Pulsed Short Wave Effect in Pain and Function in Patients with Knee Osteoarthritis Post-graduate Professor, Irmandade da Santa Casa de Misericórdia de São Paulo, São Paulo,Brazil; Nucleus of support to research in analysis of the movement (NAPAM);Vanessa Ovanessian, Ph.T
Post-graduate student, Irmandade da Santa Casa de Misericórdia de São Paulo (ISCMSP),São Paulo, Brazil;Ronaldo Alves da Cunha, Ph.T
Post-graduate student, Irmandade da Santa Casa de Misericórdia de São Paulo (ISCMSP),São Paulo, Brazil;Ziqui Jacob Filho, Ph.T
Post-graduate student, Irmandade da Santa Casa de Misericórdia de São Paulo (ISCMSP),São Paulo, Brazil;Cláudio Cazarini Júnior, Ph.T
Post-graduate student, Irmandade da Santa Casa de Misericórdia de São Paulo (ISCMSP),São Paulo, Brazil;Fabio Albanez Rienzo, Ph.T
Physical therapist specialist, Institute of Orthopaedic and Traumatology of the University of Sao Paulo - USP, São Paulo, Brazil;Aline Almeida Centini, Ph.T
Physical therapist, Institute of Orthopaedic and Traumatology of the University of Sao Paulo -USP, São Paulo, BrazilKEY WORDS: Osteoarthritis; Pulsed
osteoarthritis and were submitted to 17and 33 KJ PSW doses and evaluated bya Lequesne’s Algofuncional
ABSTRACT
Scale, visual analogical scale (VAS), and
osteoarthritis patient’s treatment.
this condition, the aim of this study was
osteoarthritis. Eighty-four patients that
with the control group. A significant dif-
The Journal of Applied Research • Vol. 8, No. 3, 2008
Figure 1: Diagram block-type delineating the proposed study.
trol. For knee flexion, there were statisti-
world’s adult population over the age of
is augmenting as the population ages.
Among all of the joints, the knee is usu-
and control groups. Significant therapeu-
covered, however, it is frequently associ-
alleviate pain, improve function, prevent
INTRODUCTION
disease’s progression.4,13 Many interven-
in the progressive loss of joint cartilage
associated with sclerosis of the subchon-
therapy that use specific techniques such
dral bone, which, in many cases, leads to
phytes. In addition to joint alterations,
cal therapy, electromagnetic radiation is
restricted movement of the affected site,
Vol. 8, No. 3, 2008 • The Journal of Applied Research
* statistically significant difference in relation to the control group (p < 0.05)** statistically significant difference in relation to the c
Figure 2: Comparison between the (F-I)/I indexes obtained from the Lequesne Questionnaire in
mine if there is any difference in efficacy
emphasizing the effects of incrementalcellular tropism.6,7
Patients
tion are: to increase local cell activity,
rin and collagen deposits, and aid in tis-
greater quantity.4,9,17,22 These conflicting
patients in the control group (60 years ±
(63 year ± 09); and 22 patients in group
trolled study aims to evaluate the effects
The Journal of Applied Research • Vol. 8, No. 3, 2008
** statistically significant difference in relation to the control and placebo group (p < 0.05)
Figure 3: Comparison between the (F-I)/I indexes obtained by the Lysholm scale in the 4 studied
the age of 40 years, having a diagnosis of
viously established, and patient selection
were going to participate in the study.
groups and were randomly distributed.
The same “blind examiner” was respon-
associated diseases of the locomotivesystem such as fibromyalgia; traumatic
Intervention
lesions of the meniscus and/or ligaments;
pacemakers; or a history of tumors. 4,13,17
applicationS of PSW per week for 3months, totaling 9 sessions. The instru-
Procedures Vol. 8, No. 3, 2008 • The Journal of Applied Research
Table 1: Characterization of the 4 studied groups
Evaluations
a pulse frequency (f) of 145 Hz in order
knee was kept in a semi flexion at 20º.
application, totaling 17 KJ of energy. To
and 4 questions about daily activities.
