Journal of the American Medical Informatics Association Volume 8 Number 4 Jul / Aug 2001
Focus on Quality Improvement
Reducing the Frequency ofErrors in Medicine UsingInformation Technology
DAVID W. BATES, MD, MSC, MICHAEL COHEN, MS, RPH,
LUCIAN L. LEAPE, MD, J. MARC OVERHAGE, MD, PHD,
M. MICHAEL SHABOT, MD, THOMAS SHERIDAN, SCD
A b s t r a c t Background: Increasing data suggest that error in medicine is frequent and results in substantial harm. The recent Institute of Medicine report (LT Kohn, JM Corrigan, MS Donaldson, eds: To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press, 1999) described the magnitude of the problem, and the public interest in this issue, which was already large, has grown. Goal: The goal of this white paper is to describe how the frequency and consequences of errors in medical care can be reduced (although in some instances they are potentiated) by the use of information technology in the provision of care, and to make general and specific recommendations regarding error reduction through the use of information technology. Results: General recommendations are to implement clinical decision support judiciously; to consider consequent actions when designing systems; to test existing systems to ensure they actually catch errors that injure patients; to promote adoption of standards for data and systems; to develop systems that communicate with each other; to use systems in new ways; to measure and prevent adverse consequences; to make existing quality structures meaningful; and to improve regulation and remove disincentives for vendors to provide clinical decision support. Specific recommendations are to implement provider order entry systems, especially computerized prescribing; to implement bar-coding for medications, blood, devices, and patients; and to utilize modern electronic systems to communicate key pieces of asynchronous data such as markedly abnormal laboratory values. Conclusions: Appropriate increases in the use of information technology in health care— especially the introduction of clinical decision support and better linkages in and among systems, resulting in process simplification—could result in substantial improvement in patient safety.
■ J Am Med Inform Assoc. 2001;8:299–308.
Affiliations of the authors: Harvard Medical School, Boston,
This work is based on discussions at the AMIA 2000 Spring
Massachusetts (DWB); Institute for Safe Medication Practices,
Congress; May 23–25, 2000; Boston, Massachusetts.
Huntingdon Valley, Pennsylvania (MC); Harvard School of Public
Correspondence and reprints: David W. Bates, MD, MSc, Division of
Health, Boston (LLL); Indiana University of Medicine,
General Medicine and Primary Care, Brigham and Women’s Hospital,
Indianapolis, Indiana (JMO); University of California–Los Angeles
75 Francis Street, Boston, MA 02115; e-mail: <[email protected]>.
School of Medicine, Los Angeles, California (MMS); MassachusettsInstitute of Technology, Cambridge, Massachusetts (TS).
Received for publication: 10/09/00; accepted for publication: 3/16/01.
Our goal in this manuscript is to describe how infor-
recommended by the IOM involves all stakeholders—
mation technology can be used to reduce the frequen-
professionals, health care organizations, regulators,
cy and consequences of errors in health care. We begin
professional societies, and purchasers. Health care
by discussing the Institute of Medicine report and the
organizations are called on to work with their profes-
evidence that errors and iatrogenic injury are a prob-
sionals to implement known safe practices and set up
lem in medicine, and also briefly mention the issue of
meaningful safety programs in their institutions, in-
inefficiency. We then define our scope of discussion
cluding blame-free reporting and analysis of serious
(in particular, what we are considering an error) and
errors. External organizations—regulators, profession-
then discuss the theory of error as it applies to infor-
al societies, and purchasers—are called on to help
mation technology, and the importance of systems
establish standards and best practice for safety and to
improvement. We then discuss the effects of clinical
hold health care organizations accountable for imple-
decision support, and errors generated by information
technology. That is followed by management issues,
Some of the best available data on the epidemiology
the value proposition, barriers, and recent develop-
of medical injury come from the Harvard Medical
ments on the national front. We conclude by making a
Practice Study.4 In that study, drug complications
number of evidence-based general and specific recom-
were the most common adverse event (19 percent),
mendations regarding the use of information technol-
followed by wound infections (14 percent) and tech-
ogy for error prevention in health care.
nical complications (13 percent). Nearly half theevents were associated with an operation. Most work
The Institute of Medicine Report and
on prevention to date has focused on adverse drug
Iatrogenesis
events and wound infections. Compared with thedata on inpatients, relatively few data on errors and
Errors in medicine are frequent, as they are in all
injuries outside the hospital are available, although
domains in life. While most errors have little poten-
errors in follow-up5 and diagnosis are probably espe-
tial for harm, some do result in injury, and the cumu-
cially important in non-hospital settings.
lative consequences of error in medicine are huge.
While the IOM report and Harvard Medical Practice
When the Institute of Medicine (IOM) released its
Study deal primarily with injuries associated with
report To Err is Human: Building a Safer Health System in
errors in health care, the costs of inefficiencies related
November 1999,1 the public response surprised most
to errors that do not result in injury are also great.
