The Journal of Clinical Endocrinology & Metabolism 92(4):1305–1310
Copyright 2007 by The Endocrine Society
The Peroxisome Proliferator-Activated Receptor-␥ Agonist Rosiglitazone Decreases Bone Formation and Bone Mineral Density in Healthy Postmenopausal Women: A Randomized, Controlled Trial
Andrew Grey, Mark Bolland, Greg Gamble, Diana Wattie, Anne Horne, James Davidson, and Ian R. Reid
Department of Medicine (A.G., M.B., G.G., D.W., A.H., I.R.R.), University of Auckland, and LabPlus (J.D.), Auckland CityHospital, 1020 Auckland, New ZealandContext: Thiazolidinediones, which are peroxisome proliferator-ac- Results: The osteoblast markers procollagen type I N-terminal
tivated receptor-␥ agonists, are widely prescribed to patients with
propeptide and osteocalcin declined by 13% (P Ͻ 0.005 vs. placebo)
disorders characterized by insulin resistance. Preclinical studies sug-
and 10% (P ϭ 0.04 vs. placebo), respectively, in the rosiglita-
gest that peroxisome proliferator-activated receptor-␥ signaling neg-
zone group. These changes were evident by 4 wk and persisted for
atively regulates bone formation and bone density. Human data on
the duration of the study. There was no change in the serum
the skeletal effects of thiazolidinediones are currently available only
-C-terminal telopeptide of type I collagen, a marker of bone re-
sorption (P ϭ 0.9 vs. placebo). Total hip bone density fell in therosiglitazone group (mean change from baseline rosiglitazone
Objective: The objective of the study was to determine whether
Ϫ1.9%, placebo Ϫ0.2%; between-group difference 1.7%, 95% con-
rosiglitazone, a thiazolidinedione, inhibits bone formation.
fidence interval 0.6 –2.7, P Ͻ 0.01); lumbar spine bone density fellsignificantly from baseline values in the rosiglitazone group (P ϭ
Design: The study was a 14-wk randomized, double-blind, placebo-
0.02 vs. baseline) but was not significantly different between
groups (mean change from baseline rosiglitazone Ϫ1.2%, placebo
Ϫ0.2%; between-group difference 1.0%, 95% confidence interval
Setting: The study was conducted in the general community. Patients: Fifty healthy, postmenopausal women participated in the study. Conclusions: Short-term therapy with rosiglitazone exerts detrimental skeletal effects by inhibiting bone formation. Skeletal Intervention: Intervention was rosiglitazone 8 mg/d.
end points should be included in future long-term studies of thia- zolidinedione use. (J Clin Endocrinol Metab 92: 1305–1310, Main Outcome Measures: The primary end point was biochemical
markers of bone formation, and secondary end points were a boneresorption marker and bone mineral density.
THIAZOLIDINEDIONESAREinsulin-sensitizingagents PPAR-␥isexpressedinanumberoftissues(1),raisingthe
that are widely prescribed in the management of a
possibility that drugs that interact with it may induce clinical
variety of clinical conditions characterized by insulin resis-
effects other than insulin sensitization. Prominent among the
tance (1, 2). They are agonists of the peroxisome proliferator-
tissues in which PPAR-␥ is expressed is bone. In skeletal
activated receptor (PPAR) family of nuclear transcription
tissue, PPAR-␥ acts as a molecular switch that regulates the
factors, in particular the PPAR-␥ isoform (1). In patients with
fate of pluripotent mesenchymal stem cells, which have the
type 2 diabetes mellitus, their use is associated with signif-
ability to differentiate into adipocytes or osteoblasts. In vitro,
icant improvements in glycemic control and serum lipopro-
PPAR-␥ agonists promote adipocyte differentiation in pref-
tein profile, although their ability to reduce the incidence of
erence to osteoblast differentiation (5– 8). There are conflict-
vascular events is uncertain (3). At present, thiazolidinedio-
ing reports of the effects of PPAR-␥ activation on osteoclas-
nes account for 21% of oral antihyperglycemic drugs used in
togenesis (9, 10). Haploinsufficiency of the PPAR-␥ gene in
the United States and 5% in Europe (4). It is estimated that
mice induces a high bone density phenotype characterized
2 million Americans were prescribed rosiglitazone last year
by increased rates of osteoblastic bone formation (11, 12),
(personal communication, Westun, C., GlaxoSmithKline,
whereas treatment of rodents with PPAR-␥ agonists induces
bone loss characterized by deficient osteoblast function (12–14). Data from human studies of the skeletal actions of thia-
First Published Online January 30, 2007
zolidinediones are currently available only from an obser-
Abbreviations: BMD, Bone mineral density; CTX, -C-terminal te-
vational study, which reported that female, but not male,
lopeptide of type I collagen; P1NP, procollagen type-I N-terminal
diabetic thiazolidinedione users experience accelerated bone
propeptide; PPAR, peroxisome proliferator-activated receptor.
loss, compared with nonthiazolidinedione users (15). JCEM is published monthly by The Endocrine Society (http://www.
