J Pediatr Adolesc Gynecol (2006) 19:173–179
Usefulness of Monitoring Fertility from Menarche
Pilar Vigil, MD, PhDFrancisco Ceric, Manuel E. Corte´sand Hanna Klaus, 1Unit of Reproduction and Development, Faculty of Biological Sciences, Pontifical Catholic University of Chile, Santiago, Chile;2Fundacio´n Me´dica San Cristo´bal, Santiago, Chile; 3School of Psychology, Faculty of Social Sciences, Pontifical Catholic Universityof Chile, Av. Vicun˜a Mackenna 4860, Santiago, Chile; 4TeenSTAR Program, Natural Family Planning Center of Washington, D.C. 8514 Bradmoor Drive, Bethesda, MD 20817-3810, USA
The concept of the ovarian cycle as a contin-
environmental conditions in order to ensure the health
uum considers that all types of ovarian activity encountered
of the mother and child. The ovarian continuum be-
during the reproductive life are responses to different envi-
gins at fertilization, when the zygote starts its devel-
ronmental conditions in order to ensure the health of the
opment. Approximately 2 months after fertilization
woman. During the normal ovulatory cycle, a series of se-
occurs, the future oogonia, called primordial germ
quential events have to occur in a highly synchronized man-
cells at this moment, leave the embryo and migrate
ner. Fertility awareness is useful in helping women toidentify the different stages of their reproductive life cycle.
to the vitelline sac in order to escape the process of
Fertility awareness is also a valuable tool in helping women
cell differentiation. Some four weeks later these cells
to identify gynecological disorders. Persistence of irregular-
migrate to the region of the future ovary, the gonadal
ities within the mucus patterns and the menstrual cycle
crest, and start their process of differentiation, form-
should be of concern to women presenting with these prob-
ing millions of primordial follicles. At this time some
lems. These irregularities may be due to obstetrical, endo-
7 million primordial follicles are formed, most of
crine, gynecological or iatrogenic disorders. Insight into
which will undergo atresia. When the girl is born, 1
early pregnancy complications, ovulatory dysfunction and
to 2 million follicles containing the oocytes remain.
pelvic inflammatory disease can be ascertained from abnor-
Of these, about 475 will complete folliculogenesis
malities within the menstrual cycle and mucus pattern.
Thus, fertility awareness will also enable the recognition
Puberty, viewed from the perspective of reproduc-
and early treatment of several metabolic, endocrine and
tion, could be considered as the process by which hor-
monal changes take place in order to permit theexpulsion from the ovary of mature oocytes, thus al-
lowing fertilization to take place. The luteinizing hor-
mone (LH) peak must follow the estrogen peak for
ovulation to occur,but there are a series of sequentialevents that must occur in a highly synchronized man-ner. During the first 2 years after menarche, occa-
sional anovulatory cycles may occur. However,subsequently, a healthy ovary will exhibit regular
Fertility is a transient biological state that depends on
monthly ovulations, characterized by a 25 to 36 day
the fertility potential of the couple. During a woman’s
cyclThe ovulatory cycles are normally only inter-
lifetime, the ovary will go through different states of
rupted by pregnancies and breastfeeding. Normal ovu-
hormonal secretion and ovulation. The concept of
latory activity and fertility are restored following
the ovarian cycle as a continuum considers that all
pregnancy and lactation; however, stress or excessive
types of ovarian activity encountered during the re-
exercise may result in chronic ovulatory dysfunction
productive life are normal responses to different
which requires therapy. Abnormality in cycles suchas anovulation or short luteal phases frequently occursas menopause approaches. This is an expected part of
Address correspondence to: Pilar Vigil, MD, PhD, Unit of Repro-
a woman’s reproductive life cycle.
duction and Development, Faculty of Biological Sciences, Ponti-fical Catholic University of Chile, Av. Alameda O’Higgins 340,
With the use of instruments such as the ovarian
monitor, which measures the urinary excretion of
Ó 2006 North American Society for Pediatric and Adolescent Gynecology
Vigil et al: Usefulness of Monitoring Fertility from Menarche
estrone glucuronide (E1G) and pregnanediol glucuro-
(14) Throughout the cycle the hypothalamus con-
nide (PdG), important metabolites of the two ovarian
tinues to produce gonadotropin-releasing hor-
hormones, estradiol and progesterone, it has been pos-
mone (GnRH) and secretes it continuously in
sible to identify hormonal variations during different
periods of a woman’s life and to correlate these
Throughout life, the ovarian continuum may present
different phases as documented by studies carriedout with the ovarian monitor
(1) Rising follicle-stimulating hormone (FSH)
levels that cause follicular recruitment.
