The Central Hospital GASTROSCOPY REPORT Stephen Rainey 1234567890 21/11/1958
Case note No: X123456 Procedure date Hospital: Referring Cons: Dr Merrick Indications Consultant/Endoscopist
Abdominal pain, haematemesis and raised WCC.
Nurses: S/N Jane Minkle & Sr Erin Kalidar
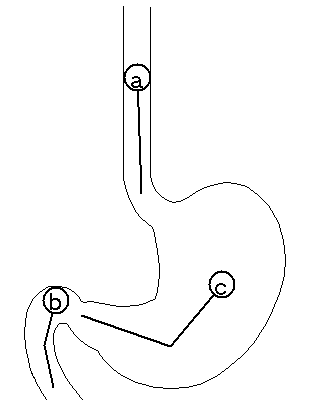
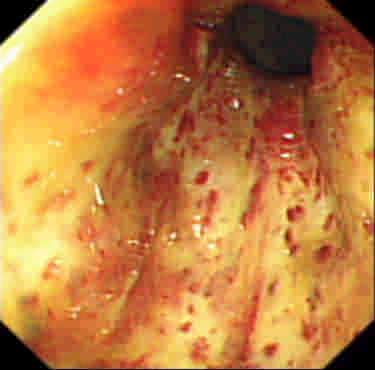
OESOPHAGUS. Moderate candida suspected at (a). STOMACH. Gastritis: severe erythematous/exudative with no bleeding, severe
Instrument
raised erosive with no bleeding and severe haemorrhagic with recent bleeding
at (c). DUODENUM. Duodenitis: severe and oedematous associated with erosions
Premedication Diagnoses OESOPHAGUS. Candida and oesophagitis/other. STOMACH. Gastritis. DUODENUM. Duodenitis. Medication Fluconazole 50 mg oral o.d. for 1 week and Pantoprazole 40 mg (iv) b.d. for 6 weeks was prescribed. Follow up Return to the ward. Awaiting histopathology results. middle oesophagus to the loweroesophagus (photographed)
b: An area extending from the bulbmiddle body to the pylorus(photographed)Specimens taken
Biopsy (x1 site a, x2 site b and x2 site c)
The Central Hospital
Site a: An area extending from the middle
Site b: An area extending from the bulb to the
Duodenitis: severe and oedematous associated with erosions and nodularity.
Site c: An area extending from the middle body to the pylorusGastritis: severe erythematous/exudative with no bleeding, severe raised erosive with no bleeding and severe haemorrhagic with recent bleeding. HISTOLOGY 3rd January 2003 Container ID Specimens 1 oesophageal biopsy from (a) Unisoft Medical Systems First Floor 2 upper duodenal biopsies from (b) 7 London Road Enfield 2 gastric biopsies from (c) DoB (Age) 21st November 1958 (44 years) NHS Inpatient (B7)
Indications. Abdominal pain, haematemesis and
Dr Merrick (General Medicine)
OESOPHAGUS. Moderate candida suspected at (a).
erythematous/exudative with no bleeding, severe
raised erosive with no bleeding and severe
haemorrhagic with recent bleeding at (c).
DUODENUM. Duodenitis: severe and oedematous
associated with erosions and nodularity at (b). the bulb to the third part(photographed)
Diagnoses. OESOPHAGUS. Candida and oesophagitis/other.
Produced by Unisoft's GI Reporting Tool. Call 0208-367 2103 if modifications to this form/layout are required. The Central Hospital ERCP REPORT Stephen Rainey 1234567890 21/11/1958
Case note No: X123456 Procedure date Hospital: Referring Cons: Dr Merrick Indications Consultant/Endoscopist
Abnormal enzymes and jaundice.Ultrasound imaging
Nurses: Sr Siobhan Rae & Sr Erin Kalidar
Report Cannulation via the major papilla to the bile duct was successful using Instrument
a sphincterotome, and to the pancreatic duct was not attempted.
Visualisation: The whole biliary system except the gall bladder, but not the pancreatic system. Contrast media used: hepatobiliary; full
Premedication
strength contrast and half strength contrast.
PAPILLA. Major: no previous surgery at (a).
BILIARY. Stricture: irregular and with upstream dilatation at (b).
Using the duodenoscope the following upper tract observations were noted. STOMACH. Gastric ulcer: early healing (regenerative mucosa evident) in the greater curve prepyloric region. Diagnosis AMPULLA. Normal. BILIARY. Extrahepatic: stricture: probably malignant. Therapeutic procedures Papillotomy: using bow string, with no bleeding. (site a) Stent insertion: one straight (length 12 cm, diameter 10 Fr) (b) Follow up Advice/comments Suggest spiral CT to look for mass lesion The Central Hospital COLONOSCOPY REPORT Stephen Rainey 1234567890 21/11/1958
Case note No: X123456 Procedure date Hospital: Referring Cons: Dr Merrick Indications Consultant/Endoscopist
Following up a transverse colectomy within the last
Nurses: S/N Jane Minkle & Sr Siobhan Rae
Bowel preparation with two sachets of Picolax was good. The colonoscope was inserted via the anus to the caecum. The
Instrument
caecum was identified positively by transillumination and the
tri-radiate caecal fold. Calibre: post operative stricture (length 5cm) at (b). Lesions: 1
Premedication
pedunculated polyp (10mm) excised, retrieved and sent to labs from
(a). The rest of the examination to the point of insertion was normal. Diagnoses Colonic polyps and post operative stricture. Therapeutic procedures Polypectomy: 1 excised (site a) Balloon dilatation (b) Follow up Awaiting histopathology results. Further colonoscopy in 3 months.
