http://mutagens.co.in PROTHROMBIN TIME & INTERNATIONAL NORMALIZED RATIO IN PEDIATRIC LIVER DISEASE
1Senior Resident, Department Of Pediatrics ,
VSS Medical College & Hospital, Burla, Sambalpur, Odisha
2Associate Professor, Department Of Pediatrics ,
VSS Medical College & Hospital, Burla, Sambalpur, Odisha
3Senior Resident, Department Of Pediatrics ,
VSS Medical College & Hospital, Burla, Sambalpur, Odisha
Abstract
As we all know that Prothrombin Time (PT) / International Normalized Ratio(INR) is used to assess the extrinsic and common pathway of blood coagulation particularly Factor VII estimation. In the present scenario all the laboratories are doing PT /INR estimation & we all are interpreting the value in the management of patients irrespective of the nature of liver disease. The laboratories doing PT /INR estimation is for monitoring oral anticoagulant (Warfarin) therapy not for liver disease per se .We serially observed the 20 liver disease patients for last six months. Some of them (12) having PT/INR value within normal range & some of them (8) having very high value of PT/INR .These 8 patients having very high PT/INR value improves without any interventions showing the falsely high value of PT/INR .We just want to reflect that PT/INR estimation for liver disease per se & for oral anticoagulation therapy monitoring are two different thing and don’t be panic at first viewing of such very high PT/INR value in liver disease patients. Key words: Prothrombin Time(PT), International Normalized Ratio(INR), International Sensitivity Index(ISI), International Sensitivity Index Liver Disease (ISI LD), Warfarin, LFT(Liver Function Test).
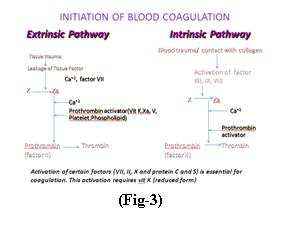
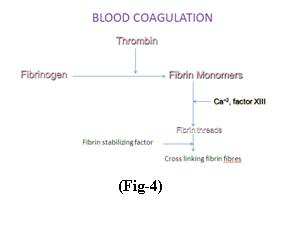
Date of Online: 28-12-2013 INTRODUCTION Before explaining the theme we just refreshing the steps of hemostasis1. There are three phases of hemostasis given in fig-12 1.Vascular spasm or vasoconstriction (smooth muscle of tunica media contract) The role of vasoconstriction is to reduce blood loss & the injured endothelia get sticky, contact each other from opposing ends and seal off the blood vessel form both ends. 2. Platelet plug formation or platelet aggregation (Positive feed-back loop) The role of the platelet aggregation or plug is to physically seals the broken blood vessel, actin- myosin complex in the aggregated platelets contract to compact the plug,vasoconstrictors are released from plug: serotonin, epinephrine, thromboxane A2, chemicals are released from plug to stimulate coagulation. 3. Blood coagulation/clotting (Fig-2 describes the steps of blood coagulation3) The transformation of blood from a liquid into a solid gel, formed on the top of the platelet plug, strengthens the platelet plug. Fig-3/44 describes it elaborately .