Throughout a woman’s life, the ovarian continuum
(2) Follicular development that causes an increase
may present different phases or patterns depending
on the presence or absence of ovulation. One pattern
(3) Increasing estradiol levels, secreted by matur-
is characterized by an anovulatory ovarian activity;
ing follicles, cause endometrium proliferation
this type can be observed in two situations. The first
and an increase in the amount of mucus se-
type of anovulatory ovarian activity occurs when the
creted by the cervical epithelium as well as
FSH levels pass the threshold and stimulate a follicle
change in the type of the mucus and the degree
to develop, but sufficient LH is not released or the re-
sulting ovulatory mechanism does not operate. This is
an important cause of long cycles. A second type is
(5) Estrogen together with inhibin shuts off FSH
when the FSH levels rise above threshold, but not suf-
ficiently to boost one follicle into dominance. A
chronic situation develops in which follicles continue
(6) Estrogen secreted by the dominant follicle
to grow and regress causing the estrogen levels to pla-
feeds back negatively on the hypothalamo- pi-
teau. The effect of the raised but constant estrogen
production is to develop an unstable endometrium that
(7) The pituitary LH rises to LH peak and luteini-
zation of the follicle is initiated. The ovum is
Another different pattern of the continuum occurs
released from the follicle (the ovum has a lim-
when the estrogen levels rise to a peak resembling
a preovulatory peak. LH is released but not in suffi-
(8) With the initiation of follicular luteinization,
cient amounts to cause the follicle to rupture and ovu-
secretion of progesterone commences in the
late. However, it is sufficient to cause a small amount
follicle. This initial rise in progesterone main-
of luteinization of the follicle with resultant low level
(9) This pattern of LH secretion aids the formation
The ovarian continuum may also present as a defi-
of a normal corpus luteum and an adequate
cient luteal phase. A cycle that presents a deficient lu-
luteal phase of the menstrual cycle.
teal phase is one in which ovulation occurs, but the
(10) The corpus luteum produces progesterone and
conditions during the luteal phase do not support an
ongoing pregnancy. Thus, any cycle in which the pro-
(11) Progesterone changes the endometrium to the
gesterone levels fail to reach 10 mmole PdG/24 hours
secretory type. It also affects the cervical mu-
7 days after ovulation has occurred or any cycle with
cus, converting it from estrogenic to progesta-
a luteal phase length of 10 days or less could be
tional type, which is not suitable for sperm
regarded as ‘‘deficient.’Ovulation is always
transport through the cervix. If fertilization
has not occurred, the corpus luteum begins to
endometrium capable of responding to the hormones
is present and there is no human chorionic gonadotro-
(12) Estrogen and progesterone levels return to
early follicular phase levels approximately 14
Even in fertile ovulatory cycles the potential for
days after the initial formation of the corpus
conception varies with the timing of insemination,
the groups of women studied, and the fertility poten-
(13) This drop in sex hormone levels releases the
tial of the male partner. Age also is an important fac-
suppression of FSH and LH and a new cycle
tor to consider when analyzing fertility potential, as
Vigil et al: Usefulness of Monitoring Fertility from Menarche
Cervical Mucus as a Determinant for Fertility
‘‘peak day.’The woman who understands herown mucus pattern should be able to recognize
It has been shown that mucus quality is a better predic-
changes in the normal ovulatory pattern and detect
tor of the possibility for conception than ovulation.
changes which may indicate a number of gynecolog-
Mucins are the main components of To date
a total of 20 distinct mucin genes have been identi-
Questions arise as to when irregularities within the
Mucins are categorized into 3 groups on the
mucus patterns and the menstrual cycle should be
basis of their structural properties such as transmem-
considered abnormal and when the woman should
brane mucin (MUCs 1, 2, 3, 4, 12, 13, 15, 16, 17),
be sufficiently concerned to consult a physician. Per-
gel-forming mucin (MUCs 2, 5AC, 5B, 6) and soluble
sistence of abnormal mucus patterns may herald re-
mucin (MUCs 7, 9, 11, 14) and others that have not yet
productive system disorders. These may be due to
been categorized (MUCs 8, 10, 18, 19, and The
serious metabolic or endocrine abnormalities or to
four large gel-forming mucin genes are located on
other diseases, all of which need to be recognized.