people in the health care community. Although the
One example is the effort associated with “missed
report’s estimates of more than a million injuries and
dose” medication errors, when a medication dose is
nearly 100,000 deaths attributable to medical errors
not available for a nurse to administer and a delay of
annually were based on figures from a study pub-
at least two hours occurs or the dose is not given at
lished in 1991, they were news to many. The mortality
all.6 Nurses spend a great deal of time tracking down
figures in particular have been a matter of some pub-
such medications. Although such costs are harder to
lic debate2,3 although most agree that whatever the
assess than the costs of injuries, they may be even
The report galvanized an enormous reaction from
Scope of Discussion
both government and health care representatives. Within two weeks, Congress began hearings and thePresident ordered a government-wide feasibility
In this paper, we are discussing only clear-cut errors
study, followed in February by a directive to govern-
in medical care and not suboptimal practice (such as
mental agencies to implement the IOM recommenda-
failure to follow a guideline). Clearly, this is not a
tions. During this time, professional societies and
dichotomous distinction, and some examples may be
health care organizations have begun to re-assess
helpful. We would consider a sponge left in the
patient after surgery an error, whereas an inappro-priate indication for surgery would be suboptimal
The IOM report made four major points—the extent of
practice. We would consider it an error if no postop-
harm that results from medical errors is great; errors
erative anticoagulation were used in patients in
result from system failures, not people failures; achiev-
whom its benefit has clearly been demonstrated (for
ing acceptable levels of patient safety will require
example, patients who have just had hip surgery).
major systems changes; and a concerted national effort
However, we would not consider it an error if a
is needed to improve patient safety. The national effort
physician failed to follow a pneumonia guideline and
Journal of the American Medical Informatics Association Volume 8 Number 4 Jul / Aug 2001
prescribed a commonly used but suboptimal antibi-
resourceful and inventive, and they can recover from
otic, even though adherence to such guidelines will
both their own and the equipment’s errors in creative
almost certainly improve outcomes. Although we
ways. In comparison, machines are more depend-
believe that information technology can play a major
able, which means they are dependably stupid when
role in both domains, we are not addressing subopti-
a minor behavior change would prevent a failure in a
neighboring component from propagating. The intel-ligent machine can be made to adjust to an identified
Theory of Error
variable whose importance and relation to other vari-ables are sufficiently well understood. The intelligent
Although human error in health care systems has
human operator still has usefulness, however, for he
only recently received great attention, human factors
or she can respond to what at the design stage may
engineering has been concerned with error for sever-
be termed an “unknown unknown” (a variable
al decades. Following the accident at Three Mile
which was never anticipated, so that there was never
Island in the late 1970s, the nuclear power industry
any basis for equations to predict it or computers and
was particularly interested in human error as part of
human factors concerns, and has produced a number
Finally, we seek to reduce the undesirable conse-
of reports on the subject.7 The U.S. commercial avia-
quences of error, not error itself. Senders and
tion sector is also very interested in human error at
Moray10 provide some relevant comments that relate
present, because of massive overhaul of the air traffic
to information technology: “The less often errors
control network. A few excellent books on human
occur, the less likely we are to expect them, and the
more we come to believe that they cannot happen… .
While it is easy and common to blame operators for
It is something of a paradox that the more errors we
accidents, investigation often indicates that an opera-
make, the better we will be able to deal with them.”
tor “erred” because the system was poorly designed.
They comment further that, “eliminating errors local-
Testimony of an operator of the Three Mile Island
ly may not improve a system and might cause worse
nuclear power plant in a 1979 Congressional hear-
ing11 makes the point, “ If you go beyond what the
A medical example relating to these issues comes from
designers think might happen, then the indications
the work of Macklis et al. in radiation therapy12; this
are insufficient, and they may lead you to make the
group has used and evaluated the safety record of a
wrong inferences. …[H]ardly any of the measure-
record-and-verify linear accelerator system that dou-
ments that we have are direct indications of what is
ble-checks radiation treatments. This system has an
error rate of only 0.18 percent, with all detected errorsbeing of low severity. However, 15 percent of the
The consensus among man–machine system engi-
errors that did occur related to use of the system, pri-
neers is that we should be designing our control
marily because when an error in the checking system
rooms, cockpits, intensive care units, and operating
occurred, the human operators assumed the machine
rooms so that they are more “transparent”—that is,
“had to be right,” even in the face of important con-
so that the operator can more easily “see through”
flicting data. Thus, the Macklis group expressed con-
the displays to the actual working system, or “what
cern that over-reliance on the system could result in an
is going on.” Situational awareness is the term used
accident. This example illustrates why it will be vital to
in the aviation sector. Often the operator is locked
measure to determine how systems changes affect the
into the dilemma of selecting and slavishly following
overall rate of not only errors but accidents.
one or another written procedure, each based on ananticipated causality. The operator may not be sure
Systems Improvement and Error Prevention
what procedure, if any, fits the current not-yet-understood situation.
Although the traditional approach in medicine has
Machines can also produce errors. It is commonly
been to identify the persons making the errors and
appreciated that humans and machines are rather
punish them in some way, it has become increasing-
different and that the combination of both thus has
ly clear that it is more productive to focus on the sys-
greater potential reliability than either alone. How-
tems by which care is provided.13 If these systems
ever, it is not commonly understood how best to
could be set up in ways that would both make errors
make this synthesis. Humans are erratic, and err in
less likely and catch those that do occur, safety might
surprising and unexpected ways. Yet they are also
A system analysis of a large series of serious medica-
in a controlled trial that computerized physician
tion errors (those that either might have or did cause
order entry systems resulted in a 55 percent reduction
harm)13 identified 16 major types of system failures
in serious medication errors. In another time series
associated with these errors. Of these system failures,
study,22 this group found an 83 percent reduction in
all of the top eight could have been addressed by bet-
the overall medication error rate, and a 64 percent
reduction even with a simple system. Evans et al.23have also demonstrated that clinical decision support
Currently, the clinical systems in routine use in
can result in major improvements in rates of antibiot-
health care in the United States leave a great deal to
ic-associated adverse drug events and can decrease
be desired. The health care industry spends less on
costs. Classen et al.24 have also demonstrated in a
information technology than do most other informa-
series of studies that nosocomial infection rates can be
tion-intensive industries; in part as a result, the
dream of system integration been realized in feworganizations. For example, laboratory systems do
Another class of clinical decision support is comput-
not communicate directly with pharmacy systems.
