International Journal of Paediatric Dentistry 2006; 16: 174–180
Erosive effect of an antihistamine-containing syrup on primary enamel and its reduction by fluoride dentifrice
C. C. COSTA1, I. C. S. ALMEIDA1 & L. C. COSTA FILHO1Santa Catarina Federal University, Florianópolis, Brazil and 2Pontificial Catholic University of Rio Grande do Sul, Porto Summary. Aim. This study evaluated the action of an antihistamine-containing syrup (Claritin D) on enamel that was subsequently submitted or not to applications of fluoride dentifrice. Methods. Two hundred sixty-four slices (n = 44 per subgroup) prepared from exfoliated primary molars were evaluated in
hardness tests. Six subgroups were submitted to different treatments for 10 days. The controls underwent pH cycling
with (positive control) or without (negative control) three daily immersions in fluoride dentifrice/distilled water slurry.
The test subgroups related to daytime use of the antihistamine syrup underwent pH cycling and two 5-min applications
of Claritin D, coupled or not to the three daily immersions in the fluoride slurry. The subgroups related to nocturnal use
of the syrup were submitted to the same procedures of daytime subgroups, respectively, but with one of the applications of
Results. The median hardness values obtained after use of the syrup were significantly lower than the initial ones. Equivalent
values for subgroups submitted to fluoride applications in addition to treatment with the syrup were significantly higher. Conclusion. It was concluded that the antihistamine-containing syrup reduced the hardness of primary enamel and that,
in this experiment, the use of fluoride dentifrice was able to diminish this erosive effect.
chronic diseases. Antihistamine-containing medicines
Introduction
may be an example of a potentially erosive agent.
Dental caries is the most prevalent disease of the
Besides the acid components found in such
oral cavity and may affect individuals at any stage
medications, other factors such as high frequency of
of their lives. Nevertheless, tooth dissolution can
ingestion (two or more times a day), bedtime con-
also be caused by erosion, which is the mineral loss
sumption, high viscosity, and the collateral effect of
of dental tissue when its surface is exposed to acids
a reduction in salivary flow may contribute to the
or chelates, in a systematic manner and without
Many recommendations have been made in order
According to Linnett and Seow [2], the prevalence
to minimize tooth damage caused by the regular use
of dental erosion has increased especially among
of liquid medications. Among these is the use of the
children and adolescents. The aetiology has been
medication at meal times in order to avoid ingestion
related to the regular use of products with low
between them [4]. Oral hygiene or mouth rinsing
endogenous pH, high acidity, and absence or low
with water or chewing sugar-free gum after taking
concentrations of ions including those of calcium,
the medication have also been recommended [3], as
fluoride, and phosphate in their composition. Among
have the addition of calcium, fluoride, or phosphate
these products are medications that may be erosive
to formulations [3] and the use of topical fluoride
because they possess these characteristics, and which
may be of a particular risk when used for treatment of
Although the efficacy of fluoride in preventing
dental caries is widely accepted, the same is notevident in relation to erosion, as the ability of
Correspondence: C. C. Costa, Rua Gaspar Martins, 1882. Bairro
treatments with fluoride to prevent the loss of dental
Centro. Santa Maria, RS, Brazil. 97060-260. E-mail:[email protected]
tissue through erosion is still questioned [1,5]. Effect of antihistamine syrup and dentifrice on primary enamel
Unlike what occurs during the caries process, in
citric acid, calcium, and phosphate, were also
erosion the acid challenge is much stronger, and after
determined. Tests demonstrated that the medication
erosive mineral loss only a thin, partly demineral-
did not contain fluoride or phosphate; the percentage
ized and softened surface layer is left to provide
of citric acid was 0·0147% and of calcium,
a structure for remineralization. In addition, the
stability of the calcium fluoride under erosive con-ditions is still unknown, but it may be speculated
that this compound provides additional mineral tobe dissolved during an acid attack before the under-
Samples were obtained from 88 exfoliated primary
lying enamel is affected. Thus it may be hypothesized
molars cut longitudinally, in a mesio-distal direc-
that, in a similar way to its anticariogenic properties,
tion, in slices 2 mm thick. The dental sections were
fluoride may assist in strengthening hard tooth tissue
invested in polyester resin (FiberGlass Ind. & Com.
against acids and re-harden an eroded enamel surface
Ltda; Florianópolis, SC, Brazil) and, after polymer-
ization, were smoothed (abrasive papers of sizes
The aim of this in vitro research was to evaluate,
800, 1000, 1200, 1500 and 2000; 3M Ind. & Com.
through hardness tests, the action of Claritin D
Ltda; St Paul, MN, USA) and polished (Arotec Ind.
syrup (Schering-Plough; São Paulo, SP, Brazil) on
& Com. Ltda; São Paulo, SP, Brazil felt discs and
the enamel of primary molars and the effect, if any,
1 and 0·3 µm oxide aluminium suspension, South
of concomitant applications of fluoride dentifrice.