Events after blood clotting1 1.Clot retraction: Platelets contract, squeezing serum from the clot.Serum:plasma without clotting proteins 2. Blood vessel repair: Platelet-derived growth factor stimulates rebuilding the wall of the blood vessel. 3. Fibrinolysis After repair the blood clot is removed. Done by the fibrin digesting enzyme: plasmin.Plasminogen (inactive) → → plasmin(active). The prothrombin time was discovered by Dr Armand Quick5 and colleagues in 1935, and a second method was published by Dr Paul Owren, also called the "p and p" or "prothrombin and proconvertin" method. The INR (also known as standardised prothrombin time) was introduced in the early 1960s, by Dr. Jack Hirsh6 and colleagues at McMaster University School of Medicine, when it turned out that
Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246 ISSN 2320-1355
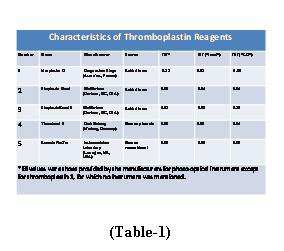
there was a large degree of variation between the various prothrombin time assays, a discrepancy mainly due to problems with the purity of the thromboplastin (tissue factor) concentrate. The INR became widely accepted worldwide, especially after endorsement by the World Health Organization. A revised international procedure for standardization of the prothrombin time (PT) in anticoagulant control was accepted by the international committees7 in 1941 and approved by the World Health Organization8. International Normalized Ratio (INR), which standardizes prothrombin time (PT) during oral anticoagulation, has been extended to standardize PT in liver diseases and is included in prognostic models such as the Model for End stage Liver Disease (MELD)9 introduced in 1960. INR or standardized prothrombin time, as the name suggest needs a detailed clarification of PT(prothrombin time). The PT test is used to monitor patients taking certain medications as well as to help diagnose clotting disorders. A sample of the patient's blood is obtained by venipuncture. The blood is decalcified (by collecting it into a tube with oxalate or citrate ions) to prevent the clotting process from starting before the test. The blood cells are separated from the liquid part of blood (plasma) by centrifugation. The PT test is performed by adding the patient's plasma to some source of Tissue Factor or factor III(e.g.: a protein, thromboplastin, from homogenized brain tissue10) that converts prothrombin to thrombin (Fig-5). The term thromboplastin refers to a complex mixture of tissue factor and phospholipids prepared from tissue extracts of animal or human origin. The mixture is then kept in a warm water bath at 37°C for one to two minutes. Calcium chloride (excess quantities of ionized calcium) is added to the mixture in order to counteract the sodium citrate and allow clotting to start. The test is timed from the addition of the calcium chloride until the plasma clots. This time is called the Prothrombin Time. PT is the time taken for clotting of citrated plasma after the addition of Ca+2 & standardized reference thromboplastins, it is expressed as ratio(PT ratio). PT ratio is PT of Pt/PT of a pool of plasma from healthy subjects on no medication. Depending upon the variability of thromboplastins, different results obtained in different laboratories. So to standardize PT measurement Internationally ,each thromboplastin is assigned with a ISI and Pt’s PT is expressed as INR11where INR = (PT Ratio)ISI . ISI(International Sensitivity Index)12 is supplied by the manufacturer of the test reagent & varies upon test reagent and instrument. It is the relative sensitivity of PT [determined from a given batch(pool of Pt. in laboratories) of thromboplastin] to decreases in the Vit. K dependent coagulation factors in comparison with a WHO human thromboplastin standard. The ISI is a numerical value that reflects the responsiveness of a given thromboplastin to reduction of the vitamin K–dependent coagulation factors13. If the INR is outside the target range, a high INR indicates a higher risk of bleeding, while a low INR suggests a higher risk of developing a clot. Reagents with low ISI are more sensitive to effect of Vit. K antagonist i.e.,PT is prolonged to a greater extent than to a less sensitive reagents with high ISI14 . However, mechanisms of PT prolongation in liver diseases(DECREASE SYNTHESIS OF FACTORII/VII/IX/X ) differ from those involved in oral anticoagulation(INHIBITION OF VIT-K REDUCTION), and the thromboplastin reagents differ in their sensitivities to these 2 mechanisms.Some laboratories hypothesized that the use of plasmas of patients with liver disease instead of plasmas from patients on oral anticoagulation