Patients with type 2 diabetes may be at increased risk of
endo-society.org), the foremost professional society serving the en- docrine community.
fragility fractures (16 –22). Because PPAR-␥ agonists are in-
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
Grey et al. • Rosiglitazone and Bone Formation
creasingly frequently used to treat this disease, it is important
tablet was similar, but not identical with, the active tablet. Tablets were
to determine whether these drugs have adverse effects on the
dispensed into identical opaque containers by a staff member who was
human skeleton. We undertook a randomized, placebo-con-
not involved in giving study medication to participants. Each containerwas labeled with the subject’s study number and distributed to the
trolled trial to test the hypothesis that treatment with ros-
participant by another staff member. Subjects took one study tablet daily
iglitazone would cause adverse skeletal effects in healthy
for the first 2 wk and then two tablets daily for the remainder of the
postmenopausal women. The primary objective was to de-
study. Blood samples were collected fasting between 0800 and 1000 h at
termine the effect of rosiglitazone 8 mg daily on biochemical
baseline and 2, 4, 8, and 14 wk. Treatment allocations were randomizedby the study statistician, using a variable block size schedule, based on
markers of bone formation over a 14-wk period. Secondary
computer-generated random numbers. To ensure masking, only the
end points were change in markers of bone resorption and
statistician had access to treatment allocation. All the other study per-
sonnel and subjects were blinded to treatment allocation throughout. Only the study statistician saw unblinded data, but he had no contact
Subjects and Methods
with study participants. The study was approved by the AucklandEthics Committee, and written informed consent was provided by each
participant. The trial is registered at the Australian Clinical Trials Reg-ister (ACTRN 012605000218695; www.actr.org.au).
Participants were normal postmenopausal women who were more
than 5 yr postmenopausal and aged older than 55 yr. They were re-cruited between January and October 2005. Women with illnesses or
receiving therapies likely to affect bone were ineligible, as were thosewith osteoporosis [bone mineral density (BMD) T score at lumbar spine
Serum calcium, phosphate, albumin, and total alkaline phosphatase
or total hip Յ Ϫ2.5] and those with any other major systemic disease or
activity were measured on a modular autoanalyzer (Roche, Stockholm,
contraindications to the use of thiazolidinediones. Subjects were re-
Sweden). 25-Hydroxyvitamin D was measured using a chemilumines-
cruited by advertisements seeking healthy postmenopausal women to
cent assay (Nichols, San Juan Capistrano, CA). Intact PTH was measured
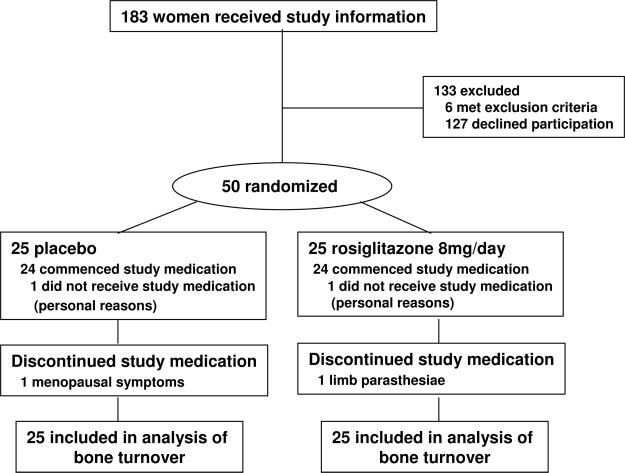
participate in clinical bone research. Of the 183 women who received
using an electrochemiluminescence immunoassay (E170; Roche). Serum
study information sheets, 75 attended a screening visit (Fig. 1). Six
osteocalcin, serum -C-terminal telopeptide of type I collagen (CTX)
women met exclusion criteria (one taking estrogen, one taking a bisphos-
and serum procollagen type-I N-terminal propeptide (P1NP) were mea-
phonate, one taking glucocorticoids, one taking an anticonvulsant, one
sured using commercially available kits, as previously described (23, 24).