Bay Technology Inc.; San Clemente, CA, USA) ina water-cooled grinding machine (Panambra DP-10,Struers; São Paulo, SP, Brazil). After the polishing
procedure, samples were viewed under an optical
This experimental study evaluated, in vitro, the
microscope (Aus Jena, model 444181, with a 40×
hardness of 264 samples of primary enamel.
objective; Astro Optics Division, Montpelier, MD,
USA) in order to check that surfaces were flat, pol-
antihistamine-containing syrup, and fluoride denti-
ished, and without irregularities that could interfere
frice. The pH cycling simulated a low acid challenge
in relation to feeding [7], and the antihistamine-containing syrup was applied to sound primary enamel
in situations set up to represent its use during theday and at bedtime in order to investigate the action
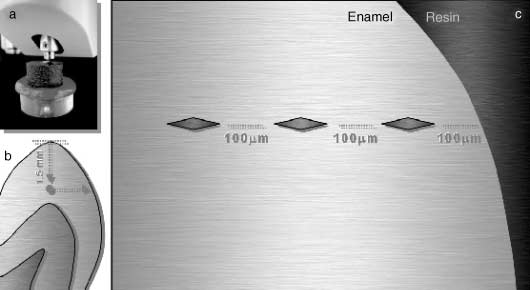
In order to make the indentations, the hardness
of fluoride dentifrice on different usage patterns.
tester (Shimadzu, model HMV – 2000; Nakagyou,Kyoto, Japan) was calibrated with a Knoop tip andload of 50 g was applied for 5 s. The initial inden-
tation was located in a standard position 1·5 mm
Claritin D syrup (Schering-Plough) was selected
below the cusp tip and 0·1 mm from the enamel
for this study because it is frequently used for
external surface. Three indentations, at the same
chronic conditions and has the characteristics of low
height, toward the dentin, spaced 100 µm from each
endogenous pH (pH 3·84 ± 0·04) and high acidity
other, were made and their average value was taken
(30·69 mL ± 1·98 mL of NaOH 0·1 N solution to
as equivalent to the hardness value of the specimen
neutralize 100 mL of the diluted medication). Pre-
liminary chemical analysis of the product was made
Following the initial hardness test, 264 dental
in triplicate using samples from three different
sections with an enamel hardness value between
batches. The pH was measured with a digital pH
272 and 440 Knoop hardness number (KHN) were
meter (MP 220 – Mettler Toledo; São Paulo, SP,
selected, as these were considered compatible with
Brazil) and the titrable acidity by the method AOAC
22·058, which determines the quantity of NaOH0·1 N solution necessary for the product to reach
neutral pH or pH above it (pH ≥ 7·0) [8].
Chemical parameters considered important in
Sections were next allocated into control and
Claritin D syrup, such as quantities of fluoride,
experimental groups and into six subgroups. Two
C. C. Costa, I. C. S. Almeida & L. C. Costa FilhoFig. 1. (a) Hardness tester with Knoop tip. (b) Drawing of the dental slice: initial position of the hardness tester tip and dislocation direction. (c) Enlargement of drawing b: from the external limit (in contact with the resin) there is a space of 100 µm among the indentations.
formed control groups (positive and negative) and
Two subgroups belonging to the experimental group
four were experimental groups representing daytime
were submitted to pH cycling and to antihistamine
medication, daytime medication + fluoride dentifrice,
syrup application, representing daily and daytime
nighttime medication, and nighttime medication +
use for 10 days (E1) or daily and nighttime use for
the same period of time (E3). The amount of syrup
Cycles of demineralization and remineralization
used for each sample was the equivalent of 0·25 mL
were based on the pH cycling proposed by Ten Cate
two times a day. In subgroup E1, the applications
and Duijsters [7] and modified by Featherstone et al.
