WORKING AT HIGH ALTITUDE: MEDICAL PROBLEMS, MISCONCEPTIONS, AND SOLUTIONS Department of Medicine, University of California San Diego Owens Valley Radio Observatory, California Institute of Technology
(Accepted for publication by The Observatory.)
Telescopes are being placed at increasingly high altitudes. The summit of Mauna Kea,
Hawaii (altitude 4200 m) has been a popular site for some time, but more recently telescopes
have been located on the Chajnantor plateau in north Chile at an altitude of 5050 m. This will
also be the site of the multinational Atacama Large Millimeter Array. Other nearby sites up to
5800 m have been used for various instruments. Although remote observing is increasingly
employed this is not always possible, and it will always be necessary to have some human beings
at the sites. These altitudes can have serious effects on mental and physical performance and
quality of sleep. The deleterious effects are reduced by the process of acclimatization but it is a
misconception to argue that this returns mental and physical performance to normal. In fact fully
acclimatized astronomers on the summit of Mauna Kea are so oxygen-deprived that if this was
caused by lung disease at sea level they would be entitled to treatment by continuous oxygen
therapy. All the medical effects of high altitude are caused by the low partial pressure of oxygen
in the inspired air, and so the most effective way of improving human performance is to add
supplementary oxygen. Recent technical advances allow this to be done very efficiently by
oxygen enrichment of room air. The occupants of the room are generally unaware of the added
oxygen but their mental and physical performance is significantly enhanced. Oxygen enrichment
for altitudes of 5000 m and above should be mandatory and would also be helpful at more
Increasingly, astronomers are setting up instruments and working at high altitudes. The
low scale-height of water in the atmosphere, and the dramatically reduced precipitable water
burden at high altitudes improves atmospheric transmission dramatically in critical wavelength
bands. One of the best known sites is Mauna Kea, Hawaii where the altitude of the summit is
4200 m and there are a number of telescopes on or near the summit. Recently there has been
much activity in north Chile in the Chajnantor region east of San Pedro de Atacama. Here there
is an extensive plateau at an altitude of about 5050 m and this can be accessed most days of the
year by a road from San Pedro de Atacama (altitude 2440 m). A group from the California
Institute of Technology has been operating the Cosmic Background Imager (CBI) there since
August 1999. The site will also be used by the multinational Atacama Large Millimeter Array
(ALMA). Nearby a German group has installed a telescope near the CBI at an altitude of 5050 m
and there is a Japanese telescope at the slightly lower altitude of 4800 m. Even higher sites on
nearby extinct volcanoes have been investigated, and altitudes up to 5800 m have been used
occasionally. Groups from Princeton and the University of Pennsylvania have operated the
Mobile Anisotropy Telescope (MAT) near this altitude successfully on three occasions for
These altitudes have many important effects on the human body and there is a large
literature on the subject1,2. Several articles have been written specifically for astronomers3-7.
However there have been a number of important advances in the last five years. In addition some
misconceptions about the medical effects of high altitude have developed in some members of
the astronomy community. One of these is that acclimatization to high altitude fully protects the
individual from the deleterious effects of the low oxygen. This is a serious fallacy and is
discussed in more detail below. A major recent advance is improvements in technolo gy that
allow economical oxygen enrichment of the working spaces for astronomers at high altitude.
Although there is a curious prejudice against this innovation in some quarters, all the evidence
suggests that it is an important advance for people who have to work at high altitude, leading to
substantial improvement in personnel safety, and more cost-effective operations.
Of course the fact that telescopes are sited at high altitude does not necessarily mean that
the observers are there. In fact the technology of remote observing is now very sophisticated.
Nevertheless it is certainly necessary to have humans at the observatory site while the telescope
is being built and tested, and in most instances some staff will be required at the site. Therefore
human factors at high altitude will always be important.
This brief review will first summarize how the oxygen deprivation at high altitude affects
the human body. Then the important topics of acclimatization to high altitude, and the common
high-altitude diseases will be briefly covered. Finally methods of combatting the oxygen
deprivation of high altitude will be considered.