Menstrual disorders and alteration in the mucus pat-
forming mucin expressed by the endocervical epithe-
tern can be caused by obstetrical, endocrine, gyneco-
lium and its expression peaks at mid-cycle.There
is evidence of other mucins as well, such as MUC4,
Early pregnancy complications such as bleeding or
which are expressed in the ovulatory phase.
vaginal spotting can alert the woman who has recog-
Two main types of cervical mucus have been de-
nized a previous fertile phase with a peak day, and can
scribed: estrogenic and progestational. According to
be identified or ruled out with the use of ultrasensitive
Odeblad’s model, the estrogenic type can be subdi-
pregnancy tests and pelvic ultrasound. Numerous
vided into L, S, and P subtypes.The L subtype
studies have shown that 10–15% of couples suffer
is the most abundant type of mucus during the perio-
from a fertility disorder. These are mainly due to:
vulatory period and the P subtype appears close to
(a) ovulatory dysfunction generally caused by hor-
monal disorders, and (b) inflammatory processes usu-
as progesterone levels increase in the blood.During
ally secondary to genital tract infections (GTI),
the luteal phase the progestational type (G) of mucus
mainly sexually transmitted diseases (STD). Ovulatory
dysfunction is the most common disorder diagnosed in
It has been demonstrated that fertility awareness
infertile couples (37%) and is predominantly associ-
can help women to identify the different stages of
ated with irregular menstrual cycles. Irregular cycles
their reproductive life cycle.Understanding the
are present in 10% of women, but having an irregular
signs of fertility and infertility is important knowledge
cycle does not necessarily mean having an ovulatory
which should be available to every woman. Briefly,
dysfunction. We have been able to show according to
fertility awareness involves self detection of mucus
cycle charting that 43% of women with irregular cycles
at the vulva primarily by noting the progression from
present an ovulatory dysfunction, which can be charac-
the basic infertile pattern of post-menstrual dryness to
terized by the absence of ovulation or abnormal ovula-
stickiness, wetness, and ultimate lubrication, the
tory activity, as seen in cycles with short or abnormal
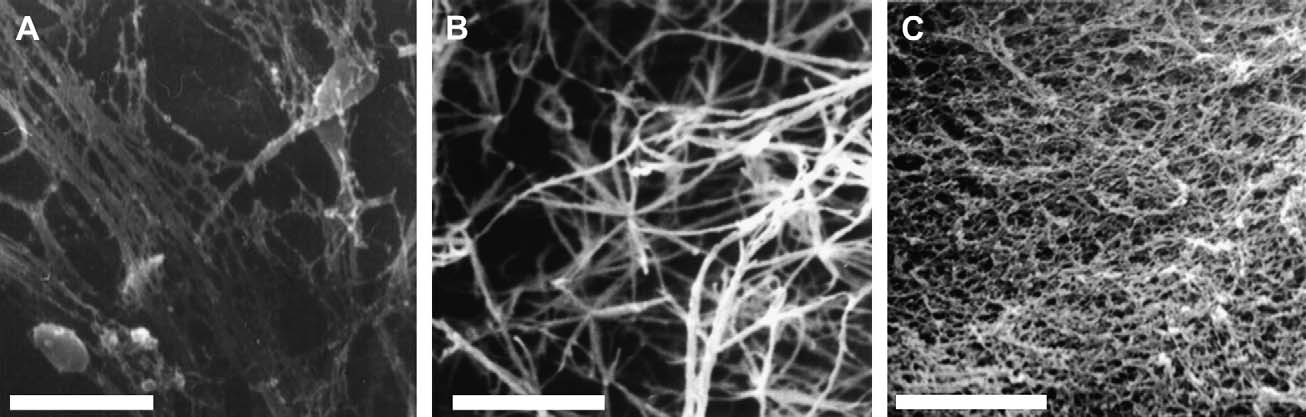
Fig. 1. Scanning electron-micrograph of cervical mucus types. Network-shaped mesh of estrogenic cervical mucus (type S)with spermatozoa migrating through it (A). In the estrogenic period type P mucus (B) appears close to ovulation. In the pro-gestational period (C) the mucus is compact and impenetrable (type G). Bar 5 10 mm.