lasted for 5 min each and in subgroup E3, one of
[10]. This cycling includes 10 cycles in which the
them lasted for 5 min and the other for 8 h.
samples are immersed daily, at 37 °C, for 3 h in the
To evaluate the topical effect of daily use of fluo-
demineralizing solution followed by 21 h in the rem-
ride dentifrice on the primary enamel that received
antihistamine syrup application, two subgroups were
Thus, each 1 mm2 of dental tissue was immersed
included in the experimental group. Each specimen
in 6·24 mL of demineralizing solution (acetate buffer
from subgroup E2 had the same treatment as subgroup
75 mm containing 2·0 mm of Ca and P at pH 4·3)
E1 added to the utilization of fluoride dentifrice/
and in 3·12 mL of remineralizing solution (Tris
distilled water slurry (1 min immersion in fluoride
buffer 0·1 m containing 1·5 mm Ca, 0·9 mm P, and
dentifrice/distilled water slurry three times a day).
150 mm KCl at pH 7·0). Because this cycling
The samples from subgroup E4 underwent the
was carried out for 14 days and involved 10 cycles
same procedures as subgroup E3 plus use of the
of pH, after the fifth day the samples were stored
in remineralizing solution for 48 h, after which both
Strategies of treatment for each subgroup, over a
solutions were changed for a new cycle of 5 days
period of 24 h, are summarized below.
C1 (negative control subgroup): demineralizing
The samples from the control group were sub-
solution for 1 h + remineralizing solution for 4 h +
mitted only to pH cycling (negative control – C1) or
to pH cycling added to immersion in slurry of fluo-
solution for 6 h + demineralizing solution for 1 h +
ride dentifrice (Tandy, Kolynos-Brazil, silex-based
gel with 1·1 mg /g F in NaF form) and distilled water
C2 (positive control subgroup): demineralizing
(proportion 1 : 3) that presented 0·948 mg /g of flu-
solution for 1 h + fluoride dentifrice/distilled water
oride and pH of 7·2 (positive control – C2). The
slurry for 1 min + remineralizing solution for 4 h +
specimens were immersed in the slurry of fluoride
demineralizing solution for 1 h + fluoride dentifrice/
dentifrice and distilled water, 0·625 mL/mm2, for
1 min on three occasions, in order to simulate the
solution for 6 h + demineralizing solution for 1 h +
topical action exerted by the fluoride during tooth
fluoride dentifrice/distilled water slurry for 1 min +
Effect of antihistamine syrup and dentifrice on primary enamel
E1 (experimental subgroup simulating daily and
indentations were firstly located in carry out the
daytime use of medication): demineralizing solution
for 1 h + remineralizing solution for 2 h + applicationof medication for 5 min + remineralizing solution for
2 h + demineralizing solution for 1 h + remineralizingsolution for 6 h + demineralizing solution for 1 h
The software sas system 8·02 for Windows (SAS
+ remineralizing solution for 2 h + application of
Institute Inc. – Cary, NC, USA) was used for the
medication for 5 min + remineralizing solution for 9 h.
statistical analysis, using analysis of variance with
E2 (experimental subgroup simulating daily and
mixed models. To analyse hardness before and after
daytime use of medication and of fluoride denti-
the specific treatments, two mixed models were
made in which the dependent variable was initial
dentifrice/distilled water slurry for 1 min + reminer-
and final hardness, respectively, and the fixed effects
alizing solution for 2 h + application of medication
(explanatory variables) were subgroup and indenta-
for 5 min + remineralizing solution for 2 h +
tion number (which represent enamel depth),
demineralizing solution for 1 h + fluoride dentifrice/
whereas the random effect was the sample number.
After the treatments, the initial hardness was used
solution for 6 h + demineralizing solution for 1 h
as a co-variable in the final hardness model to increase
+ remineralizing solution for 2 h + application of
statistical power and to better adjust the model. A
medication for 5 min + fluoride dentifrice/distilled
third mixed model was made, keeping the same
water slurry for 1 min + remineralizing solution for 9 h.
fixed and random effects, but considering the per-
E3 (experimental subgroup simulating daily and
centual reduction in hardness as the dependent
nighttime use of medication): demineralizing solu-
The covariance structure used was the variance com-
application of medication for 5 min + remineralizing
ponents, and the method to estimate the differences
solution for 2 h + demineralizing solution for 1 h +
among subgroups and indentations was the Tukey–
Kramer with significance level of 1% (P < 0·01).