with cancer, one with primary hyperparathyroidism), and 19 women
Coefficients of variation of these markers are as follows: osteocalcin,
elected for personal reasons (10 concerned about possible weight gain,
5.5%; CTX, 5.1%; PINP, 1.9%. Each turnover marker was assayed at the
two unwilling to undergo blood tests, four with nonexclusionary inter-
end of the study period in a single batch. Samples were stored at Ϫ70
current illnesses, three for unstated reasons) not to proceed to
Bone mineral density of the lumbar spine and proximal femur was
Among the 50 women randomized, four (two placebo, two rosigli-
measured by dual-energy x-ray absorptiometry using a Lunar Prodigy
tazone) withdrew during the study. One woman in each group never
instrument (GE-Lunar, Madison, WI; software version 7.51.008) at base-
started study medication (withdrew for personal reasons). One partic-
line and 14 wk. Bone density measurements were performed by two
ipant in the rosiglitazone group withdrew at 4 wk because of meno-
experienced technicians, both of whom are certified by Synarc, the
pausal symptoms, and one participant in the placebo group withdrew
international company that provides bone density oversight for most
after 16 d because of limb paresthesiae. Five women in the rosiglitazone
international osteoporosis drug registration trials. The coefficients of
group reported ankle swelling during the study, one of whom took 4 mg
variation for measurement of total hip and lumbar spine bone mineral
densities in our laboratory are 1.1 and 1.4%, respectively.
A randomized trial, comparing rosiglitazone 8 mg daily (2 ϫ 4 mg
The primary end points of the study were the two specific markers
tablets) with placebo over a period of 14 wk was performed. The placebo
of bone formation, osteocalcin and P1NP. The study was therefore de-
FIG. 1. Flow of subjects through the study.
Grey et al. • Rosiglitazone and Bone Formation
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
signed to detect a 1 sd difference between the treatment groups in thechange in either of these markers. Because recruitment made allowancefor dropouts, the number of completing subjects provides 80% power atthe 5% significance level to detect differences of at least 90% of 1 sdbetween the placebo and rosiglitazone arms. Sample-size calculationswere performed using PASS (NCSS and PASS number cruncher statis-tical systems, Kaysville, UT). Procedures of the statistical analysis systemSAS (version 9.2; SAS Institute Inc., Cary, NC) were used for all analyses. All statistical tests were two tailed, and a 5% significance level wasmaintained throughout. All treatment evaluations were performed onthe principle of intention to treat. A mixed-models approach to repeatedmeasures was used to examine the time course of response in treatmentand control arms at baseline and at 2, 4, 8 and 14 wk. The correctcovariance structure was determined by likelihood ratio test (i.e. thefirst-order autoregression matrix was compared against an unstructuredcovariance matrix). Maximum likelihood imputation was used to ensureall the randomized patients could be included in the model (25). Theassumptions of normality of the dependent variable and residuals weretested by inspection and goodness of fit assessed by maximizing theAkaike information criterion. P values for significant main and inter-action (treatment by time) effects were constructed using the method ofTukey.
The baseline characteristics of the study subjects are
shown in Table 1. At baseline, the only significant differencebetween the study groups was in serum osteocalcin, whichwas lower in the rosiglitazone group. Five of 25 subjects inthe placebo group and four of 25 subjects in the rosiglitazonegroup were taking calcium supplements at study inception;in each case the dose was unchanged during the study. Nosubjects took vitamin D supplements during the study. Com-pliance with study medication, as assessed by tablet counts,was 97% in the placebo group and 99% in the rosiglitazonegroup.
The effects of rosiglitazone on markers of bone turnover
are shown in Fig. 2. Figure 2, A and B, shows the osteoblast-specific markers P1NP and osteocalcin. Each of these mark-ers of bone formation was stable in the placebo group anddeclined significantly in the rosiglitazone group. Overall,P1NP declined by 13% in the rosiglitazone group by 4 wk,and this effect was maintained for the remainder of the study(P for time ϫ treatment interaction ϭ 0.004). Osteocalcin fellby 8% from baseline values in the rosiglitazone group, and
FIG. 2. The effects of rosiglitazone or placebo on markers of bone
the between-groups difference in this bone formation marker
turnover in normal postmenopausal women. A, Serum P1NP. B, Se-
was 10% at the study conclusion (P for time ϫ treatment
rum osteocalcin. C, CTX P (group ϫ time) is the P value for thetime-treatment interaction. Data are mean Ϯ SEM percent changefrom baseline. TABLE 1. Baseline characteristics of study subjects
interaction ϭ 0.04). Total serum alkaline phosphatase alsodeclined, by 17%, in the rosiglitazone group and remained
stable in the placebo group (mean change ϩ0.01%) (P for
time ϫ treatment interaction Ͻ 0.001). ␥-Glutamyl trans-
ferase did not change during the study (P for time ϫ treat-
In contrast to the bone formation markers, levels of serum
CTX, a marker of bone resorption, did not change in re-
sponse to rosiglitazone (P for time ϫ treatment interaction ϭ
There were no differences between the groups in the levels
of serum calcium, phosphate, and PTH (Table 2). Mean val-
Data are mean (SD) or number of subjects. Biochemical analytes are
ues of each of these variables were within the normal range
measured in serum. To convert 25-hydroxyvitamin D values to nano-moles per liter, multiply by 2.5. a P Ͻ 0.05 vs. placebo.