erized alerting systems, which can notify physicians
Even within medication systems, electronic links be-
about problems that occur asynchronously. A grow-
tween parts of the system—prescribing, dispensing,
ing body of evidence suggests that such systems
and administering—typically do not exist today.
may decrease error rates and improve therapy,
Nonetheless, real and difficult issues are present in
thereby improving outcomes, including survival, the
the implementation of information technology in
length of time patients spend in dangerous condi-
health care, and simply writing a large check does
tions, hospital length of stay, and costs.25–27 While an
not mean that an organization will necessarily get an
increasing number of clinical information systems
outstanding information system, as many organiza-
contain data worthy of generating an alert message,
tions have learned to their chagrin.
delivering the message to caregivers in a timely wayhas been problematic. For example, Kuperman et
Evaluation is also an important issue. Data on the
al.28 documented significant delays in treatment
effects of information technology on error and
even when critical laboratory results were phoned to
adverse event rates are remarkably sparse, and many
caregivers. Computer-generated terminal messages,
more such studies are needed. Although such evalu-
e-mail, and even flashing lights on hospital wards
ations are challenging, tools to assess the frequencyof errors and adverse events in a number of domainsare now available.14–19 Errors are much more fre-quent than actual adverse events (for medicationerrors, for example, the ratio in one study6 was100:1). As a result, it is attractive from the sample sizeperspective to track error rates, although it is impor-tant to recognize that errors vary substantially intheir likelihood of causing injury.20
Clinical Decision Support
While many errors can be detected and corrected byuse of human knowledge and inspection, these rep-resent weak error reduction strategies. In 1995, Leapeet al.13 demonstrated that almost half of all medica-tion errors were intimately linked with insufficientinformation about the patient and drug. Similarly,when people are asked to detect errors by inspection,they routinely miss many.21
It has recently been demonstrated that computerizedphysician order entry systems that incorporate clini-
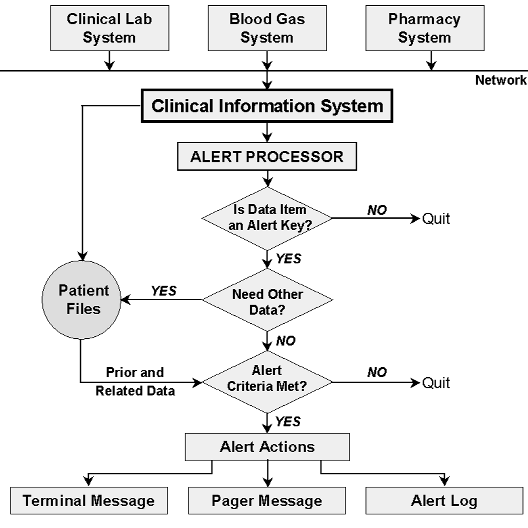
Alert detection system. Three major forms of
cal decision support can substantially reduce medica-
critical event detection occur—critical laboratory alerts,
tion error rates as well as improve the quality and effi-
physiologic “exception condition” alerts, and medication
ciency of medication use. In 1998, Bates et al.20 found
Journal of the American Medical Informatics Association Volume 8 Number 4 Jul / Aug 2001
2 Wireless alerting system. In the Cedars-Sinai system, alerts are initially detected by the clinical system, then
sent to a server, then via the Internet, then sent over a PageNet transmitter to a two-way wireless device.
have been tried.29–32 A new system, which transmits
includes appropriate patient identification informa-
real-time alert messages to clinicians carrying
alphanumeric pagers or cell phones, promises to
Alerts are a crucial part of a clinical decision support
eliminate the delivery problem.33,34 It is now possible
system,35 and their value has been demonstrated in
to integrate laboratory, medication, and physiologic
controlled trials.27,35 In one study, Rind et al.27 alerted
data alerts into a comprehensive real-time wireless
physicians via e-mail to increases in serum creatinine
in patients receiving nephrotoxic medications or
Shabot et al.33,34 have developed such a comprehen-
renally excreted drugs. Rind et al. reported that when
sive system for patients in intensive care units. A
e-mail alerts were delivered, medications were adjust-
software system detect alerts and then sends them to
ed or discontinued an average of 21.6 hours earlier
caregivers. The alert detection system monitors data
than when no e-mail alerts were delivered. In another
flowing into a clinical information system. The detec-
study, Kuperman et al.35 found that when clinicians
tor contains a rules engine to determine when alerts
were paged about “panic” laboratory values, time to
therapy decreased 11 percent and mean time to reso-lution of an abnormality was 29 percent shorter.