solution for 1 h + remineralizing solution for 2 h +application of medication for 8 h + remineralizing
E4 (experimental subgroup simulating daily and
Pre-treatment hardness values among the six sub-
nighttime use of medication and of fluoride denti-
groups did not show a statistically significant differ-
ence (P = 0·3687). All mean values were greater
dentifrice/distilled water slurry for 1 min + reminer-
alizing solution for 2 h + application of medication for
The mean hardness values obtained for the six
5 min + remineralizing solution for 2 h + demineraliz-
subgroups after the different treatments were all sig-
ing solution for 1 h + fluoride dentifrice/distilled
nificantly lower than equivalent pretreatment values
water slurry for 1 min + remineralizing solution
(P < 0·001) (Table 1 and Fig. 2), demonstrating that
for 6 h + demineralizing solution for 1 h + fluoride
there had been loss of hardness in all subgroups.
dentifrice/distilled water slurry for 1 min + reminer-
In subgroup C1 (pH cycling), there was a decrease
alizing solution for 2 h + application of medication
in hardness of 20·28% and the mean of post-
for 8 h + remineralizing solution for 1 h.
treatment values was 266·16 KHN. In subgroup C2(pH cycling and fluoride application), the decreasein hardness was only 5·31% and the mean hardness
after treatment was still compatible with sound
Identifications marks on the samples were covered
with adhesives and were mixed for blind estimations
Subgroup E1 (pH cycling and daytime medication
use) showed a decrease of 46·83% in enamel hard-
The final hardness analysis was performed by the
ness and mean hardness after treatment (179·29
same examiner in exactly the same way as the initial
KHN) was considered representative of demineral-
assessment, using the same instrument, number of
ized human enamel. In subgroup E2 (same treatment
indentations, load, and application time. The initial
as E1 added to fluoride application), the decrease in
C. C. Costa, I. C. S. Almeida & L. C. Costa FilhoTable 1. Mean values in KHN and hardness variation after treatments in the six subgroups.
Equal superscripts indicated statistical equivalence (P > 0·36). Different superscripts indicated statistical difference (P < 0·0001). The values in parentheses indicated the confidence intervals of 95% of the means estimated by the three mixed models.
Among these properties are: low endogenous pH[12], high titrable acidity [12], presence of citricacid [13], absence of fluoride and phosphate, andminimal quantity of calcium in its composition [14].
It is common knowledge that the chemistry of
enamel changes from its surface to interior and thiswas evident in the present study, because the inter-nal indentations had lower hardness values than didthe external ones. As the mixed model statisticincorporated the coverable indentation depth andthere was no interaction with the different treat-ments, showing that enamel reaction was uniformdespite its depth and suggesting that it was unlikely
Fig. 2. Mean Knoop hardness values for the six subgroups before
to have acted as a confounder. Thus, investigations
using surface tissue may be directly compared tothis research.
hardness was lower, at 14·59%, and the post-treatment
Subgroup C1 had a substantial loss of mineral,
indicating that the immersion of enamel in a rem-
The subgroup E3 (pH cycling and nighttime med-
ineralizing solution, with a composition similar to
ication use) showed the greatest decrease in enamel
human saliva, for 21 h daily, was not enough to
hardness, at 89·14%, and the final hardness value
prevent the demineralization caused by three acid
was only 36·32 KHN. In subgroup E4 (same treat-
attacks. These findings corroborated the study of
ment as E3 added to fluoride application), the hard-
Eisenburger et al. [15] in which artificial saliva was
ness decrease was also high, 84·49%, and final
not able to restore the superficial hardness or mor-
hardness value was 51·75 KHN (Table 1 and Fig. 2).
phology of the eroded dental samples. The results
Among the mean values for hardness obtained
of subgroup C2 supported the findings of studies
after the different treatments, statistically significant
[16,17] in which the enamel specimens treated with
differences (P < 0·001) were detected among the six
dentifrice containing sodium fluoride showed an
subgroups (Table 1). Values for subgroups submitted
increase in hardness, indicating remineralization.
to fluoride application were significantly greater
All subgroups where treatment utilized antihista-
than were values for subgroups that did not have
mine-containing syrup showed statistically signifi-
cant decreases in hardness values when compared to
control subgroups. This was irrespective of patternof treatment.