Vigil et al: Usefulness of Monitoring Fertility from Menarche
luteal phases, while some of the rest have prolonged
are characterized by a hyperestrogenic state where
early infertile phases followed by a late, but normal
a continuous fertile type of mucus pattern (slippery,
ovulation. On the other hand, a young nulliparous
stringy, clear, mucus) is identified, or mucus patches
woman with regular cycles, (i.e., cycle length between
(days of sticky or slippery mucus forming no progres-
25 and 36 days) may also present an ovulatory dysfunc-
sive pattern to ‘‘peak’’) are present. Cycles can be
tion identified by her understanding of the fertility pat-
ovulatory, with a long follicular phase, or anovulatory.
When a young woman complains of menstrual abnor-
Endocrine disorders are the most common cause of
malities, teaching her to observe her fertility signs can
be the first step to enable the clinician to rule out met-
pothalamic, pituitary, or adrenal and/or ovarian, or
abolic conditions such as hyperinsulinemia. Our stud-
ies have shown that in 82% of women who present
Hypothalamic disorders (e.g., anorexia nervosa)
with menstrual irregularities, an endocrine abnormal-
are characterized by long hypo-estrogenic cycles with
ity is present of which hyperandrogenemia is the most
the persistence of ‘‘dry’’ days (days with no mucus).
common (46% of It is important to note that
Amenorrhea may be present. This condition is caused
an impaired insulin response to the oral glucose toler-
by a delay of the FSH levels to rise above threshold
ance test is a commonly (50–80%) associated condi-
and thus initiate a new cycle. Unless the woman has
tion in these women. This requires treatment to
permanent ovarian failure, such as having reached
prevent progression to type II diabetes mellitus.
menopause, the situation eventually corrects itself.
Proper care, including diet, exercise, and medical
This condition is associated with long ovulatory or
treatment will restore normal cyclical ovarian activity.
Women who know how to recognize their mucus
Long, anovulatory cycles are seen in athletes, and
symptoms will be able to follow the improvement
in this case they could be considered as a part of
the continuum. These women frequently return to reg-
Hypothyroidism is a less frequent (about
ular ovarian cyclic activity observed within 3 months
cause of ovarian dysfunction but it has to be consid-
of less strenuous physical exercHowever, some
ered along with hyperthyroidism. Different types of
of the young women in this category may further de-
ovarian dysfunction can be observed in patients with
velop an anorectic state and despite discontinuation of
thyroid disorders. Menorrhagiais frequently associ-
strenuous physical activity will not return to normal
ated with hypothyroidism. Although there is no spe-
cific pattern of ovarian activity associated with these
Pituitary disorders (e.g. hyperprolactinemia) ac-
endocrine abnormalities they should always be kept
count for about 10% of ovarian dysfunction and are
in mind and eliminated as a possible cause.
characterized either by amenorrhea or short cycles
Women with ovulatory dysfunctions associated
in which a short or abnormal luteal phase with pre-
with irregular cycles and abnormal mucus patterns
menstrual spotting can be observed. In vitro studies
will not usually resume normal cycling spontaneously
have shown impairment in steroidogenic activity of
without appropriate treatment. Follow-up studies have
follicular cells under the influence of prolactin, which
shown that in the absence of treatment these condi-
could explain, at least in part, the abnormal luteal
phases commonly observed in the charts of women
Other conditions, such as premature ovarian fail-
with hyperprolactinemia.Galactorrhea may be also
ure, may also be a cause of fertility disorders present-
present. In women with hyperprolactinemia the inter-
ing with irregular mucus patterns in response to
action between neurological, endocrine, and immune
fluctuating estrogen levels. These conditions are also
observed in the perimenopausal period, where some
women may also present some immunologic alter-
cycles show an ovulatory pattern. As the condition
ations such as allergies. Stress may be an important
worsens, anovulatory cycles will predominate.
factor associated with increased prolactin le
In fertile women, naturally occurring midcycle cer-
Adrenal and ovarian abnormalities are the most
vical mucus studied with scanning electron micros-
frequent cause of ovarian dysfunction. The most com-
copy shows an arrangement of parallel fibers
mon is the polycystic ovary syndrome (PCOS): an
oriented along the main axis of the mucus sample,
ovulatory dysfunction caused by hyperandrogene-
mia.In these women, irregular cycles are usually
transport may be facilitated by this normally occur-
ring condition. At mid-cycle, cervical mucus is
when present at 15 years of age has recently been
greater in quantity, has more mucin and less protein,
shown to be the best predictor for These girls
and has higher water content than in the luteal
may present with acne and/or hirsutism as well as in-
This increase in the amount of mucin in the
creased body weight and mood changes. Their cycles
cervical canal, because of its hydrophilic character,
Vigil et al: Usefulness of Monitoring Fertility from Menarche
probably functions to retain or hold water in place at
Trichomonas vaginalis, and Gardnerella vaginalis
the cell surface, keeping the cervical canal patent for
among others, must also be considered when unusual
sperm migration. The increase in water content of the
mucus patterns or menstrual irregularities occur. In
mucin may protect the cervix. Pathogens or other
this situation, both members of the couple should be
toxins may be trapped by the mucin, thus preventing
treated in order to restore the healthy condition.