The changes in bone density are shown in Fig. 3. Total hip
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
Grey et al. • Rosiglitazone and Bone Formation
TABLE 2. Serum biochemistry in study subjects
Data are mean (SD). There were no differences between the groups in the change from baseline values in any of the variables shown. To convert
serum calcium to millimoles per liter, multiply by 0.25; to convert serum phosphate to millimoles per liter, multiply by 0.32; to convert PTHto picomoles per liter, multiply by 0.11.
the therapies commonly used to treat the disease may beincreasing that risk is a cause for concern. The increasing useof thiazolidinediones in other clinical conditions character-ized by insulin resistance (28, 29), including impaired glu-cose tolerance (30), is a further reason to fully characterizetheir long-term skeletal effects. We therefore suggest thatskeletal safety end points should be added to existing andplanned randomized trials of PPAR-␥ agonists so that theskeletal effects of thiazolidinediones can be studied over alonger period.
FIG. 3. The effect of rosiglitazone or placebo on BMD in normal post-
Although preclinical studies have consistently reported
menopausal women. P values refer to comparisons between groups in
that rosiglitazone impairs osteoblast function (13, 14, 31, 32),
the percent change from baseline at each indicated skeletal site. Data
conflicting in vitro data exist as to whether PPAR-␥ signaling
are mean Ϯ SEM percent change from baseline.
affects osteoclastogenesis (7, 9, 10). Our data suggest that
bone density declined by a greater amount in the rosiglita-
PPAR-␥ agonists do not influence bone resorption in vivo, a
zone group than the placebo group [mean (sd) change ros-
finding consistent with those of in vivo studies in rodents (11,
iglitazone Ϫ1.9 (2.0)%, placebo Ϫ0.2 (1.6)%, between-groups
13, 14). The limited preclinical data that are available on the
difference 1.7%, 95% confidence interval 0.6 –2.7, P ϭ 0.003].
skeletal effects of pioglitazone, the other commonly pre-
Lumbar spine bone density fell significantly from baseline
scribed thiazolidinedione, suggest that it has comparable
values in the rosiglitazone group (P ϭ 0.02 vs. baseline) and
actions with those of rosiglitazone (33, 34). Whether there is
remained stable in the placebo group (P ϭ 0.7 vs. baseline)
a class effect of thiazolidinediones on skeletal homeostasis is
but was not different between groups [mean (sd) change
uncertain, with recent preclinical studies of new compounds
rosiglitazone Ϫ1.2 (2.1)%, placebo Ϫ0.2 (2.1)%, between-
reporting both adverse (35) and neutral (36) effects in rodent
groups difference 1.0%, 95% confidence interval Ϫ0.2–2.3,
P ϭ 0.13]. As expected, body weight tended to increase in the
Currently there are few data available on the skeletal ac-
rosiglitazone group (mean change rosiglitazone ϩ0.7 kg; pla-
tions of thiazolidinediones in humans. Uncontrolled studies
cebo Ϫ0.8 kg, P for between-groups comparison in change
of Japanese subjects with type 2 diabetes treated with tro-
from baseline ϭ 0.07). Adjusting the bone density data for
glitazone, a PPAR-␥ agonist no longer in clinical use, re-
change in body weight, the baseline osteocalcin level, or both
ported significant reductions in markers of both bone for-
variables did not change the results.
mation and resorption after 1 month, but values returned tobaseline by 1 yr (37, 38). More recently an analysis of the
Discussion
small number (n ϭ 69) of diabetic subjects taking thiazo-
This study demonstrates that short-term therapy with ros-
lidinediones (pioglitazone, troglitazone, and rosiglitazone)
iglitazone, a commonly prescribed PPAR-␥ agonist, inhibits
in the Health, Aging, and Body Composition observational
bone formation and accelerates bone loss in healthy post-
study reported accelerated bone loss in over 4 yr in women
menopausal women. These data are consistent with those
but not men (15). After our manuscript was submitted, Kahn
from in vitro and animal studies demonstrating that PPAR-␥
et al. (39) reported a higher incidence of fractures, detected
signaling negatively regulates osteoblast function (bone for-
as adverse events, in female diabetic subjects randomized to
mation) and bone mass (7, 8, 11, 13, 14). The pattern of
receive rosiglitazone, compared with those randomized to
alteration of bone remodeling that we observed in response
receive either metformin or glyburide, during a 4 yr study of
to rosiglitazone is similar to that seen after the initiation of
glycemic durability of oral monotherapies. Our findings pro-
glucocorticoid therapy (26). The uncoupling of bone forma-
vide rigorous evidence for a detrimental effect of PPAR-␥
tion from resorption by glucocorticoids is accompanied by
agonists on the postmenopausal female skeleton. Whether
early and rapid bone loss and an increased risk of fragility
there is a gender difference in the skeletal response to thia-
fractures (27). Our data suggest that rosiglitazone may also
zolidinediones can be determined only by a randomized,
promote rapid bone loss; longer-term studies are needed to
determine whether the rate of loss we observed is sustained.