Considering subgroup E1, it can be suggested
Discussion
that five daily acid challenges were able to cause
Claritin D syrup (Schering-Plough) presents charac-
considerable enamel demineralization. In subgroup
teristics that may well provide erosive potential.
E3, it was demonstrated that prolonged exposure
Effect of antihistamine syrup and dentifrice on primary enamel
of primary enamel to an acid medication caused an
frice is able to diminish erosion in vitro, it seems
extremely aggressive demineralization that resulted
likely to do the same in vivo. In addition, if more
in a reduction of the final hardness mean almost
concentrated fluoride agents could be used simulta-
five times greater than did shorter exposure to the
neously, even better protection of dental tissues
same product. The increase in exposure time to acid
would be assured and, possibly, erosion would be
products that worsened the occurrence of erosion
has also been described by Hunter et al. [18].
It was possible to conclude that the final hardness
Results for the subgroups submitted to medication
values for subgroups that received application of
and fluoride applications (E2 and E4) showed that
Claritin D syrup (E1 and E3) were significantly
fluoride is capable of reducing the erosive effect of
lower than values in the control subgroup (C1). This
an acid product, because it provides enamel protec-
difference was reduced by the fluoride dentifrice/
tion in relation to its hardness. Similar findings were
distilled water slurry, because the subgroups submit-
demonstrated in the studies with dentifrice [19],
ted to topical fluoride treatment (C2, E2, and E4)
varnish [4], gel, and fluoride solution [20], which
presented final hardness values that were signifi-
have led to the conclusion that different forms of
cantly greater than those of homologue subgroups
fluoridation are able to minimize enamel and dentin
without fluoride treatment (C1, E1, and E3).
The results of subgroup E4 showed that the
What this paper adds
presence of fluoride was not enough to prevent an
• This paper adds information that an acid medication can
accentuated demineralization because of prolonged
reduce deciduous enamel hardness, especially when in
acid challenge and that, perhaps, the application of
contact with this tissue for a prolonged period of timeand without the presence of fluoride in the environment.
additional fluoride in solutions, gels, or varnishes,as suggested by some authors [20], may be
Why this paper is important for paediatric dentists
employed in order to protect dental tissues in an
• Paediatric dentists must be aware of the potential
demineralization an acid medication can bring to
deciduous enamel and also should have in mind that a
Many researches have indicated that the action of
fluoride toothpaste can attenuate this harmful effect.
topical fluoride in dental erosion prevention is ques-tionable [5,21] or that this ion only provides a pre-ventive effect when applied in high concentrations[4,20]. Results of this study are contrary to these
References
findings, since the fluoride dentifrice/distilled waterslurry was able to reduce the erosive process.
1 Ten Cate JM. What dental diseases are we facing in the new
In considering results, the difficulty in reproduc-
millennium: some aspects of research agenda. Caries Research 2001; 35: 2–5.
ing the clinical situation in in vitro studies must be
2 Linnett V, Seow WK. Dental erosion in children: a literature
borne in mind. This is due to the complexity of the
review. Pediatric Dentistry 2001; 23: 37–43.
oral environment. Because of that, this research
3 McDonald JL, Stookey GK. Laboratory studies concerning
may have overestimated the occurrence of erosive
the effect of acid-containing beverages on enamel dissolutionand experimental dental caries. Journal of Dental Research
demineralization because of the absence of salivary
1973; 52: 211–216.
pellicle, which may be protective, the absence of
4 Sorvari R, Meurman JH, Alakuijala P, Frank RM. Effect of
buffering by saliva, and to its direct contact with the
fluoride varnish and solution on enamel erosion in vitro. Caries
teeth [22,23]. Salivary pellicle is important for
Research 1994; 28: 227–232.