in the calibration model for thromboplastins15. Calibration Procedure of Thromboplastins for the Definition of the Parameter ISI“LD”. Calibration was performed according to the WHO guidelines16 for thromboplastins and plasma used to control oral anticoagulant therapy, with the following differences: the use of frozen instead of fresh plasmas and the use of plasmas from patients with liver disease instead of plasmas from patients on stable oral anticoagulation but till now no definitive ISI value for liver disease is available. Characteristics of different Thromboplastin Reagents are given in Table-117 Time required for clotting of plasma after adding thromboplastin is called PT(N =12-13sec,>16sec = abnormal, ≥ 20sec = definite abnormality)18.Blood collected must be used with in 2hr if at room temp or with in 4 hr if cold & should be frozen if not used with in this period. Frozen sample should be thawed at 370C before use.PT measures the activity of factor I, II, V, VII, X. PT dose not prolong until the conc. of these factor is <30% or until fibrinogen <100mg/dl. Isolated PT prolongation indicates factor VII deficiency. Normal value of ISI is 1 to 218. Normal value of INR is 0.8 to 1.2 http://mutagens.co.in242 Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246 ISSN 2320-1355
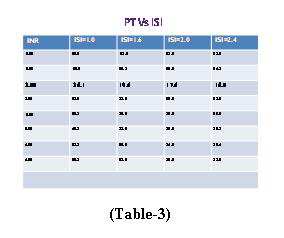
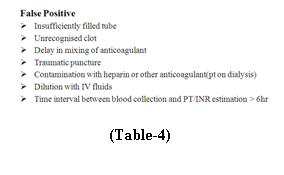
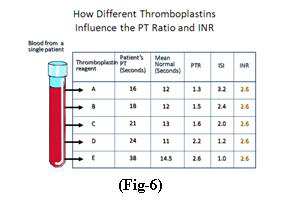
without anticoagulation,2 to 3 with anticoagulation, 2.5 to 3.5 with intense anticoagulation18.Table-2 demonstrates the PT values in various age groups19 . PATIENTS AND METHOD: Twenty (20) cases were included in this study review in last six months . Inclusion criteria being children admitted to our hospital for liver diseases not taking any anticoagulation. Detailed clinical, hematological & LFT evaluation was done for every patients. Out of 20, 12 patients found to have normal PT / INR (mean=12.37±0.88sec) values and 8 patients were having PT / INR values very high(mean=20.13 ±1.78 sec) reflecting very severe liver failure. But these 8 patients though having high PT / INR, surprisingly improves without any active interventions as the parents were extremely poor. Thanks to the God for their survival, but the thing is to think that was their PT / INR reports were correct, if yes then how they survived & if no then what is the fact. Calculation of mean PT / INR was done by SPSS v 16 software. DISCUSSION: Out of 20 liver disease patients, 12 having PT / INR values normal & 8 patients showed high PT / INR values .This differences most probably due to ISI values20 used by the laboratories or lessly due to false positive21 / false negative22 results. Table-3 shows how PT / INR values differ according to various ISI values. This table demonstrate at a constant INR value PT value decreases as ISI values increases.Fig-6 demonstrate how different thromboplastins influence the PT ratio and INR. Table-4/5 shows various causes of false positive or negative PT / INR. As the thromboplastins are supplied by different laboratories, the ISI values will be different but unfortunately the ISI values used by different laboratories is for monitoring oral anticoagulant therapy & till date ISI for liver disease(ISI LD) is not available, the PT / INR estimation we are sending is not the ideal one. CONCLUSION:
PT ESTIMATION WITHOUT INR IS MEANINGLESS INR FOR LIVER DISEASE IS DIFFERENT FROM THAT OF INR FOR
TILL DATE INR FOR LIVER DISEASES NOT AVAILABLE(UNDER RESEARCH) INR CAN BE USED FOR APTT ESTIMATION , BUT INR MEANS PT ESTIMATION ISI IS VERY IMPORTANT IN CALCULATION OF INR ISI IS DIFFERENT FOR LIVER DISEASE & ANTICOAGULATION THERAPY WE MUST CHECK THE ISI VALUE BEFORE INR ESTIMATION
ACKNOWLEDGEMENT: The authors would like to thank H.O.D.Pediatrics,V.S.S.MC and the participating clinicians for this study review and Cyber Zone for assistant with the draft manuscript preparation. http://mutagens.co.in243 Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246 ISSN 2320-1355 http://mutagens.co.in244 Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246 ISSN 2320-1355 REFERENCES: 1. BIOL 2305/ 2101 Human Physiology, CH-11-Blood Clotting , p 6. 2. http://www.womens-health-advice.com/heart-disease/coagulation.html. 3. Pallister CJ and Watson MS (2010). Haematology. Scion Publishing. pp. 336–347. 4. Garcia-Alamino JM, Ward AM, Alonso-Coello P, et al. Self-monitoring and self-management of
oral anticoagulation. Cochrane Database Syst Rev. 2010;(4).
5. Quick AJ, Stanley-Brown M, Bancroft FW (1935). "A study of the coagulation defect in hemophilia and in jaundice". Am J Med Sci 190:501.