The mechanism(s) by which rosiglitazone alters bone re-
Because patients with type 2 diabetes may have an increased
modeling likely involves direct effects on osteoblast devel-
risk of fragility fractures (16 –20), the possibility that one of
opment and function, but the possibility of indirect skeletal
Grey et al. • Rosiglitazone and Bone Formation
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
actions also exists. Adipose tissue is a target for PPAR-␥
PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular
agonists, and some adipokines influence bone cell function.
Events): a randomised controlled trial. Lancet 366:1279 –1289
4. Yki-Jarvinen H 2005 The PROactive study: some answers, many questions.
Thiazolidinediones may decrease circulating levels of leptin
(38), the peripheral actions of which include osteoblast anab-
5. Gimble JM, Robinson CE, Wu X, Kelly KA, Rodriguez BR, Kliewer SA,
olism (40). The insulin-sensitizing actions of PPAR-␥ agonists
Lehmann JM, Morris DC 1996 Peroxisome proliferator-activated receptor-␥ activation by thiazolidinediones induces adipogenesis in bone marrow stromal
lower circulating levels of insulin (1) and therefore are likely
to reduce levels of the cosecreted pancreatic -cell peptide
6. Lecka-Czernik B, Gubrij I, Moerman EJ, Kajkenova O, Lipschitz DA, Mano- lagas SC, Jilka RL 1999 Inhibition of Osf2/Cbfa1 expression and terminal
amylin, each of which is anabolic to osteoblasts (41, 42).
osteoblast differentiation by PPAR␥2. J Cell Biochem 74:357–371
A theoretical limitation of our study is the possibility that
7. Kawaguchi H, Akune T, Yamaguchi M, Ohba S, Ogata N, Chung U-i, Kubota
dual-energy x-ray absorptiometry may underestimate bone
N, Terauchi Y, Kadowaki T, Nakamura K 2005 Distinct effects of PPAR␥ insufficiency on bone marrow cells, osteoblasts, and osteoclastic cells. J Bone
density in rosiglitazone-treated subjects because of changes
in bone marrow adiposity. We think this unlikely because,
8. Khan E, Abu-Amer Y 2003 Activation of peroxisome proliferator-activated
although it is not known whether rosiglitazone increases
receptor-␥ inhibits differentiation of preosteoblasts. J Lab Clin Med 142:29 –34
9. Okazaki R, Toriumi M, Fukumoto S, Miyamoto M, Fujita T, Tanaka K,
marrow fat in humans, 30-fold higher doses (by body weight)
Takeuchi Y 1999 Thiazolidinediones inhibit osteoclast-like cell formation and
of drug than those used in our study do not increase marrow
bone resorption in vitro. Endocrinology 140:5060 –5065
10. Mbalaviele G, Abu-Amer Y, Meng A, Jaiswal R, Beck S, Pittenger MF,
fat in rodents (13), and dual-energy x-ray absorptiometry
Thiede MA, Marshak DR 2000 Activation of peroxisome proliferator-acti-
accurately measures bone density in vivo, as corroborated by
vated receptor-␥ pathway inhibits osteoclast differentiation. J Biol Chem 275:
histomorphometry and/or microcomputed tomography,
11. Akune T, Ohba S, Kamekura S, Yamaguchi M, Chung U-i, Kubota N, Ter-
when marrow adiposity is known to be either increased (31,
auchi Y, Harada Y, Azuma Y, Nakamura K, Kadowaki T, Kawaguchi H 2004
PPAR-␥ insufficiency enhances osteogenesis through osteoblast formation
Limitations of the present study are its short duration and
from bone marrow progenitors. J Clin Invest 113:846 – 855
12. Pei L, Tontonoz P 2004 Fat’s loss is bone’s gain. J Clin Invest 113:805– 806
the healthy volunteer study population. An advantage of
13. Soroceanu MA, Miao D, Bai X-Y, Su H, Goltzman D, Karaplis AC 2004
studying healthy subjects is that it allows an assessment of
Rosiglitazone impacts negatively on bone by promoting osteoblast/osteocyte
the effects of rosiglitazone on bone metabolism, independent
14. Ali AA, Weinstein RS, Stewart SA, Parfitt AM, Manolagas SC, Jilka RL 2005
of any confounding introduced by improvements in the met-
Rosiglitazone causes bone loss in mice by suppressing osteoblast differenti-
abolic control of diabetes mellitus (44). Furthermore, because
ation and bone formation. Endocrinology 146:1226 –1235
15. Schwartz AV, Sellmeyer DE, Vittinghoff E, Palermo L, Lecka-Czernik B,
the indications for use of thiazolidinediones are expanding
Feingold KR, Strotmeyer ES, Resnick HE, Carbone L, Beamer BA, Park SW,
to include individuals with insulin resistance (30), assess-
Lane NE, Harris TB, Cummings SR 2006 Thiazolidinedione use and bone loss
ment of their bone effects outside the context of a specific
in older diabetic adults. J Clin Endocrinol Metab 91:3349 –3354
16. Strotmeyer ES, Cauley JA, Schwartz AV, Nevitt MC, Resnick HE, Bauer DC,
pathological state is appropriate. The short duration of the
Tylavsky FA, de Rekeneire N, Harris TB, Newman AB 2005 Nontraumatic
study was necessary because the hypothesis was one of
fracture risk with diabetes mellitus and impaired fasting glucose in older white
harm, and the study participants were normal volunteers
and black adults: the health, aging, and body composition study. Arch InternMed 165:1612–1617
who would not be expected to benefit from the intervention.