For some kinds of alert detection, prior or relateddata are needed. When the necessary data have been
As more and different kinds of clinical data become
collected, alerting algorithms are executed and a
available electronically, the ability to perform more
decision is made as to whether an alert has occurred
sophisticated alerts and other types of decision sup-
(Figure 1). The three major forms of critical event
port will grow. For example, medication-related, lab-
detection are critical laboratory alerts, physiologic
oratory, physiologic data can be combined to create a
“exception condition” alerts, and medication alerts.
variety of automated alerts. (Table 1 shows a sample
When an alert condition is detected, an application
of those currently included in the system used at
formats a message and transmits it to the alphanu-
Cedars-Sinai Medical Center, Los Angeles,
meric pagers of various recipients, on the basis of a
California.) Furthermore, computerization offers
table of recipients by message type, patient service
many tools for decision support, but because of space
type, and call schedule. The message is sent as an e-
limitations we have discussed only some of these;
mail to the coded PIN (personal identification num-
Among the others are algorithms, guidelines, order
ber) of individual caregivers’ pagers or cell phones.
sets, trend monitors, and co-sign forcers. Most
The message then appears on the device’s screen and
sophisticated systems include an array of these tools.
Sample of Wireless Alerts Currently in Use at Cedars-Sinai Medical Center, Los Angeles, California
PEEP (positive end-respiratory pressure) > 15 cm H
Systolic BP < 80 mm Hg and no pulmonary artery catheter
Systolic BP < 80 mm Hg and pulmonary wedge pressure
Urine output < 0.3 cc/kg/hour and patient not admitted in
Re-admission to intensive care unit < 48 hours after discharge
Heparin flush ≥ 500 unitsHeparin injection ≥ 5000 units
Alert if urine output is low (< 0.3 cc/kg/hour for 3 hours) and the
patient is receiving gentamicin, tobramycin, vancomycin, penicillin,
ampicillin, Augmentin (amoxicillin/clavulanic acid), piperacillin,
Zosyn (piperacillin/tazobactam), oxacillin, Primaxin (imipenem/
cilastatin), or Unasyn (ampicillin/sulbactam).
Medication–laboratory data trend alerts:
Alert if serum creatinine level increases by > 0.5 mg/dL in
24 hours and the patient is receiving any of the following drugs:
gentamicin, tobramycin, amikacin, vancomycin, amphotericin,
digoxin, procainamide, Prograf (tacrolimus), cyclosporin, or ganciclovir. Errors Generated By Information Technology
cian order entry systems are separate from the phar-macy system, which requires double entry of all
Although information technology can help reduce
orders. This may result in electronic/computer-gener-
error and accident rates, it can also cause errors. For
ated medication administration records (MARs) that
example, if two medications that are spelled similar-
are derived from the order entry system database, not
ly are displayed next to each other, substitution
the pharmacy database, which can result in discrepan-
errors can occur. Also, clinicians may write an order
cies and extra work for nurses and pharmacists.
Furthermore, many computerized physician order
In particular, early adopters of vendor-developed
entry systems lack even basic screening capabilities
order entry have reported significant barriers to suc-
to alert practitioners to unsafe orders relating to over-
cessful implementation, new sources of error, and
ly high doses, allergies, and drug–drug interactions.
major infrastructure changes that have been necessary
While visiting hospitals in 1998, representatives of
to accommodate the technology. The order entry
the Institute for Safe Medication Practices (ISMP)
process with many computerized physician order
tested pharmacy computers and were alarmed to dis-
entry systems currently on the market is error-prone
cover that many failed to detect unsafe drug orders.
and time-consuming. As a result, prescribers may
Subsequently, ISMP asked directors of pharmacy in
bypass the order entry process totally and encourage
U.S. hospitals to perform a nationwide field test to
nurses, pharmacists, or unit secretaries to enter written
assess the capability of their systems to intercept
or verbal drug orders. Also, most computerized physi-
common or serious prescribing errors.36 To partici-
Journal of the American Medical Informatics Association Volume 8 Number 4 Jul / Aug 2001
pate, pharmacists set up a test patient in their com-
puter system, then entered actual physician prescrip-
Percentage of Pharmacy Computer Systems That
tion errors that had actually led to a patient’s death or
serious injury during 1998 (Table 2). Only a smallnumber of even fatal errors were detected by current
These anecdotal data suggest that current systems
may be inadequate and that simply implementing
the current off-the-shelf vendor products may not
have the same effect on medication errors that hasbeen reported in research studies. Improvement of
vendor-based systems and evaluation of their effectsis crucial, since these are the systems that will be
Management Issues
* All these orders are unsafe and have resulted in at least one fatal-
A major problem in creating the will to reduce errors
ity in the United States. However, most pharmacy systems did notdetect them, and even among those that did, a large percentage
has been that administrators have not been aware of
allowed an override without a note. Data reprinted, with permis-
the magnitude of problem. For example, one survey
sion, from ISMP Medication Safety Alert! Feb 10, 1999.36
showed that, while 92 percent of hospital CEOs
Copyright Institute for Safe Medication Practices.
reported that they were knowledgeable about the fre-quency of medication errors in their facility, only 8
result in a 12.7 percent decrease in total charges and
percent said they had more than 20 per month, when
a 0.9 day decrease in length of stay.41 Even without
in fact all probably had more than this.37 Probably in
full computerization of ordering, substantial savings
part as a result, the Advisory Board Company found
can be realized: data from LDS Hospital23 demon-
that reducing clinical error and adverse events
strated that a program that assisted with antibiotic
ranked 133rd when CEOs were asked to rank items
management resulted in a fivefold decrease in the
on a priority list.38 A number of efforts are currently
frequency of excess drug dosages and a tenfold
under way to increase the visibility of the issue. For
decrease in antibiotic-susceptibility mismatches, with
example, a video about this issue, which was devel-
substantially lower total costs and lengths of stay.