their entry into the uterus and Fallopian Fu-
Fertility disorders may also be iatrogenic, caused
ture research is needed to establish the ultrastructure
by contraceptive pills or by hormonal therapy. Women
and biochemical properties of mucus in different
discontinuing steroidal contraception may present cy-
endocrine abnormalities. Also, the function of the
cles with short luteal phases, absence of a well-
specific mucins and mucus types remains to be
defined mucus pattern indicating anovulation, poor
determined as well as their possible alterations.
mucus response due to damaged cervical epithelium
Menstrual disorders and alteration in the mucus
and/or a poor menstrual flow due to alterations of
pattern can also be caused by gynecologic disorders
such as anatomical abnormalities, neoplasia, or in-
for up to seven cycles (cycle length O 35 days or lu-
flammatory diseases. The second most frequent cause
teal phase ! 10 days, monophasic basal body temper-
of fertility disorders are inflammatory processes, usu-
ature or anovulatory cycles) occur in women after
ally secondary to GTI, which predominantly have
discontinuation of oral contraception. They also have
their origin in STD. Microbial mucin degrading en-
lower monthly conception rates during the first 3
zymes are associated with sexually transmitted infec-
months off the pill, and a somewhat lower percentage
tions and are produced by the offending micro
from the fourth to the tenth month after discontinua-
organisms. These enzymes will alter the mutually
beneficial cohabitation that normally exists between
In conclusion, although usually used for fertility
commensals such as Lactobacillus, which use glyco-
awareness, cycle charting provides women with infor-
gen as an energy source and contribute to normal mu-
mation about their cycle pattern and ovarian function.
cin turnover by the production of mucin degrading
Klaus and Martinshowed that ethnically and socio-
enzymes such as sialidase. Mucin molecules would
economically diverse perimenarchal girls can be
be partly or completely degraded by the microbial en-
taught to recognize their cervical mucus patterns
zymes. These molecules dictate the rheological prop-
and distinguish anovulatory from ovulatory c
erties which determine the amount and viscosity of
Menstrual irregularities and/or ovarian dysfunction
the mucus, so these properties will change in response
may reflect several systemic or reproductive disor-
to enzymes produced by microbial organisms in the
ders. Recent studies have shown that the menstrual
cycle pattern during the first years after menarche is
A woman who knows her own mucus pattern in
a better predictor for ovulatory dysfunction in adult-
times of health will be able to recognize a GTI early.
These will usually cause a continuous discharge
and other previously conducted studies support the
whose characteristics will depend upon the etiologic
evidence that conditions such as hyperandrogenic
agent causing the infection. In general, an ovulatory
ovulatory dysfunction in the adult female have their
pattern is identifiable alongside the continuous dis-
origin in adolescence. Most of these conditions are
charge. Symptomatic infections (itching and a charac-
not self-limited disorders and will worsen during
teristic discharge) are usually caused by fungi,
bacteria, or parasites. Chlamydia trachomatis infec-
women were taught how to chart their cycles they
tions, with an incidence of 13% in infertile couples
could be able to detect menstrual irregularities and
and often associated with tubal pathology, may be
ovarian dysfunction early in life. This finding could
asymptomatic or present with continuous vulvar
alert women to seek medical advice early which could
moistness and variable degrees of pelvic pain.This
be crucial for the prevention of disorders such as type
infection may also show a mucopurulent discharge as-
sociated with the mucus discharge. The recognition of
Furthermore, sex education programs that include
this infection and timely treatment may prevent fertil-
training in fertility awareness have an impact in pre-
ity disorders. It has been shown that these infections
vention of unintended adolescent pregnancyThese
provoke pelvic inflammatory processes and are asso-
programs have shown retardation of sexual initiation