2. Why High Altitude Affects the Human Body
High altitude impairs human function because of the oxygen deprivation. Of course other
factors such as cold and high winds may be present but these can be negated by appropriate
protection. The reduction in oxygen is best described by the fall in inspired partial pressure of
oxygen (PO2). As altitude increases, barometric pressure falls though here it is worth mentioning
that for most locations of interest to astronomers (for example, Mauna Kea and north Chile) the
Standard Atmosphere8 is not applicable. The reason is that these locations are at low latitudes
where the barometric pressure for a given altitude is higher than predicted from the Standard
Atmosphere. As an example, at an altitude of 5800 m near Chajnantor the Standard Atmosphere
predicts a barometric pressure of 363.5 torr (485 mb) whereas the actual pressure is close to
379.0 torr (505 mb). This difference is significant from a physiological point of view and, for
example, represents a change of altitude of over 300 m.
Physiologists always calculate the inspired PO2 because that is the partial pressure of
oxygen actually available to the body. When air is inspired it is warmed and saturated with water
vapor at the body temperature of 37°C and therefore the water vapor pressure is 47 torr. This is
irrespective of altitude. Therefore the inspired PO2 is given by PIO2 = 0.2093 (PB - 47) where PB
is the barometric pressure. The inspired PO2 at sea level, the University of California White
Mountain Research Station (altitude 3800 m), Mauna Kea (altitude 4200 m), Chajnantor (altitude
5050 m) and a nearby peak (altitude 5800 m) are shown in Table I.
It can be seen that at Chajnantor the inspired PO2 is only about 52% of the sea level value.
The table is perhaps misleading in that it shows that the difference of PO2 between Mauna Kea
and Chajnantor is only 7% of the sea level value, and that between Chajnantor and the nearby
peak at 5800 m is only about 5% of the sea level value. However the physiological effects of this
oxygen reduction are very nonlinear. There is a world of difference between the physiological
effects of hypoxia at Chajnantor and Mauna Kea, and again a very large difference between 5800
3. Effects of High Altitude on Human Performance
The medical effects of high altitude are legion. However in the present context they are
3.1. Mental Performance
Most people who have worked at altitudes over 4000 m state that mental ability is
impaired. They recognize an increased number of arithmetical errors, reduced attention span,
increased fatigue, impaired short-term memory, and increased difficulty in making decisions.
However it has proved to be very difficult to quantitate impairment of mental function. This was
recognized eighty years ago by the British physiologist Joseph Barcroft when he was reporting
on his experiences at Cerro de Pasco, Peru (altitude 4330 m) and wrote:
.judged by the ordinary standards of efficiency in laboratory work, we were in an
obviously lower category at Cerro that at the sea level. By a curious paradox this
was most apparent when it was being least tested, for perhaps what we suffered
from chiefly was the difficulty of maintaining concentration. When we knew we
were undergoing a test, our concentration could by an effort be maintained over
the length of time taken for the test, but under ordinary circumstances it would
lapse. It is, perhaps, characteristic that, whilst each ind ividual mental test was
done as rapidly at Cerro as at the sea level, the performance of the series took
nearly twice as long for its accomplishment. Time was wasted there in trivialities
and ‘bungling’, which would not take place at sea level9.
In other words, most intelligent competitive people when faced with a test of mental function are
determined to do the best they can, and perform very well in the short term. However this
performance is not typical of that during the full working day.
Nevertheless McFarland has reported data on mental performance of unacclimatized
individuals at altitudes from 2500 to 5000 m and these are shown in Table II. The difficulties of
making these measurements are so great that the emphasis should be on the pattern of changes
rather than the individual numbers. Other investigators, for example Sharma and colleagues 10
have shown impairment of hand-eye coordination in acclimatized subjects at an altitude of 4000
m where their performance was only 63% of sea level after one month and this improved to 83%
after several months. In all these tests the “learning effect,” that is the ability to perform better
when the test is repeated on a number of occasions, can be important and is difficult to take into
account. Not all investigators have reported impairment of mental ability at altitudes of 4000 m.
For example, Forster4 measured numeric memory in shift workers in the U.K. Infrared Telescope
(UKIRT) at Mauna Kea and found that this was reduced to 88% of its sea level value on the first
day of work at 4200 m, but improved over the next few days so that by the fifth day there was no
significant difference between altitude and sea level. Here the effects of acclimatization are
important (see below) but again it is difficult to rule out the learning effect.