oped by the American Hospital Association and theInstitute for Healthcare Improvement, has been sent
Barriers
to all hospital CEOs in the United States, and a num-ber of indicators suggest that such efforts may be
Despite these demonstrated benefits, only a handful
of organizations have successfully implemented clin-ical decision support systems. A number of barriers
The Value Proposition
have prevented implementation. Among these arethe tendency of health care organizations to invest in
For information technology to be implemented, it
administrative rather than clinical systems; the issue
must be clear that the return on investment is suffi-
of “silo accounting,” so that benefits that accrue
cient, and far too few data are available regarding
across a system do not show up in one budget and
this in health care. Furthermore, there are many hor-
thus do not get credit; the current financial crisis in
ror stories of huge investments in information tech-
health care, which has been exacerbated by the
Balanced Budget Amendment and has made it veryhard for hospitals to invest; the lack, at many sites, of
Positive examples relate to computer order entry. At
leaders in information technology; and the lack of
one large academic hospital, the savings were esti-
mated to be $5 million to $10 million annually on a$500 million budget.39 Another community hospital
One of the greatest barriers to providing outstanding
predicts even larger savings, with expected annual
decision support, however, has been the need for an
savings of $21 million to $26 million, representing
extensive electronic medical record system infra-
about a tenth of its budget.40 In addition, in a ran-
structure. Although much of the data required to
domized controlled trial, order entry was found to
implement significant clinical decision support is
already available in electronic form at many institu-
ment safe practices.42 One of the first of these practices
tions, the data are either not accessible or cannot be
will be the implementation of computerized physi-
brought together to be used in clinical decision sup-
cian order entry systems. Similarly, a recent Medicare
port because of format and interface issues. Existing
Patient Advisory Commission report suggested that
and evolving standards for exchange of information
that the Health Care Financing Administration con-
(HL7) and coding of this data are simplifying this
sider providing financial incentives to hospitals that
task. Correct and consistent identification of patients,
adopt physician order entry systems.43 The Agency
doctors, and locations is another area in which stan-
for Healthcare Research and Quality has received $50
dards are needed. Approaches to choosing which
million in funding to support error reduction
information should be coded and how to record a
research, including information technology–related
mixture of structured coded information and
strategies. California recently passed a law mandating
that non-rural hospitals implement computerizedphysician order entry or another application like it by
Some organizations have moved ahead with adopt-
2005.44 Clearly, many look to automation to play a
ing such standards on their own, and this can have
major role in the redesign of our systems.
great benefits. For example, a technology architectureguide was developed at Cedars-Sinai Medical Center
Recommendations
to help ensure that its internal systems and databasesoperate in a coherent manner. This has allowed them
Recommendations for using information technology
to develop what they call their “Web viewing sys-
to reduce errors fall into two categories—general
tem,” which allows clinicians to see nearly all results
suggestions that are relevant across domains, and
on an Internet platform. Many health care organiza-
very specific recommendations. It is important to rec-
tions are hamstrung, because they have implemented
ognize that these lists are not exhaustive, but they do
so many different technologies and databases that
contain many of the most important and best-docu-
mented precepts. Although many of these relate to
A second major hurdle is choosing the appropriate
the medication domain, this is because the best cur-
rules or guidelines to implement. Many organizations
rent evidence is available for this area; we anticipate
have not developed processes for developing and
that information technology will eventually be
implementing consensus choices in their physician
shown to be important for error reduction across a
groups. Once the focus has been determined, the
wide variety of domains, and some evidence is
organization must determine exactly what should be
already available for blood products, for example.45,46
done about the selected problem. Regulatory and
The strength of these recommendations is based on a
legal issues have also prevented vendors from pro-
standard set of criteria for levels of evidence.47 For
viding this type of content. Finally, despite good
therapy and prevention, evidence level 1a represents
precedents for delivering feedback to clinicians for
multiple randomized trials, level 1b is an individual
simple decision support, changing provider behavior
randomized trial, level 4 is case series, and level 5
for more complex aspects of care remains challenging. The National Picture General Recommendations
A national commitment to safer health care is devel-
Implement clinical decision support judiciously
oping. Although it is too soon to determine how it
(evidence level 1a). Clinical decision support can
will “play out” (the initial fixation on mandatory
clearly improve care,48 but it must be used in ways
reporting has been an unwelcome diversion, for
that help users, and the false-positive rate of active
example), it seems clear that many stakeholders have
suggestions should not be overly high. Such deci-
a real interest in improving safety. Doctors and other
sion support should be usable by physicians.
professionals are in the interesting position of being
Consider consequent actions when designing sys-
expected to be both leaders in this movement and the
tems (evidence level 1b). Many times, one action
recipients of its attention. Already a national coalition
implies another, and systems that prompt regard-
involving many of the leading purchasers, the
ing this can dramatically decrease the likelihood of
Leapfrog Group, which includes such companies as
General Motors and General Electric, have an-nounced their intention to provide incentives to hos-
Test existing systems to ensure that they actually
pitals and other health care organizations to imple-
catch errors that injure patients (evidence level 5).
Journal of the American Medical Informatics Association Volume 8 Number 4 Jul / Aug 2001
The match between the errors that systems detect
Specific Recommendations
and the actual frequency of important errors isoften suboptimal.
Implement provider order entry systems, especial-ly computerizing prescribing (evidence level 1b).