ciated with spontaneous abortions. Recent studies
and discontinuation of sexual activity among sexually
have shown that the mesh spacing between mucin fi-
active adolescents, which is important for prevention
bers is large enough for small viruses such as human
papilloma virus, associated with cervical neoplasia,
Teaching fertility awareness to young women in-
volves an effort that may be useful for every women
Vigil et al: Usefulness of Monitoring Fertility from Menarche
ovulatory cycles by comparison with radioimmunoassay. Steroids 2003; 68:465
Knowledge about fertility awareness acquired by self
10. Noyes RW, Hertig AT, Rock J: Dating the endometrial
observation of cervical mucus patterns at the vulva is
an invaluable tool for women desiring to achieve and
11. Johannisson E, Oberholzer M, Swahn ML, et al: Vascular
changes in the human endometrium following the admin-
maintain a healthy reproductive system. The identifi-
istration of the progesterone antagonist RU 486. Contra-
cation of medical and environmental causes of abnor-
mal menstrual cycle patterns may provide clues to the
12. Barros C, Arguello B, Jedlicki A, et al: Scanning electron
causes of the most frequent fertility disorders. Early
microscopy study of human cervical mucus. Gam Res
diagnosis of these alterations, as can be achieved
through fertility awareness, will not only improve fer-
13. Morales P, Rocco M, Vigil P: Human cervical mucus:
tility disorders, but may help in the diagnosis and
relationship between biochemical characteristics and ability
treatment of other pathologies such as metabolic
to allow migration of spermatozoa. Hum Reprod 1993; 8:78
and endocrine disorders, anatomical alterations, pel-
14. Vigil P, Pe´rez A, Neira J, et al: Post-partum cervical mu-
vic inflammatory diseases or even neoplasia. Mucus
cus: biological and rheological properties. Hum Reprod
as well as the menstrual cycle patterns are important
15. Armstrong DG, Webb R: Ovarian follicular dominance:
components of the clinical decision-making process.
the role of intraovarian growth factors and novel proteins. Rev Reprod 1997; 2:139
Acknowledgments: We would like thank to Dr. James B. Brown
16. Laven JS, Fauser BC: Inhibins and adult ovarian function.
and Dr. Emil Steinberger for their teaching throughout the
years and for the discussion leading to this article. Further-
17. Hoff JD, Quiglel ME, Yen SS: Hormonal dynamics at mid-
more, we would like to extend thanks to Dr. Gareth I. Owen
cycle: a reevaluation. J Clin Endocrinol Metab 1983; 57:792
for his commentary on the manuscript.
18. Ferin MD, Van Vugt D, Warlaw S: The hypothalamic
control of the menstrual cycle and the endogenous opioidpeptides. Rec Prog Horm Res 1984; 40:441
19. Miyake A, Kawamura Y, Aono T, et al: Changes in plasma
LRH during the normal menstrual cycle in women. Acta
1. Lunenfeld B, Insler V: Follicular development and its con-
20. Misao R, Nakanishi Y, Iwagaki S, et al: Expression of
2. Roche JF: Control and regulation of folliculogenesisda
progesterone receptor isoforms in corpora lutea of human
symposium in perspective. Rev Reprod 1996; 1:19
subjects: correlation with serum estrogen and progesterone
3. Vigil P, Rodrı´guez-Rigau L, Palacios X, et al: Diagnosis of
concentrations. Mol Hum Reprod 1998; 4:1045
menstrual disorders in adolescence. In: Reproductive
21. Elstein M, Daunter B: The structure of cervical mucus. In:
Medicine. Frajese G, Steinberger E, Rodrı´guez-Rigau LJ,
The Cervix. Edited by JA Jordan, A Singer. London, W.B.
editors. New York, Raven Press, 1993, pp 149–154
4. Brown JB, Blackwell LF, Holmes J, et al: New assays for
22. Odeblad E, Ingelman-Sundberg A, Hallstro¨m L, et al: The
identifying the fertile period. Int J Gynecol Obstet 1989;
biophysical properties of cervical-vaginal secretions. Int
5. Blackwell LF, Brown JB, Cooke DG: Definition of the po-
23. Vollman RF: The menstrual cycle. In: Major Problems in
tentially fertile period from urinary steroid excretion rates.
Obstetrics and Gynecology, (1st ed.). Edited by EA
Part II. A threshold value for pregnanediol glucuronide as
Friedman. Toronto, W.B. Saunders, 1977, pp 11–193
a marker for the end of the potentially fertile period in the
24. Yen SSC, Tsai CC: The biphasic pattern in the feedback
human menstrual cycle. Steroids 1998; 63:5
action ethynyl estradiol on the release of FSH and LH.