6. Owren PA, Aas K (1951). "The control of dicumarol therapy and the quantitative determination of prothrombin and proconvertin". Scand. J. Clin. Lab. Invest. 3 (3): 201–8.
7. Loeliger EA, Lewis SM. Progress in laboratory control of anticoagulants. Lancet ii:3 18-20. 8. World Health Organization. Expert Committee on Biological Standardisation. 33rd Report. WHO Technical Report Series.Geneva: WHO, 1983:1-105.
9. Ingram GI, Hills M. Reference method for the one-stage prothrombintime in human blood. International committee for standardization in hematology.Thromb Haemost 1976;36:237-238.
http://mutagens.co.in245 Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246 ISSN 2320-1355
10. Medicare expands coverage for home blood testing of prothrombin time international normalized
ratio". The Centers for Medicare and Medicaid Services. 19 March 2008.
11. Medicare expands coverage for home blood testing of prothrombin time international normalized
ratio". The Centers for Medicare and Medicaid Services. 19 March 2008.
12. Horsti J, Uppa H, Vilpo JA (March 2005). "Poor agreement among prothrombin time international normalized ratio methods: comparison of seven commercial reagents".Clin. Chem. 51 (3): 553–60.
13. Ansell J, Hirsh J, Poller L, Bussey H, Jacobson A, Hylek E. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:457S-482S.
14. Jackson S, Bereznicki L, Peterson G, et al. An update on INR monitoring. Aust Pharmacist.
15. World Health Organization Expert Committee on Biological Standardization.33rd report:Technical Report Series, no. 687. Geneva, Switzerland: World Health Organization, 1983.
16. World Health Organization Expert Committee on Biological Standardization. Guidelines for thromboplastins and plasma used to control anticoagulant therapy. WHO Technical Report Series 1999;889:64-93
17. Trotter JF, Brimhall B, Arjal R, Phillips C. Specific laboratory methodologies achieve higher model for endstage liver disease (MELD) scores for patients listed for liver transplantation. Liver Transpl 2004;10:995-1000.
18. Fritsma, George A. "Evaluation of Hemostasis." Hematology: Clinical Principles and Applications . Ed. Bernadette Rodak. W.B. Saunders Company: Philadelphia, 2002. 719-53.
19. Riley RS, Rowe D, & Fisher LM: Clinical utilization of the international normalized ratio (INR).
20. Haemostatis and Thrombosis Task Force of the British Society for Standards in Haematology:
Guidelines on oral anticoagulation: third edition. Br J Haematol 1998; 101(2):374-287.
21. Kucher N, Connolly S, Beckman JA, et al.International normalized ratio increase before warfarin-associated hemorrhage: brief and subtle. Arch Intern Med. 2004;164:2176–2179.
22. Zumberg M, Kitchens CS. Purpura and other hematovascular disorders. In: Kitchens CS, Alving
BM, Kessler CM, eds. Consultative Hemostasis and Thrombosis. 2nd ed. Philadelphia, Pa: Saunders; 2007: 159–182.
http://mutagens.co.in246
Andrea R. Castillo, Assistant Professor Curriculum Vitae Eastern Washington University 258 Science Building Cheney, WA 99004-2440 Phone: (509) 359-2866, Fax: (509) 359-6867, email: [email protected] Current Position: Assistant Professor of Biology, Eastern Washington UniversityPostdoctoral fellow with Dr. Karen Ottemann, University of California, Santa Cruz, CAPostdoctoral fellow with Dr
PRESCRIPTION DRUG RIDER This Prescription Drug Rider (“Rider”) is made a part of Coventry Health and Life Insurance Company’s Certificate of Coverage (“COC”). The benefits provided by this Rider become effective on the date Coverage under the COC is effective. PRESCRIPTION DRUG BENEFITS Subject to the terms, conditions and scope of coverage, including all Exclusions, Limitati



 Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246
Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246 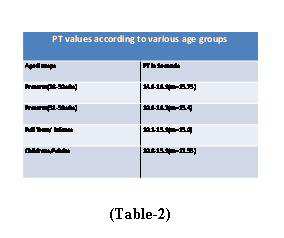

 Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246
Journal of Global Biosciences Vol. 2(6), 2013 pp. 241-246