Promote adoption of standards for data and sys-
Provider order entry has been shown to reduce the
tems (evidence level 5). Adoption of standards is
serious medication error rate by 55 percent.20
critical if we are to realize the potential of infor-mation technology for error prevention. Standards
Implement bar-coding for, for example, medica-
for constructs such as drugs and allergies are espe-
tions, blood, devices, and patients (evidence level
4). In other industries, bar-coding has dramaticallyreduced error rates. Although fewer data are avail-
Develop systems that communicate with each
able for this recommendation in medicine, it is like-
other (evidence level 5). One of the greatest barri-
ly that bar-coding will have a major impact.52
ers to providing clinicians with meaningful infor-mation has been the inability of systems, such as
Use modern electronic systems to communicate
medication and laboratory systems, to readily
key pieces of asynchronous data (evidence level
exchange data. Such communication should be
1b). Timely communication of markedly abnormal
seamless. Adopting enterprise database standards
laboratory tests can decrease time to therapy and
the time patients spend in life-threatening condi-tions.
Use systems in new ways (evidence level 5). Elec-tronic records will soon facilitate new, sophisticated
Our hope is that these recommendations will be use-
prevention approaches, such as risk factor profiling
ful for a variety of audiences. Error in health care is a
and pharmacogenomics, in which a patient’s med-
pressing problem, which is best addressed by chang-
ications are profiled against their genetic makeup.
ing our systems of care—most of which involveinformation technology. Although information tech-
Measure and prevent adverse consequences (evi-
nology is not a panacea for this problem, which is
dence level 5). Information technology in general
highly complex and will demand the attention of
and clinical decision support in particular can cer-
many, it can play a key role. The informatics commu-
tainly have perverse and opposite consequences;
nity should make it a high priority to assess the
continuous monitoring is essential.50 However,
effects of information technology on patient safety.
such monitoring has often not been carried out. Itshould also be routine to measure how often rec-
ommendations are presented and how often sug-
1. Kohn LT, Corrigan JM, Donaldson MS (eds). To Err Is Human:
gestions are accepted and to have some measures
Building a Safer Health System. Washington, DC: National
2. McDonald CJ, Weiner M, Hui SL. Deaths due to medical errors
Make existing quality structures meaningful (evi-
are exaggerated in Institute of Medicine report. JAMA.
dence level 5). Quality measurement and improve-
ment groups are often suboptimally effective.
3. Leape LL. Institute of Medicine medical error figures are not
Increasing the use of computerization should
exaggerated [comment]. JAMA. 2000;284:95–7.
4. Leape LL, Brennan TA, Laird NM, et al. The nature of adverse
make it dramatically easier to measure quality
events in hospitalized patients: results from the Harvard
continually. Such information must then be used
Medical Practice Study II. N Engl J Med. 1991;324:377–84.
5. Gurwitz JH, Field T, Avorn J, et al. Incidence and preventability of
adverse drug events in nursing homes. Am J Med. 2000;109:87–94.
Improve regulation and remove disincentives for
6. Bates DW, Boyle DL, Vander Vliet MB, Schneider J, Leape LL.
vendors to provide clinical decision support (evi-
Relationship between medication errors and adverse drug
dence level 5). The regulation relating to informa-
events. J Gen Intern Med. 1995;10:199–205.
7. Rasmussen J. Human errors: a taxonomy for describing
tion technology is hopelessly outdated and is cur-
human malfunction in industrial installations. J Occup Accid.
rently being revised to address such issues as pri-
vacy in the electronic world.51 One issue that
8. Reason J. Human Error. Cambridge, UK: Cambridge
relates to error in particular is that vendors, with
some cause, fear being sued if they provide action-
9. Norman DA. The Design of Everyday Things. New York:
oriented clinical decision support. Thus, the sup-
10. Senders J, Moray N. Human Error: Cause, Prediction and
port either is not provided or is watered down.
Reduction. Mahwah, NJ: Lawrence Erlbaum, 1991.
11. Testimony of the Three Mile Island Operators. United States
President's Commission on the Accident at Three Mile Island, vol
34. Shabot M, LoBue M, Chen J. Wireless clinical alerts for critical
1. Washington, DC: U.S. Government Printing Office, 1979:138.
medication, laboratory and physiologic data. Proceedings of
12. Macklis RM, Meier T, Weinhous MS. Error rates in clinical
the 33rd Hawaii International Conference on System
radiotherapy. J Clin Oncol. 1998;16:551–6.
Sciences (HICSS); Jan 4–7, 2000; Maui, Hawaii [CD-ROM].
13. Leape LL, Bates DW, Cullen DJ, et al. Systems analysis of
Washington, DC: IEEE Computer Society, 2000.
adverse drug events. ADE Prevention Study Group. JAMA.
35. Kuperman G, Sittig DF, Shabot M, Teich J. Clinical decision
support for hospital and critical care. J HIMSS. 1999;13:81–96.
14. Brennan TA, Leape LL, Laird N, et al. Incidence of adverse
36. Institute for Safe Medication Practices. Over-reliance on com-
events and negligence in hospitalized patients: results from the
puter systems may place patients at great risk. ISMP Medication
Harvard Medical Practice Study I. N Engl J Med. 1991;324:370–6.
Safety Alert, Feb 10, 1999. Huntingdon Valley, Pa.: ISMP, 1999.
15. Barker KN, Allan EL. Research on drug-use-system errors. Am
37. Bruskin Goldring Research. A Study of Medication Errors and
J Health Syst Pharm. 1995;52:400–3.