6. Brown J: Ovarian activity and fertility and the Billings ovu-
lation method. In: Studies on Human Reproduction. Mel-
25. Lincoln DW, Fraser HM, Lincoln GA: Hypothalamic pulse
bourne, Ovul Meth Res Ref Centre Australia, 2000.
generators. Rec Prog Horm Res 1985; 41:369
26. Yen SSC: The human menstrual cycle. In: Reproductive
Endocrinology: Physiology, Pathophysiology and Clinical
7. Miro F, Aspinall LJ: The onset of the initial rise in follicle-
Management, (2nd ed.). Edited by SSC Yen, RB Jaffe.
stimulating hormone during the human menstrual cycle.
Philadelphia, W.B. Saunders, 1991, pp 273–308
27. Brown JB, Blackwell LF, Billings JJ, et al: Natural family
8. Catt KJ, Pierce JG: Gonadotropin hormones of the adeno-
planning. Am J Obstet Gynecol 1987; 157:1082
hypophysis. In: Reproductive Endocrinology: Physiology,
28. Blackwell LF, Brown JB: Application of time-series anal-
Pathophysiology and Clinical Management. Edited by
ysis for the recognition of increases in urinary estrogens as
SSC Yen, RB Jaffe. Philadelphia, W.B. Saunders, 1978,
markers for the beginning of the potentially fertile period.
9. Blackwell LF, Brown JB, Vigil P, et al: Hormonal monitor-
29. Moniaux N, Escande F, Porchet N, et al: Structural organi-
ing of ovarian activity using the ovarian monitor. Part I.
zation and classification of the human mucin genes. Front
Validation of home and laboratory results obtained during
Vigil et al: Usefulness of Monitoring Fertility from Menarche
30. Ceric F, Silva D, Vigil P: Ultrastructure of the human peri-
48. Vigil P, Kolbach M, Aglony M, et al: Hiperandrogenismo e
ovulatory cervical mucus. J Electron Microsc (Tokyo)
irregularidades menstruales en mujeres jo´venes. Rev Chil
31. Gipson IK, Moccia R, Spurr-Michaud S, et al: The amount
49. Van Hooff MHA, Voorhorst FJ, Kaptein MB, et al: Predic-
of MUC 5B mucin in cervical mucus peaks at midcycle.
tive value of menstrual cycle pattern, body mass index, hor-
mone levels and polycystic ovaries at age 15 years for
32. Gipson IK, Spurr-Michaud S, Moccia R, et al: MUC4 and
oligomenorrhoea at age 18 years. Hum Reprod 2004; 19:383
MUC5B transcripts are the prevalent mucin messenger ri-
50. Koutras DA: Disturbances of menstruation in thyroid dis-
bonucleic acids of the human endocervix. Biol Reprod
51. Howe L, Wiggins R, Soothill PW, et al: Mucinase and sia-
33. Gipson IK: Mucins of the human endocervix. Front Biosci
lidase activity of the vaginal microflora: implications for
the pathogenesis of preterm labour. Int J STD AIDS
34. Barbieri RL: Infertility. In: Reproductive Endocrinology:
Physiology, Pathophysiology and Clinical Management
52. Stadtmauer LA, Wong BC, Oehninger S: Should patients
(4th ed.). Edited by SSC Yen, RB Jaffe. Philadelphia,
with polycystic ovary syndrome be treated with metfor-
min? Benefits of insulin sensitizing drugs in polycystic
35. Billings EL, Billings JJ, Catarinich M: Billings Atlas of the
ovary syndrome beyond ovulation induction. Hum Reprod
Ovulation Method. The Mucus Patterns of Fertility and
Infertility. Melbourne, Advocate Press, 1989, pp 1–108
53. Vigil P, Morales P, Tapia A, et al: Chlamydia trachomatis
36. Vigil P: La Fertilidad de la Pareja Humana. Santiago de
infection in male partners of infertile couples: Incidence
Chile, Ediciones Universidad Cato´lica de Chile, 2004, pp
and sperm function. Andrologia 2002; 34:155
54. Olmsted SS, Padgett JL, Yudin AI, et al: Diffusion of mac-
37. Ceric F, Riquelme R, Pinto E, et al: Scanning electron mi-
romolecules and virus-like particles in human cervical mu-
croscopy study of cervical mucus during the periovulatory
55. Pinkerton GD, Carey HM: Post-pill anovulation. Med J
38. Gipson IK, Ho SB, Spurr-Michaud SJ, et al: Mucin genes
expressed by human female reproductive tract epithelia.