17. de Liefde II, van der Klift M, de Laet CEDH, van Daele PLA, Hofman A, Pols
We believe that the 14-wk study duration was adequate to
HAP 2005 Bone mineral density and fracture risk in type-2 diabetes mellitus: the Rotterdam Study. Osteoporos Int 16:1713–1720
provide proof of principle that thiazolidinediones impact
18. Nicodemus KK, Folsom AR 2001 Type 1 and type 2 diabetes and incident hip
adversely on the human skeleton, without exposing the sub-
fractures in postmenopausal women. Diabetes Care 24:1192–1197
jects to a significant risk of long-term skeletal harm. Longer-
19. Vestergaard P, Rejnmark L, Mosekilde L 2005 Relative fracture risk in patients
with diabetes mellitus, and the impact of insulin and oral antidiabetic med-
term studies are clearly necessary, but these would best be
ication on relative fracture risk. Diabetologia 48:1292–1299
undertaken in study populations that might reasonably be
20. Taylor BC, Schreiner PJ, Stone KL, Fink HA, Cummings SR, Nevitt MC,
expected to derive some benefit from thiazolidinedione use,
Bowman PJ, Ensrud KE 2004 Long-term prediction of incident hip fracture risk in elderly white women: study of osteoporotic fractures. J Am Geriatr Soc
such as people with type 2 diabetes and/or impaired glucose
21. Strotmeyer ES, Cauley JA, Schwartz AV, Nevitt MC, Resnick HE, Zmuda JM, Bauer DC, Tylavsky FA, de Rekeneire N, Harris TB, Newman AB, Health ABCS 2004 Diabetes is associated independently of body composition with Acknowledgments
BMD and bone volume in older white and black men and women: the Health,Aging, and Body Composition Study. J Bone Miner Res 19:1084 –1091
22. Bonds DE, Larson JC, Schwartz AV, Strotmeyer ES, Robbins J, Rodriguez
Received November 30, 2006. Accepted January 22, 2007. BL, Johnson KC, Margolis KL 2006 Risk of fracture in women with type 2
Address all correspondence and requests for reprints to: Dr. Andrew
diabetes: the Women’s Health Initiative Observational Study. J Clin Endocrinol
Grey, Department of Medicine, University of Auckland, Private Bag
23. Reid IR, Davidson JS, Wattie D, Wu F, Lucas J, Gamble GD, Rutland MD,
92019, 1020 Auckland, New Zealand. E-mail: [email protected]. Cundy T 2004 Comparative responses of bone turnover markers to bisphos-
This work was supported by the Health Research Council of New
phonate therapy in Paget’s disease of bone. Bone 35:224 –230
Zealand. M.B. is the recipient of a Fellowship from the Australia and
24. Reid IR, Lucas J, Wattie D, Horne A, Bolland M, Gamble GD, Davidson JS,
New Zealand Bone and Mineral Society. Grey AB 2005 Effects of a -blocker on bone turnover in normal postmeno-
Author Disclosure Summary: None of the authors have anything to
pausal women: a randomized controlled trial. J Clin Endocrinol Metab 90:
25. Truxillo C, Maximum likelihood parameter estimation with incomplete data.
SAS Users Group International Conference, Philadelphia, PA, 2005 (http://
References
www2.sas.com/proceedings/sugi30/111-30.pdf)