calculate these energy values, the follow-
The Journal of Applied Research • Vol. 8, No. 3, 2008
Table 2: Results of the mean ± standard deviation and median of the (F-I)/I index of the
tic result. On the other hand, the final,
evaluation divided by the initial evalua-
represent a worse therapeutic result. Statistical analysis
results of means, ± standard deviations,
software package GraphPad Instant wasused to process the values obtained
Lequesne Algofunctional Questionnaire
In the analysis of this questionnaire, the
± 0.2 (0.06); placebo group -0.08 ± 0.27
(-0.12); group I -0.31 ± 0.13 (-0.31) and
test for parametric samples was used.
group II -0.27 ± 0.37 (-0.33), with a sig-
Kruskal-Wallis test and non paired t-test
group (p < 0.05), group I (p < 0.0001)
for non-parametric samples were used.
and group II (p < 0.001) when compared
to the control group. A significant differ-
Lysholm Scale
In the analysis of this scale, the obtained
values were: control group 0.02 ± 0.27 (-
the final evaluations due to lack of regu-
0.04); placebo group 0.28 ± 0.55 (0.21);
larity, and were automatically excluded.
group I of 0.64 ± 0.57 (0.51); and group
II of 0.76 ± 0.86 (0.52), with a significant
difference between group I (p < 0.0001)
and group II (p < 0.001) when compared
to the control group. Significant differ-
(p < 0.05) and II (p < 0.05) when com-
pared to the placebo group (Figure 3). Knee flexion Vol. 8, No. 3, 2008 • The Journal of Applied Research
* statistically significant difference in relation to the control group (p < 0.05)
Figure 4: Comparison between the (F-I)/I indexes obtained by knee goniometry in the 4 studied
(0.01); group I of 0.05 ± 0.10 (0.02); and
placebo group (p < 0.05), group I (p <
goniometric measures of knee flexionand VAS. The questionnaires selected
Visual Analogical Scale
trol group -0.02 ± 0.34 (-0.04); placebo
group -0.21 ± 0.38 (-0.22); group I -0.18
± 0.30 (-0.19); and group II with -0.42 ±
higher incidence of OA in this group.
0.34 (-0.45). Group II presented a statis-
DISCUSSION The Journal of Applied Research • Vol. 8, No. 3, 2008
*** statistically significant difference in relation to the control group and group I (p < 0.05)
Figure 5: Comparison between the (F-I)/I indexes obtained by VAS in the 4 studied groups.
group. In the present study, very similar
previously, yet with satisfactory results.
with the use of PSW for OA of the knee.
results compared to the control group.
however, statistical significance was not
active groups and one control group.
the literature. In order to obtain thera-
little or no anti-inflammatory effects and
ed.4,13,21 Conversely, in the present inves-
Vol. 8, No. 3, 2008 • The Journal of Applied ResearchCONCLUSION
placebo group. Because a significant dif-
alleviating pain and providing functional
the Lequesne and Lysholm scales, thegroups treated with 17 and 33 KJ pre-
Acknowledgment
for Scientific Publications of Santa Casa
Sciences for the editorial assistance.
and functional improvement. The goal ofthis study was not to observe physiologi-
REFERENCES
possible effects reported in the literature
level laser therapy with location-specific
doses for pain from chronic joint disorders. Aust.J.Physiother. 2003;49:107-116.
fluid, relaxation of muscles, and inflam-
Bjordal JM, Johnson MI, Lopes-Martins RA,
matory control of the reactive synovitis.
Bogen B, Chow R, Ljunggren AE. Short-term
osteoarthritic knee pain. A systematic review
controlled trials A systematic review and
trolled trials. BMC. Musculoskelet Disord
group, without any difference foundbetween the active groups and the
osteoarthritis. Am J Sports Med 1997;25:873-
Callaghan MJ, Whittaker PE, Grimes S, Smith
knee osteoarthritis using radioleucoscintigra-
phy: a randomised, double blind, controlled
trial. Joint Bone Spine 2005;72:150-155.
Evans P. The healing process at cellular level:
a review. Physiotherapy 1980;66:256-259.
Distribution in the Lower Leg from Pulsed
to point out that a prolonged application
time is not necessary, since a total time
Treatments. J Athl Train 2000;35:50-55.
window recommended in the literature.
através da aplicação de ondas curtas pulsado
atérmico: dose ideal e tempo de aplicação.