56. Linn S, Schoenbaum SC, Monson RR, et al: Delay in con-
ception for former ‘pill’ users. JAMA 1982; 247:629
39. Billings EL, Billings JJ, Brown JB, et al: Symptoms and hor-
57. Kolstad HA, Bonde JP, Hjøllund NH, et al: Menstrual cycle
monal changes accompanying ovulation. Lancet 1972; 1:282
pattern and fertility: a prospective follow-up study of preg-
40. Klaus H: Natural family planning: a review. Obstet Gyne-
nancy and early embryonal loss in 295 couples who were
planning their first pregnancy. Fertil Steril 1999; 71:490
41. Klaus H, Martin JL: Recognition of ovulatory/anovulatory
58. Gnoth C, Frank-Herrmann P, Schmoll A, et al: Cycle char-
cycle pattern in adolescents by mucus self-detection.
acteristics after discontinuation of oral contraceptives. Gy-
42. Mansfield MJ, Emans SJ: Anorexia nervosa, athletics, and
59. Steinberger E, Rodrı´guez-Rigau LJ, Ayala C, et al: Conse-
amenorrhea. Pediatr Clin North Am 1989; 36:533
quences of hyperandrogenism during adolescence on the
43. Diddle AW: Athletic activity and menstruation. South Med
ovarian function of adult female. In: Reproductive Medi-
cine. Edited by G Frajese, E Steinberger, LJ Rodrı´guez-
44. Barron ML: Proactive management of menstrual cycle ab-
Rigau. New York, Raven Press, 1993, pp 253–264
normalities in young women. J Perinat Neonatal Nurs
60. Cabezo´n C, Vigil P, Rojas I, et al: Adolescent pregnancy
prevention: An abstinence-centered randomized controlled
45. Clark R: The somatogenic hormones and insulin-like
intervention in a Chilean public high school. J Adolesc
growth factor I: stimulators of lymphopoiesis and immune
61. Vigil P, Riquelme R, Rivadeneira R, et al: Effect of Teen-
46. Johansson GG, Karonen SL, Laakso ML: Reversal of an
STARÒ, an Abstinence-only Sexual Education Program on
elevated plasma level of prolactin during prolonged psy-
Adolescent Sexual Behavior. J Pediatr Adolesc Gynecol
chological stress. Acta Physiol Scand 1983; 119:463
47. Vigil P, Steinberger E, del Rı´o MJ, et al: Sı´ndrome de
62. Vigil P, Riquelme R, Rivadeneira R, et al: TeenSTAR: Una
ovario poliquı´stico. In: Guzma´n E, editor. Seleccio´n de
opcio´n de madurez y libertad. Programa de educacio´n in-
Temas en Ginecoobstetricia. Santiago de Chile, Editorial
tegral de la sexualidad, orientado a adolescentes. Rev Me´d
The initial healing period typically takes from one to two weeks, gum tissue takes about 3-4 weeks to heal and complete healing of the bone can take about 6-8 months depending on your care of this area. As your mouth heals, you can promote faster healing and avoid complications by simply following these instructions. DO NOT DISTURB THE WOUND: The healing process begins immediately aftersurgery
CHAPTER 16b: SEXUALLY TRANSMITTED DISEASES (STDs) I. Viral Infections A. Pathogens : Viruses, bacteria, and other organisms that cause disease. B. Viruses : Incapable of independent reproduction. They reproduce only inside a living host cell—obligate intracellular parasites. 1. Virus particles are generally very small, about ten times smaller than a bacterium. 2. Composed of an
 Vigil et al: Usefulness of Monitoring Fertility from Menarche
Cervical Mucus as a Determinant for Fertility
‘‘peak day.’The woman who understands herown mucus pattern should be able to recognize
It has been shown that mucus quality is a better predic-
changes in the normal ovulatory pattern and detect
tor of the possibility for conception than ovulation.
Vigil et al: Usefulness of Monitoring Fertility from Menarche
Cervical Mucus as a Determinant for Fertility
‘‘peak day.’The woman who understands herown mucus pattern should be able to recognize
It has been shown that mucus quality is a better predic-
changes in the normal ovulatory pattern and detect
tor of the possibility for conception than ovulation.