I.
high-risk prostatic carcinoma. Int. J. Rad. Oncol. Biol. Phys.,
and Walsh, P. C.: Serum PSA after anatomic radical prosta-
35: 875, 1996.
tectomy. The Johns Hopkins experience after 10 years. Urol.
35. Blasko, J. C., Ragde, H., Cavanagh, W., Sylvester, J. and Grimm,
Clin. N. Amer., 20: 713, 1993.
P. D.: Long-term outcomes of external beam irradiation and
27. D’Amico, A. V., Whittington, R., Malkowicz, S. B., Schultz, D.,
I-125/Pd-103 brachytherapy boost for prostate cancer. Int. J.
Schnall, M., Tomaszewski, J. E. and Wein, A.: A multivariate
Rad. Oncol. Biol. Phys., 36: 198, 1996. Dr. C. A. Olsson. You reported in your series a 15% positive biopsy rate. What do you in this situation?Dr. N. N. Stone. We reported negative prostate biopsies in 87% of the low risk, 96.8 versus 68.6% of the
moderate risk (p ϭ 0.0023, favoring neoadjuvant hormonal therapy) and 86% of the high risk patients. The
options for treating brachytherapy failure cases which have a documented local recurrence (positive biopsy) andno evidence of systemic disease include another seed implant, external beam irradiation, salvage radicalprostatectomy and hormonal therapy. The decision of which to recommend depends on the situation and theresults of post-implant dosimetry. The dosimetry should describe the radiation dose to the prostate, rectum,bladder and urethra. In most cases the radiation dose to the rectum and bladder is much lower than that receivedby a patient initially treated with external beam (the dose to 30% of the rectum averages only 40% of theprescription dose). A repeat implant might be considered if the original implant was done poorly (as defined bydosimetry) and rectal doses were low. Salvage external beam irradiation might be considered if the biopsies werepositive outside of the prostate and the rectal doses were low. Finally, salvage radical prostatectomy might beconsidered if the dose to the prostate was adequate, and the rectal and bladder dose was low. Doctor Olsson. What is the morbidity of a salvage prostatectomy following a radiation seed failure? Are most
failures at 2 years associated with distant relapse?
Doctor Stone. The morbidity of a salvage prostatectomy following a seed implant would in theory be similar to
the morbidity following external beam irradiation. If post-implant dosimetry reveals low dose to the rectum andbladder neck then the radical should be no more difficult than in a previously untreated patient, and this is infact the case. The urologist will need to know the dosimetry before undertaking the salvage radical prostatec-tomy. Local failure at 2 years in low risk patients is most often not associated with systemic relapse. Thelikelihood of local failure in a moderate risk patient who received neoadjuvant therapy is only 3.2%. Local failurein high risk patients is almost always associated with systemic relapse.
Tödlicher Zeckenschutz Zecken sind ein besonders unangenehmes Mitbringsel vonStreifzügen unsere Haustiere. Die Spinnentiere übertragenKrankheiten, die für Mensch und Tier gefährlich sind. UmHund und Katze vor Zecken zu schützen, gibt es speziel eTropfen. Doch beim Gebrauch der Mittel ist höchste Vorsicht geboten . Für Hunde vorgesehene Zeckenmittel können für Katzen tödlic
FLOMAX – IMPORTANT - BE AWARE! Information compiled by Charles (Chuck) Maack – Prostate Cancer Advocate Wichita, Kansas Chapter, Us TOO, Intl., Inc. Prostate Cancer Education and Support Network Many men dealing with prostate cancer or Benign Prostatic Hyperplasia (BPH) - and in this case continence/incontinence issues - are prescribed the alpha blocker Flomax (tamsulosin hydrochlor
 board approved 103Pd dose escalation study, and received 3months of hormonal therapy before implant and continuedandrogen withdrawal therapy for 6 months after implant(total 9 months). Patients on the institutional review boardprotocol also received a higher dose of external beam irradi-ation to 5,940 and 7,040 cGy. and the implant dose was alsoescalated from 56 to 76 to 86 Gy. as part of this protocol.