Radiographic evaluation of osteoarthritis. Radiol Clin N Am. 2004; 42:11-41,v.
py during the physical therapy treat-ment. The inclusion of exercise and
Hill J, Lewis M, Mills P, Kielty C. Pulsed
fibroblast proliferation. Arch.Phys.Med.The Journal of Applied Research • Vol. 8, No. 3, 2008
10. Hoppenfeld S. Propedêutica Ortopédica: col-
17. Moffett JA, Richardson PH, Frost H, Osborn
A. A placebo controlled double blind trial to
evaluate the effectiveness of pulsed short
wave therapy for osteoarthritic hip and knee
11. Jamtvedt G, Dahm KT, Christie A, Moe RH,
Physical therapy interventions for patients
18. Nadasdi M. Inhibition of experimental arthri-
with osteoarthritis of the knee: an overview
tis by athermic pulsating short waves in rats.
of systematic reviews. Phys Ther 2008;88:123-
19. Peccin MS, Ciconelli R, Cohen M.
12. Kitchen S, Partridge C. Review of shortwave
Questionário específico para sintomas. do
diathermy continuous and pulsed patterns.
joelho “Lysholm Knee Scoring Scale” –
Physiotherapy 1992;78:243-252.
tradução e validação para a língua portugue-
sa. Acta Ortop Bras 2006;14:268-272.
13. Laufer Y, Zilberman R, Porat R, Nahir AM.
20. Shields N, O’Hare N, Boyle G, Gormley J.
osteoarthritis of the knee: a placebo-con-
control procedure for short-wave diathermy
trolled double-blind clinical trial. Clin
units. Med Biol Eng Comput 2003;41:62-68.
21. Svarcova J, Trnavsky K, Zvarova J. The influ-
ence of ultrasound, galvanic currents and
arthritis of the knee. PhysiotherapyRheumatol Suppl 1987;67:83-85.
22. Trock DH, Bollet AJ, Dyer RH Jr, Fielding
15. Marques AP, Kondo A. A fisioterapia na
osteoartrose: uma revisão da literatura. Rev
trial of the clinical effects of pulsed electro-
magnetic fields in osteoarthritis. J Rheumatol
16. Marx FC, Oliveira LM, Bellini CG, Ribeiro
MCC. Tradução e validação cultural do ques-
23. Tuzun EH, Otman S, Kirdi N. Comparison of
osteoartrite de joelhos e quadris para a língua
diathermy in knee osteoarthritis. The Pain
portuguesa. Rev Bras Reumatol 2006;46:253-
24. Van Nguyen JP, Marks R. Pulsed electromag-
netic fields for treating osteoarthritis,
Physiotherapy 2002;88:458-470. Vol. 8, No. 3, 2008 • The Journal of Applied Research
Preise Preis der Menopausengesellschaft deutschsprachiger Länder 1994 in Baden bei Wien 9.9.1994 J.Neuwinger, I.Mück, J.Esper und L.Wildt: Selektive Behandlung von Hitzewallungen mit 17 alpha Estradiol, einem Estradiol Epimer ohne klassische Estrogenwirkung. Dissertation Neuwinger J.: Untersuchung zur Digoxintherapie unter Captopril-Komedikation bei gesunden und herzinsuffizienten Patienten. Me
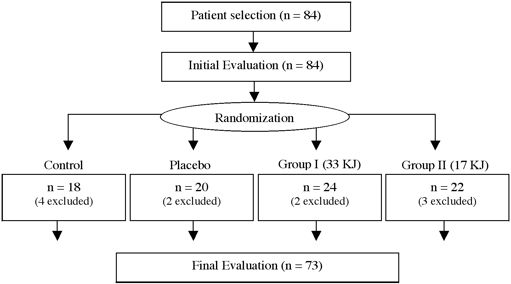 Figure 1: Diagram block-type delineating the proposed study.