3.2. Physical Performance
The rate at which humans can perform physical work (power output) depends on the
amount of oxygen available to the body, so it is not surprising that as the altitude increases,
maximal oxygen uptake falls. There is a large literature on this topic and at the altitude of Mauna
Kea (4200 m) the power output of the body is reduced to about 70% of its sea level value. At the
altitude of Chajnantor (5050 m) power output drops to about 60% of the sea level value, and
there is a further fall to about 50% at an altitude of 5800 m. Although astronomers working at a
high altitude site will not often be called upon to exert maximum effort, the limitations in the
amount of physical work that can be done will be obvious.
Muscular exertion at high altitude is accompanied by very high levels of ventilation, that
is the product of rate and depth of breathing. As a result, people working at high altitude pant and
the resulting shortness of breath is often unpleasant. This panting will often continue for several
minutes after performing a heavy task. In fact even a small increase in activity, for example
sitting up in bed, at an altitude of 5800 m may cause panting for two or three minutes.
Just as important as the limited power output at high altitude is the great increase in
fatigue that follows several hours’ work. This is difficult to quantitate but people working at
altitudes of 5050 or particularly at 5800 m will generally find it impossible to do a full day’s
3.3. Sleep
One of the most unpleasant features of going to high altitude is difficulties with sleeping.
Indeed many people notice this at very modest altitudes such as 2500 to 3000 m at ski resorts.
Typically people complain that they wake frequently, have unpleasant dreams, and do not feel
refreshed in the morning. An important causative factor is “periodic breathing” during which the
breathing waxes and wanes with typical cycles of ten to fifteen seconds. Periods of no breathing
at all (apnea) lasting up to five or ten seconds may occur, and it is believed that the low oxygen
levels in the blood following apneic periods may account for some of the arousals. Many
measurements have been made during sleep at high altitude and these show large fluctuations in
the concentration of oxygen in the arterial blood caused by the waxing and waning of breathing.
Electroencephalographic studies confirm that the quality of sleep is impaired at high altitude.
Mountain climbers often adopt the policy of climbing high and sleeping low in order to reduce
Fortunately the human body has the ability to adapt to the oxygen deprivation of high
altitude to some extent, a process known as acclimatization (or acclimation). In fact physiologists
often use high-altitude acclimatiza tion as one of the best examples of the body’s response to a
The two most obvious features of high-altitude acclimatization are the increase in
breathing (hyperventilation) and the increase in concentration of red blood cells (polyc ythemia).
There are other less obvious features including an increased concentration of capillaries in some
body tissues, and changes of oxidative enzymes in the cells that enhance the ability of the tissues
to operate in an oxygen-deprived environment.
By far the most important feature of acclimatization is hyperventilation which is brought
about by an increase in both the rate and depth of breathing. As examples, an acclimatized
person at an altitude of 4200 m will have his or her ventilation increased by 15% while an
acclimatized subject at an altitude of 5800 m will have an increase of over 70%. It is this large
increase in ventilation that is responsible for the panting and sensation of shortness of breath on
The increase in ventilation is brought about by stimulation of sensors (chemoreceptors)
that respond to the low partial pressure of oxygen in the arterial blood. The advantage of
hyperventilation is that it raises the PO2 in the air in the depths of the lung (alveolar gas) and thus
counters the oxygen deprivation of the environment to some extent. The degree to which this is
effective is discussed below. When an individual goes to high altitude, the hyperventilation
gradually increases over the course of several days and this important feature of the
acclimatization process is essentially complete in ten days.