26. Ton FN, Gunawardene SC, Lee H, Neer RM 2005 Effects of low-dose pred-
1. Yki-Jarvinen H 2004 Thiazolidinediones. N Engl J Med 351:1106 –1118
nisone on bone metabolism. J Bone Miner Res 20:464 – 470
2. Kendall DM 2006 Thiazolidinediones: the case for early use. Diabetes Care
27. Reid IR 1997 Glucocorticoid osteoporosis—mechanisms and management.
3. Dormandy JA, Charbonnel B, Eckland DJA, Erdmann E, Massi-Benedetti M,
28. Staels B, Fruchart J-C 2005 Therapeutic roles of peroxisome proliferator- Moules IK, Skene AM, Tan MH, Lefebvre PJ, Murray GD 2005 Secondary
activated receptor agonists. Diabetes 54:2460 –2470
prevention of macrovascular events in patients with type 2 diabetes in the
29. Ehrmann DA 2005 Polycystic ovary syndrome. N Engl J Med 352:1223–1236
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
Grey et al. • Rosiglitazone and Bone Formation
30. The Dream Trial Investigators 2006 Effect of rosiglitazone on the frequency
38. Watanabe S, Takeuchi Y, Fukumoto S, Fujita H, Nakano T, Fujita T 2003
of diabetes in patients with impaired glucose tolerance or impaired fasting
Decrease in serum leptin by troglitazone is associated with preventing bone
glucose: a randomised controlled trial. Lancet 368:1096 –1105
loss in type 2 diabetic patients. J Bone Miner Metab 21:166 –171
31. Rzonca SO, Suva LJ, Gaddy D, Montague DC, Lecka-Czernik B 2004 Bone
39. Kahn SE, Haffner SM, Heise MA, Herman WH, Holman RR, Jones NP,
is a target for the antidiabetic compound rosiglitazone. Endocrinology 145:
Kravitz BG, Lachin JM, O’Neill MC, Zinman B, Viberti G, for the ADOPT Study Group 2006 Glycemic durability of rosiglitazone, metformin, or gly-
32. Lecka-Czernik B, Moerman EJ, Grant DF, Lehmann JM, Manolagas SC, Jilka
buride monotherapy. N Engl J Med 355:2427–2443
RL 2002 Divergent effects of selective peroxisome proliferator-activated re-
40. Cornish J, Callon KE, Bava U, Lin C, Naot D, Hill BL, Grey AB, Broom N,
ceptor-␥2 ligands on adipocyte versus osteoblast differentiation. Endocrinol-
Myers DE, Nicholson GC, Reid IR 2002 Leptin directly regulates bone cell
function in vitro and reduces bone fragility in vivo. J Endocrinol 175:405– 415
33. Jennermann C, Triantafillou J, Cowan D, Pennink BGA, Connolly KM,
41. Cornish J, Callon KE, King AR, Cooper GJS, Reid IR 1998 Systemic admin- Morris DC 1995 Effects of thiazolidinediones on bone turnover in the rat.
istration of amylin increases bone mass, linear growth, and adiposity in adult
34. Syversen U, Bakke I, Aune G, Thommesen L 2003 PPAR-␣ agonists increase
bone mineral density in female rats. J Bone Miner Res 18(Suppl 2):S42
42. Cornish J, Callon KE, Reid IR 1996 Insulin increases histomorphometric
35. Li M, Pan LC, Simmons HA, Li Y, Healy DR, Robinson BS, Ke HZ, Brown
indices of bone formation in vivo. Calcif Tissue Int 59:492– 495
TA 2006 Surface-specific effects of a PPAR-␥ agonist, darglitazone, on bone in
43. Justesen J, Mosekilde L, Holmes M, Stenderup K, Gasser J, Mullins JJ, Seckl JR, Kassem M 2004 Mice deficient in 11-hydroxysteroid dehydrogenase type
36. Lazarenko OP, Rzonca SO, Suva LJ, Lecka-Czernik B 2006 Netoglitazone is
1 lack bone marrow adipocytes, but maintain normal bone formation. Endo-
a PPAR-␥ ligand with selective effects on bone and fat. Bone 38:74 – 84
37. Okazaki R, Miura M, Toriumi M, Taguchi M, Hirota Y, Fukumoto S, Fujita
44. Okazaki R, Totsuka Y, Hamano K, Ajima M, Miura M, Hirota Y, Hata K, T, Tanaka K, Takeuchi A 1999 Short-term treatment with troglitazone de- Fukumoto S, Matsumoto T 1997 Metabolic improvement of poorly controlled
creases bone turnover in patients with type 2 diabetes mellitus. Endocr J
noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin En-
JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.
V O L U M E V I S S U E I I D B S A S o u t h e r n N e v a d a S P R I N G E D I T I O N WH W A H T A T C A C N A N D B D S B A S A S O S U O T U H T E H RN R N N E N V E A V D A A D A SU S P U P P O P R O T R
Michael G. Crookston, DDS • Nathan D. Call, DDS 1 Please Read , and Answer the Fol owing Questions, Medical History Form Are you having pain or discomfort at this time? 2. Do you have or have you ever had bleeding or sensitive gums? 3. Do you feel nervous about having dental treatment? 4. Have you been hospitalized during the past two years? 5. Have you been under the care of a medical d
 J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
Grey et al. • Rosiglitazone and Bone Formation
creasingly frequently used to treat this disease, it is important
tablet was similar, but not identical with, the active tablet. Tablets were
to determine whether these drugs have adverse effects on the
dispensed into identical opaque containers by a staff member who was
human skeleton. We undertook a randomized, placebo-con-
not involved in giving study medication to participants. Each containerwas labeled with the subject’s study number and distributed to the
trolled trial to test the hypothesis that treatment with ros-
participant by another staff member. Subjects took one study tablet daily
iglitazone would cause adverse skeletal effects in healthy
for the first 2 wk and then two tablets daily for the remainder of the
postmenopausal women. The primary objective was to de-
study. Blood samples were collected fasting between 0800 and 1000 h at
termine the effect of rosiglitazone 8 mg daily on biochemical
baseline and 2, 4, 8, and 14 wk. Treatment allocations were randomizedby the study statistician, using a variable block size schedule, based on
markers of bone formation over a 14-wk period. Secondary
computer-generated random numbers. To ensure masking, only the
end points were change in markers of bone resorption and
statistician had access to treatment allocation. All the other study per-
sonnel and subjects were blinded to treatment allocation throughout.