5 Larsen MJ. Prevention by means of fluoride of enamel erosion
protection of enamel because some kinds of pellicle
as caused by soft drinks and orange juice. Caries Research
proteins are tenacious even at low pH and may
2001; 35: 229–234.
function as a barrier to acid attack [22]. Similar
6 Rolla G, Ogaard B, Cruz RA. Clinical effect and mechanism
situations may occur in the oral cavity with respect
of cariostatic action of fluoride-containing toothpastes: a review. International Dental Journal 1991; 41: 171–174.
to saliva, since use of medications, such as anti-
7 Ten Cate JM, Duijsters PPE. Alternating demineralization and
histamines, may reduce salivary flow. This is also the
remineralization of artificial enamel lesions. Caries Research
case during nocturnal administration, when salivary
1982; 16: 201–210.
flow is naturally reduced. Because of this, use of
8 Association of Official Analytical Chemist. Official Methodsof Analysis, 16th edn. St. Louis, MO: Mosby, 1984.
fluoride is especially important to reduce damage
9 Meredith N, Scherriff M, Setchell DJ, Swanson SA. Meas-
caused by the erosive process. If the fluoride denti-
urement of the microhardness and Young’s modulus of human
C. C. Costa, I. C. S. Almeida & L. C. Costa Filho
enamel and dentine using an indentation technique. Archives
analysis of fluoride dentifrice effects on lesion progression
of Oral Biology 1996; 41: 539–545. in vitro. Caries Research 1987; 21: 502–512.
10 Featherstone JDB, O’Reilly MM, Shariati M, Brugler S.
17 White DJ. Reactivity of fluoride dentifrices with artificial
Enhancement of remineralization in vitro and in vivo. In:
caries. II. Effects on subsurface lesions – F uptake, F distri-
Leach SA (ed.). Factors Relating to Demineralization and
bution, surface hardening and remineralization. Caries ResearchRemineralization of the Teeth. Oxford: ERL, 1986: 23–34.
1988; 22: 27–36.
11 Duke SA, Forward GC. The conditions occurring in vivo
18 Hunter ML, West NX, Hughes JA, Newcombe RG, Addy M.
when brushing with toothpastes. British Dental Journal 1982;
Erosion of deciduous and permanent dental hard tissue in the
152: 52–54.
oral environment. Journal of Dentistry 2000; 28: 257–263.
12 Edwards M, Creanor SL, Foye RH, Gilmour WH. Buffering
19 Clark JW, Corpron RE, More FG, Easton JW, Merril DF,
capacities of soft drinks: the potential influence on dental
Kowalsi CJ. Comparison of the effects of two topical fluoride
erosion. Journal of Oral Rehabilitation 1999; 26: 923 –927.
regimens on demineralized enamel in vivo. Journal of Dental
13 Meurman JH, Harkonen M, Naveri H, et al. Experimental
Research 1988; 67: 954 –958.
sports drink with minimal dental erosion effect. Scandinavian
20 Tezel H, Ergucu Z, Onal B. Effects of topical fluoride agents
Journal of Dental Research 1990; 98: 120–128.
on artificial enamel lesion formation in vitro. Quintessence
14 Grenby TH. Lessening dental erosive potential by product
International 2002; 33: 347–352.
modification. European Journal of Oral Sciences 1996; 104:
21 Larsen MJ, Richards A. Fluoride is unable to reduce dental
erosion from soft drinks. Caries Research 2002; 36: 75–80.
15 Eisenburger M, Addy M, Hughes JA, Shellis RP. Effect of
22 Hanning M, Balz M. Influence of vivo formed salivary pel-
time on the remineralization of enamel by synthetic saliva
licle on enamel erosion. Caries Research 1999; 33: 372–379.
after citric acid erosion. Caries Research 2001; 35: 211–
23 Nekrashevych Y, Stosser L. Protective influence of experi-
mentally formed salivary pellicle on enamel erosion. An in
16 White DJ, Featherstone JD. A longitudinal microhardness
vitro study. Caries Research 2003; 37: 225 –231.