Specimen Collection Errors. Commissioned by BD (Becton-
16. Classen DC, Pestotnik SL, Evans RS, Burke JP. Computerized
Dickinson) and College of American Pathologists. Feb 1999.
surveillance of adverse drug events in hospital patients.
Available at http://www.bd.com/bdid/whats_new/survey.
17. Jha AK, Kuperman GJ, Teich JM, et al. Identifying adverse
38. The Advisory Board Company. Prescription for change:
drug events: development of a computer-based monitor and
toward a higher standard in medication management. Wash-
comparison to chart review and stimulated voluntary report. J
Am Med Inform Assoc. 1998;5(3):305–14.
39. Glaser J, Teich JM, Kuperman G. Impact of information events
18. Gandhi TK, Seger DL, Bates DW. Identifying drug safety issues—
on medical care. Proceedings of the 1996 HIMSS Annual
from research to practice. Int J Qual Health Care 2000;12:69–76.
Conference. Chicago, Ill.: Healthcare Information and
19. Karson AS, Bates DW. Screening for adverse events. J Eval
Management Systems Society, 1996:1–9.
40. Sarasota Memorial Hospital documents millions in expected
20. Bates DW, Leape LL, Cullen DJ, et al. Effect of computerized
cost savings, reduced LOS through use of Eclipsys’ Sunrise
physician order entry and a team intervention on prevention
Clinical Manager [press release]. Delray Beach, Fla.: Eclipsys
of serious medication errors. JAMA. 1998;280(15):1311–6.
Corporation; Oct 11, 1999. Available at: http://www.
21. Bates DW, Cullen D, Laird N, et al. Incidence of adverse drug
events and potential adverse drug events: implications for
41. Tierney WM, Miller ME, Overhage JM, McDonald CJ.
Physician inpatient order writing on microcomputer worksta-
22. Bates DW, Miller EB, Cullen DJ, et al. Patient risk factors for
tions: effects on resource utilization. JAMA. 1993;269:379–83.
adverse drug events in hospitalized patients. Arch Intern
42. Fischman J. Industry Preaches Safety in Pittsburgh. U.S. News
23. Evans RS, Pestotnik SL, Classen DC, et al. A computer-assist-
43. Medicare Payment Advisory Commission. Report to the
ed management program for antibiotics and other anti-infec-
Congress: Selected Medicare Issues, Jun 1999. Available at:
tive agents. N Engl J Med. 1998;338:232–8.
http://www.medpac.gov/html/body_june_report.html.
24. Classen DC, Evans RS, Pestotnik SL, et al. The timing of pro-
phylactic administration of antibiotics and the risk of surgical-
44. California Senate Bill No. 1875. Chapter 816, Statutes of 2000.
wound infection. N Engl J Med 1992;326:281–6.
45. Lau FY, Wong R, Chui CH, Ng E, Cheng G. Improvement in
25. Tate K, Gardner RM, Scherting K. Nurses, pagers and patient
transfusion safety using a specially designed transfusion
specific criteria: three keys to improved critical value report-
wristband. Transfus Med.2000;10(2):121–4.
ing. Proc Annu Symp Comput Appl Med Care. 1995;19:164–8.
46. Blood-error reporting system tracks medical mistakes [press
26. Tate K, Gardner RM, Weaver LK. A computerized laboratory
release]. Dallas, Tex: The University of Texas Southwestern
alerting system. MD Comput. 1990;7:296–301.
Medical Center at Dallas; Nov 22, 1999. Available at
27. Rind D, Safran C, Phillips RS, et al. Effect of computer-based
http://irweb.swmed.edu/newspub. Accessed Mar 12, 2001.
alerts on the treatment and outcomes of hospitalized patients.
47. Centre for Evidence-based Medicine. Levels of evidence and
grades of recommendation; Sep 8, 2000. Available at:
28. Kuperman G, Boyle D, Jha AK, et al. How promptly are inpa-
http://cebm.jr2.ox.ac.uk/docs/levels.html. Accessed Mar 12,
tients treated for critical laboratory results? J Am Med Inform
48. Haynes RB, Hayward RS, Lomas J. Bridges between health
29. Bradshaw K. Computerized alerting system warns of life-threatening
care research evidence and clinical practice. J Am Med Inform
events. Proc Annu Symp Comput Appl Med Care. 1986;10:403.
30. Bradshaw K. Development of a computerized laboratory alert-
49. Overhage JM, Tierney WM, Zhou X, McDonald CJ. A ran-
ing system. Comput Biomed Res. 1989;22:575–87.
domized trial of “corollary orders” to prevent errors of omis-
31. Shabot M, LoBue M, Leyerle B. Inferencing strategies for auto-
sion. J Am Med Inform Assoc. 1997;4:364–75.
mated alerts on critically abnormal laboratory and blood gas
50. Miller R, Gardner RM. Summary recommendations for
data. Proc Annu Symp Comput Appl Med Care. 1989;13:54–7.
responsible monitoring and regulation of clinical software sys-
32. Shabot M, LoBue M, Leyerle B. Decision support alerts for
tems. Ann Intern Med. 1997;127:842–5.
clinical laboratory and blood gas data. Int J Clin Monit
51. Gostin LO, Lazzarini Z, Neslund VS, Osterholm MT. The pub-
lic health information infrastructure: a national review of the
33. Shabot M, LoBue M. Real-time wireless decision support alerts
law on health information privacy. JAMA.1996;275:1921–7.
on a palmtop PDA. Proc Annu Symp Comput Appl Med Care.