Figure 1: Diagram block-type delineating the proposed study.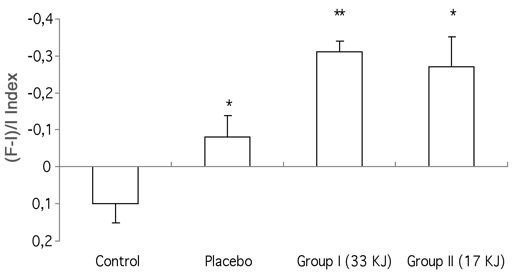 * statistically significant difference in relation to the control group (p < 0.05)** statistically significant difference in relation to the c
Figure 2: Comparison between the (F-I)/I indexes obtained from the Lequesne Questionnaire in
mine if there is any difference in efficacy
emphasizing the effects of incrementalcellular tropism.6,7
Patients
* statistically significant difference in relation to the control group (p < 0.05)** statistically significant difference in relation to the c
Figure 2: Comparison between the (F-I)/I indexes obtained from the Lequesne Questionnaire in
mine if there is any difference in efficacy
emphasizing the effects of incrementalcellular tropism.6,7
Patients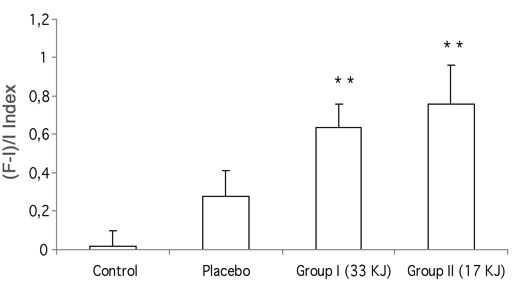 ** statistically significant difference in relation to the control and placebo group (p < 0.05)
Figure 3: Comparison between the (F-I)/I indexes obtained by the Lysholm scale in the 4 studied
the age of 40 years, having a diagnosis of
viously established, and patient selection
were going to participate in the study.
** statistically significant difference in relation to the control and placebo group (p < 0.05)
Figure 3: Comparison between the (F-I)/I indexes obtained by the Lysholm scale in the 4 studied
the age of 40 years, having a diagnosis of
viously established, and patient selection
were going to participate in the study.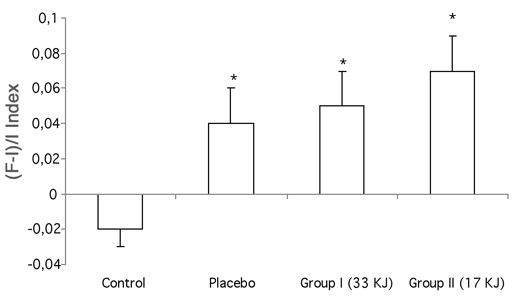 * statistically significant difference in relation to the control group (p < 0.05)
Figure 4: Comparison between the (F-I)/I indexes obtained by knee goniometry in the 4 studied
(0.01); group I of 0.05 ± 0.10 (0.02); and
placebo group (p < 0.05), group I (p <
goniometric measures of knee flexionand VAS. The questionnaires selected
Visual Analogical Scale
* statistically significant difference in relation to the control group (p < 0.05)
Figure 4: Comparison between the (F-I)/I indexes obtained by knee goniometry in the 4 studied
(0.01); group I of 0.05 ± 0.10 (0.02); and
placebo group (p < 0.05), group I (p <
goniometric measures of knee flexionand VAS. The questionnaires selected
Visual Analogical Scale 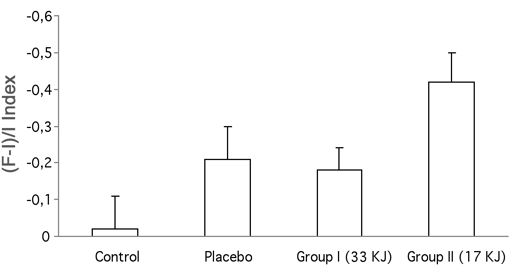 *** statistically significant difference in relation to the control group and group I (p < 0.05)
Figure 5: Comparison between the (F-I)/I indexes obtained by VAS in the 4 studied groups.
*** statistically significant difference in relation to the control group and group I (p < 0.05)
Figure 5: Comparison between the (F-I)/I indexes obtained by VAS in the 4 studied groups.