board approved 103Pd dose escalation study, and received 3months of hormonal therapy before implant and continuedandrogen withdrawal therapy for 6 months after implant(total 9 months). Patients on the institutional review boardprotocol also received a higher dose of external beam irradi-ation to 5,940 and 7,040 cGy. and the implant dose was alsoescalated from 56 to 76 to 86 Gy. as part of this protocol.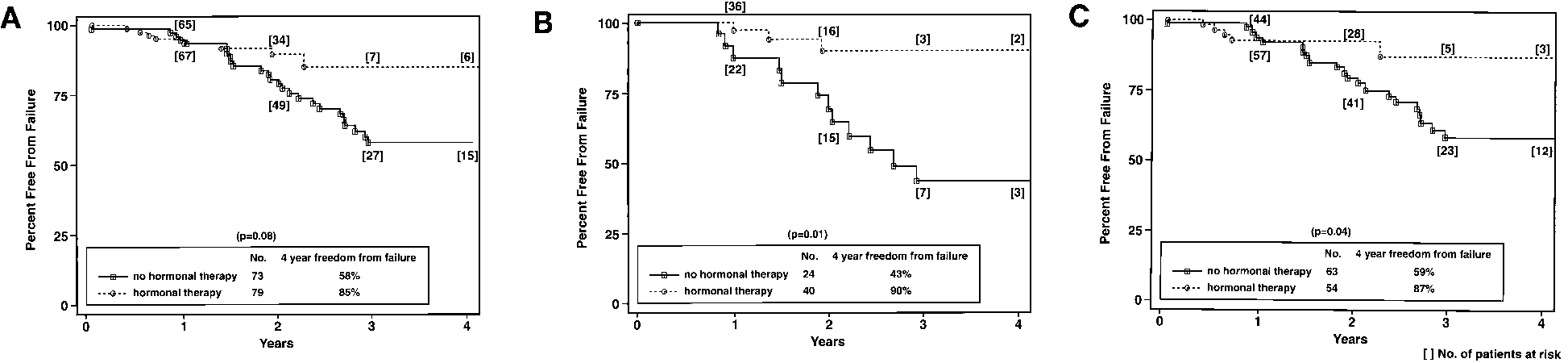
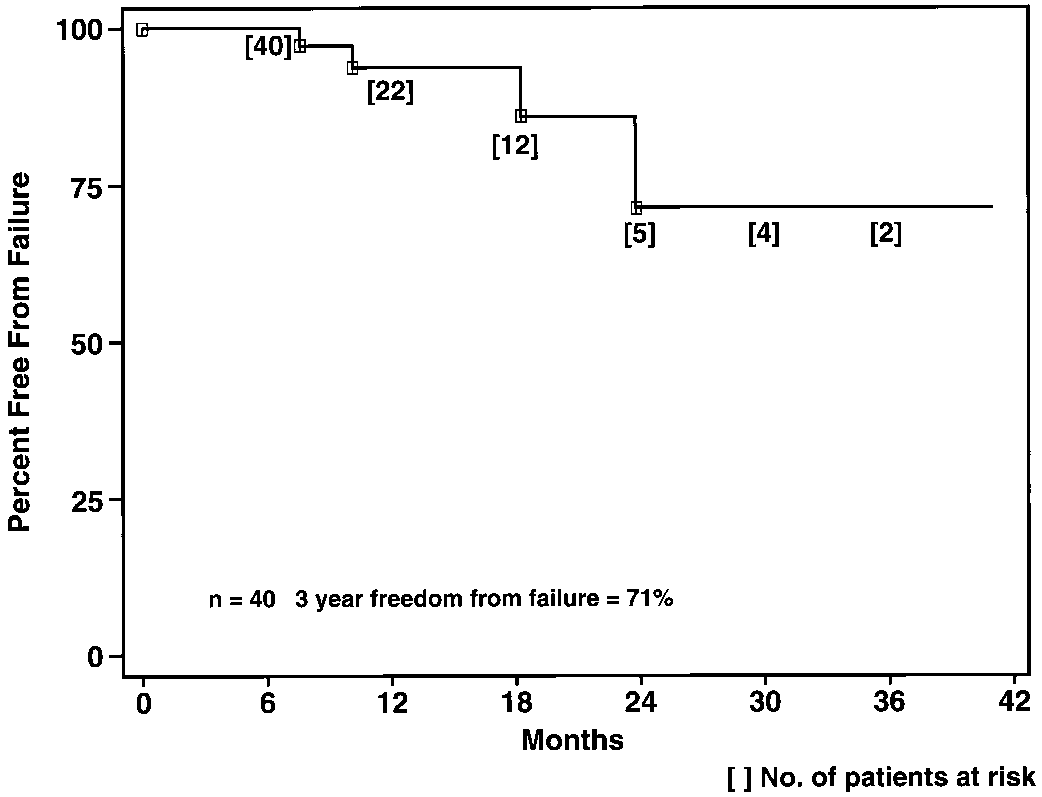 FIG. 2. Effect of hormonal therapy on PSA failure. Four-year biochemical freedom from failure for moderate risk patients treated with or
without hormones (p ϭ 0.08, A), with Gleason 7 or greater (p ϭ 0.01, B) and with PSA 10 ng./ml. or greater (p ϭ 0.04, C).
FIG. 2. Effect of hormonal therapy on PSA failure. Four-year biochemical freedom from failure for moderate risk patients treated with or
without hormones (p ϭ 0.08, A), with Gleason 7 or greater (p ϭ 0.01, B) and with PSA 10 ng./ml. or greater (p ϭ 0.04, C).