a: Distal descendingb: An area extending from the proximaldescending through the anastomosis tothe proximal ascendingSpecimens taken HISTOLOGY 3rd January 2003 Container ID Specimens 1 colonic pedunculated polyp from (a) Unisoft Medical Systems First Floor 7 London Road
Indications. Following up a transverse colectomy
within the last month. Previous carcinoma. DoB (Age) 21st November 1958 (44 years) NHS Inpatient (B7)
Calibre: post operative stricture (length 5cm) at (b).
Lesions: 1 pedunculated polyp (10mm) excised,
Dr Merrick (General Medicine)
retrieved and sent to labs from (a). The rest of the examination to the point of insertion
Diagnoses. colonic polyps and post operative
proximal descending throughthe anastomosis to theproximal ascending
Produced by Unisoft's GI Reporting Tool. Call 0208-367 2103 if modifications to this form/layout are required.
BP Lam et al. Treatment regimens for non-alcoholic fatty liver disease Annals of Hepatology 2009; 8(1): Supplement: S51-S59 Treatment regimens for non-alcoholic fatty liver disease Abstract Introduction, epidemiology, and natural history With the growing epidemic of obesity and diabetes, Since first described by Ludwig in 1980, non-alcoholic more attention has been placed on meta
Chicago Family Asthma & Allergy, S.C. Aaron Donnell, M.D. and Kelly Newhall, M.D. 2551 N Clark St, Suite 201, Chicago, IL 60614 773-388-2322, fax 773-388-2333 Thank you for coming to visit us! Here are some details about your first visit at CFAA… The visit for patient _______________________________________ is on the date of _______________ at time ______________. Our banner
 The Central Hospital
The Central Hospital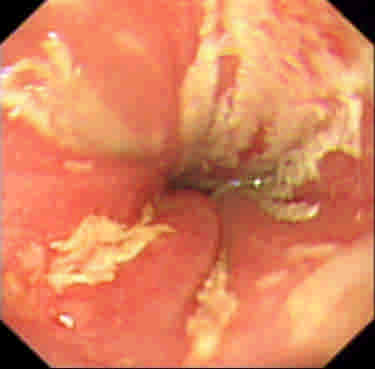

 The Central Hospital
The Central Hospital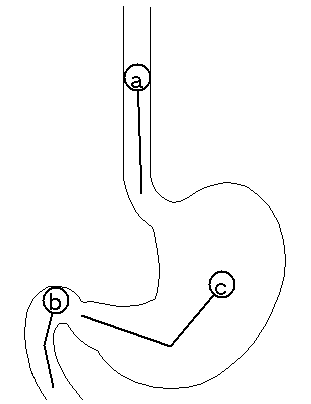 HISTOLOGY
HISTOLOGY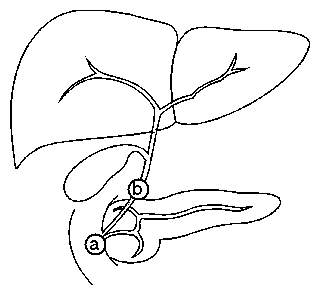 The Central Hospital
The Central Hospital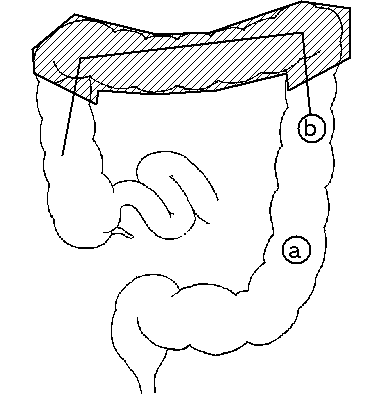 The Central Hospital
The Central Hospital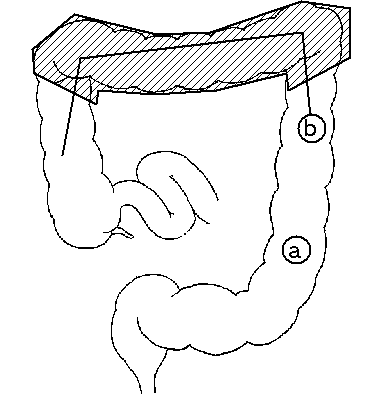 HISTOLOGY
HISTOLOGY