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
Grey et al. • Rosiglitazone and Bone Formation
creasingly frequently used to treat this disease, it is important
tablet was similar, but not identical with, the active tablet. Tablets were
to determine whether these drugs have adverse effects on the
dispensed into identical opaque containers by a staff member who was
human skeleton. We undertook a randomized, placebo-con-
not involved in giving study medication to participants. Each containerwas labeled with the subject’s study number and distributed to the
trolled trial to test the hypothesis that treatment with ros-
participant by another staff member. Subjects took one study tablet daily
iglitazone would cause adverse skeletal effects in healthy
for the first 2 wk and then two tablets daily for the remainder of the
postmenopausal women. The primary objective was to de-
study. Blood samples were collected fasting between 0800 and 1000 h at
termine the effect of rosiglitazone 8 mg daily on biochemical
baseline and 2, 4, 8, and 14 wk. Treatment allocations were randomizedby the study statistician, using a variable block size schedule, based on
markers of bone formation over a 14-wk period. Secondary
computer-generated random numbers. To ensure masking, only the
end points were change in markers of bone resorption and
statistician had access to treatment allocation. All the other study per-
sonnel and subjects were blinded to treatment allocation throughout.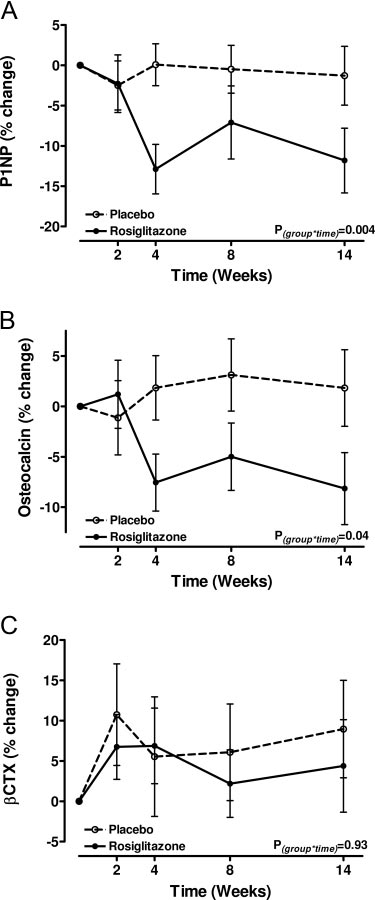 Grey et al. • Rosiglitazone and Bone Formation
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
signed to detect a 1 sd difference between the treatment groups in thechange in either of these markers. Because recruitment made allowancefor dropouts, the number of completing subjects provides 80% power atthe 5% significance level to detect differences of at least 90% of 1 sdbetween the placebo and rosiglitazone arms. Sample-size calculationswere performed using PASS (NCSS and PASS number cruncher statis-tical systems, Kaysville, UT). Procedures of the statistical analysis systemSAS (version 9.2; SAS Institute Inc., Cary, NC) were used for all analyses.
Grey et al. • Rosiglitazone and Bone Formation
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
signed to detect a 1 sd difference between the treatment groups in thechange in either of these markers. Because recruitment made allowancefor dropouts, the number of completing subjects provides 80% power atthe 5% significance level to detect differences of at least 90% of 1 sdbetween the placebo and rosiglitazone arms. Sample-size calculationswere performed using PASS (NCSS and PASS number cruncher statis-tical systems, Kaysville, UT). Procedures of the statistical analysis systemSAS (version 9.2; SAS Institute Inc., Cary, NC) were used for all analyses.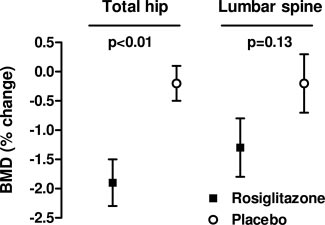 J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
Grey et al. • Rosiglitazone and Bone Formation
TABLE 2. Serum biochemistry in study subjects
J Clin Endocrinol Metab, April 2007, 92(4):1305–1310
Grey et al. • Rosiglitazone and Bone Formation
TABLE 2. Serum biochemistry in study subjects