Preparing for Winter: Q&A This Q&A comes from an email to bee-commerce from a customer. The questions were so astute and had such strong bearing on all beekeepers, that they are repeated here for everyone's benefit. Hats off to a smart beekeeper! The answers from bee-commerce are in BLUE CAPS: Q: Sugar water mix with Fumidil and Terramycin - every time I mix up a batch of sugar wate
CRUK CI Annual International Symposium 2013Ralph DeBerardinisChildren’s Medical Center Research Institute at UT SouthwesternIntroduction of the Chair by Kevin BrindleRalph DeBerardinisUT SouthwesternCancer metabolism – basic biology and translational approachesJohn GriffithsCancer Research UK Cambridge InstituteImaging metabolism: Carbonic anhydrase IX acts as the tumour extracellular pH a
 C. C. Costa, I. C. S. Almeida & L. C. Costa Filho
Fig. 1. (a) Hardness tester with Knoop
C. C. Costa, I. C. S. Almeida & L. C. Costa Filho
Fig. 1. (a) Hardness tester with Knoop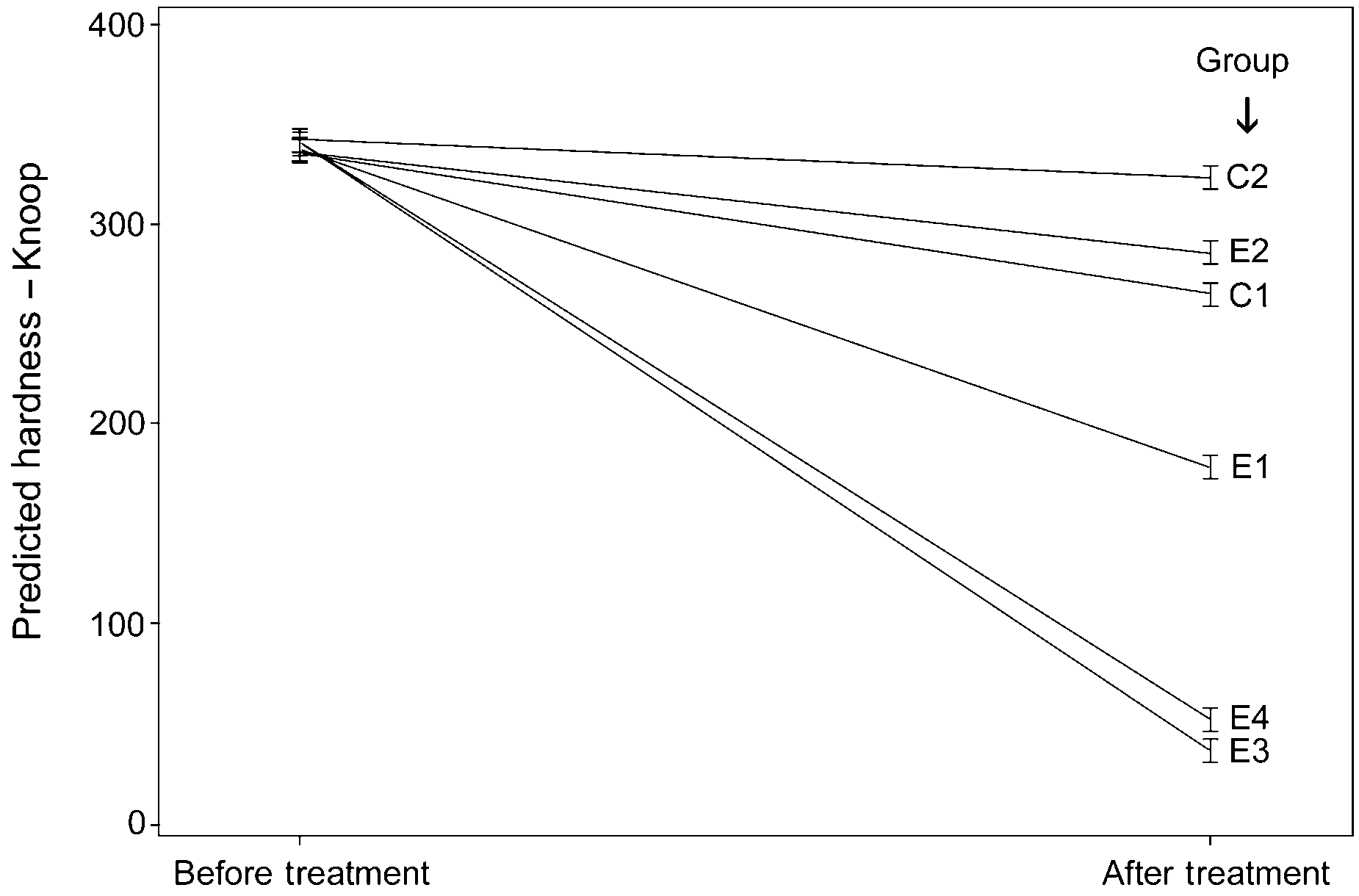 C. C. Costa, I. C. S. Almeida & L. C. Costa Filho
Table 1. Mean values in KHN and hardness variation after treatments in the six subgroups.
C. C. Costa, I. C. S. Almeida & L. C. Costa Filho
Table 1. Mean values in KHN and hardness variation after treatments in the six subgroups.