52. Bates DW. Using information technology to reduce rates of
medication errors in hospitals. BMJ. 2000;320:788–91.
Balancing Moods Through Lifestyle Choices Mood disorders such as depression and anxiety may be related to a number of different causes. Frequently, physicians prescribe drugs such as Prozac and Wellbutrin to alter brain chemistry in an attempt to normalize moods. While such prescriptions may be life-saving in certain cases, many doctors agree that these drugs are over-used and may have seriou
Question Paper Preview Question Paper Name: Assistant Prof. General Surgery - 2012 Creation Date: 2012-06-28 12:19:42.0 Cut Off: 0 Duration: 120 Status: Sealed Section 1 Question id : 147163 (Correct + 1.0 , Wrong - 0.33) Which one of the following is the ideal treatment of Alkaline Reflux Gastritis after Billroth II gastrectomy 1. Conversion of Billroth II to B
 A system analysis of a large series of serious medica-
in a controlled trial that computerized physician
tion errors (those that either might have or did cause
order entry systems resulted in a 55 percent reduction
harm)13 identified 16 major types of system failures
in serious medication errors. In another time series
associated with these errors. Of these system failures,
study,22 this group found an 83 percent reduction in
all of the top eight could have been addressed by bet-
the overall medication error rate, and a 64 percent
reduction even with a simple system. Evans et al.23have also demonstrated that clinical decision support
Currently, the clinical systems in routine use in
can result in major improvements in rates of antibiot-
health care in the United States leave a great deal to
ic-associated adverse drug events and can decrease
be desired. The health care industry spends less on
costs. Classen et al.24 have also demonstrated in a
information technology than do most other informa-
series of studies that nosocomial infection rates can be
tion-intensive industries; in part as a result, the
dream of system integration been realized in feworganizations. For example, laboratory systems do
Another class of clinical decision support is comput-
not communicate directly with pharmacy systems.
A system analysis of a large series of serious medica-
in a controlled trial that computerized physician
tion errors (those that either might have or did cause
order entry systems resulted in a 55 percent reduction
harm)13 identified 16 major types of system failures
in serious medication errors. In another time series
associated with these errors. Of these system failures,
study,22 this group found an 83 percent reduction in
all of the top eight could have been addressed by bet-
the overall medication error rate, and a 64 percent
reduction even with a simple system. Evans et al.23have also demonstrated that clinical decision support
Currently, the clinical systems in routine use in
can result in major improvements in rates of antibiot-
health care in the United States leave a great deal to
ic-associated adverse drug events and can decrease
be desired. The health care industry spends less on
costs. Classen et al.24 have also demonstrated in a
information technology than do most other informa-
series of studies that nosocomial infection rates can be
tion-intensive industries; in part as a result, the
dream of system integration been realized in feworganizations. For example, laboratory systems do
Another class of clinical decision support is comput-
not communicate directly with pharmacy systems.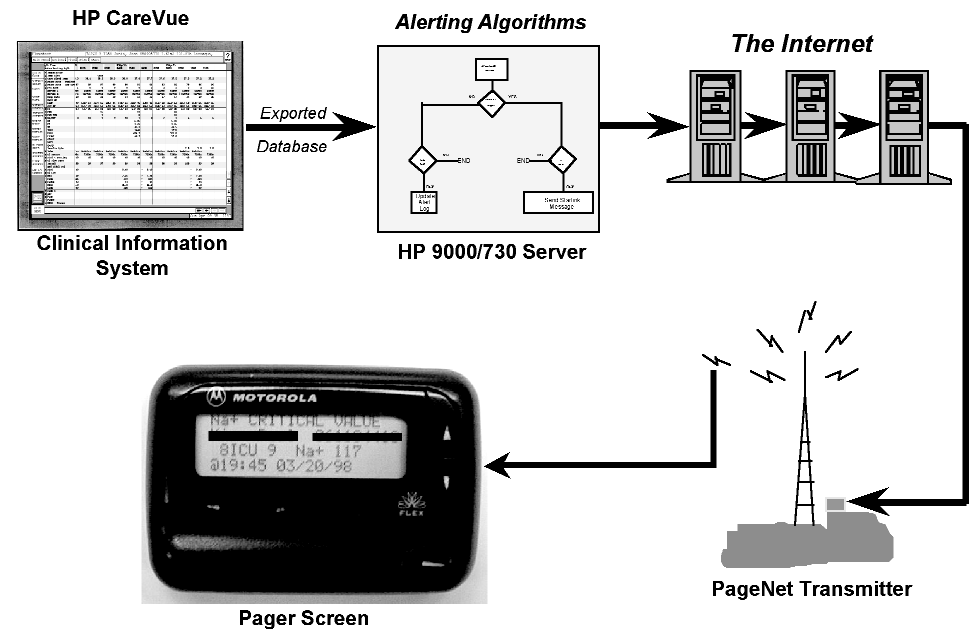 Journal of the American Medical Informatics Association Volume 8 Number 4 Jul / Aug 2001
2 Wireless alerting system. In the Cedars-Sinai system, alerts are initially detected by the clinical system, then
Journal of the American Medical Informatics Association Volume 8 Number 4 Jul / Aug 2001
2 Wireless alerting system. In the Cedars-Sinai system, alerts are initially detected by the clinical system, then