The other well-known feature of acclimatization is an increase in the concentration of red
cells in the blood (polycythemia). However the value of this process is very limited. First it takes
several weeks to develop and probably two or three months to reach its maximum value. It is true
that newcomers to high altitude often show an increase in red blood cell concentration within a
day or so but this is solely caused by dehydration and therefore concentration of the blood which
is very common at high altitude. All the evidence suggests that in the context of astronomers
working at high altitude, the increase in red cell concentration is a very minor advantage at high
altitude. Interestingly some people who spend many months at very high altitudes, for example
5800 m, develop such high levels of red cell concentration that these are thought to be
disadvantageous because the great cellularity of the blood affects its flow in peripheral
capillaries and consequently interferes with oxygen unloading 2. Polycythemia also increases the
4.1. Effectiveness of Acclimatization
As indicated above, the most important feature of acclimatization is the hyperventilation
which increases the PO2 and reduces the PCO2 of the alveolar gas. The efficacy of acclimatization
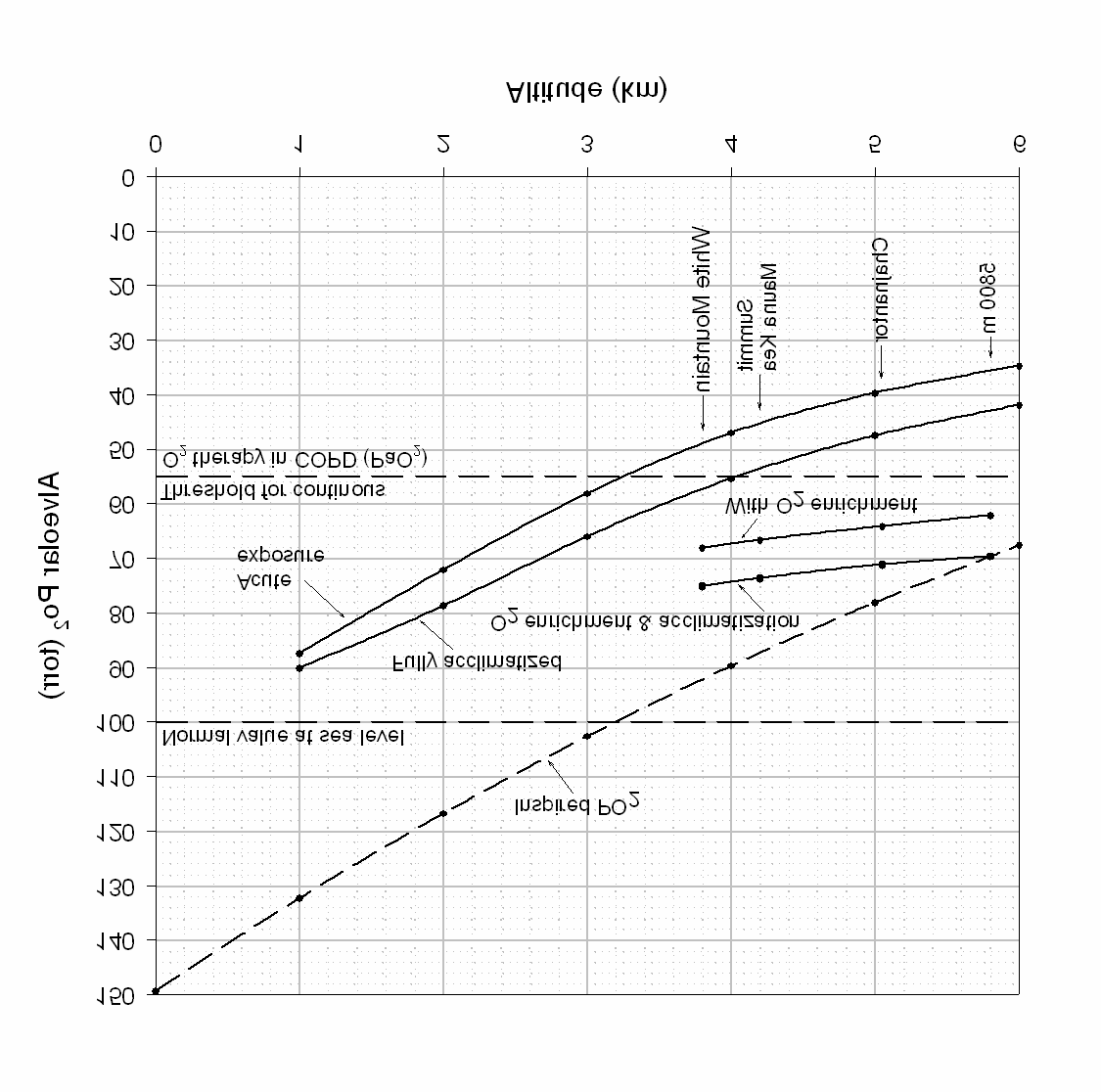
at various altitudes is shown in Figure 1. The horizontal broken line at a PO2 of 100 torr shows
the alveolar PO2 at sea level. The data for the lines indicating the alveolar PO2 for acute exposure
to high altitude (that is, with no acclimatization) and for full acclimatization come from Rahn
and Otis11. It can be seen that useful gains in the alveolar PO2 of between 5 and 10 torr occur at
all the altitudes of interest. However both the alveolar PO2 for acute exposure and full
acclimatization fall rapidly as altitude increases. Of course the reason for this is the fall in
inspired PO2 which is also shown in the figure. Note that at the summit of Mauna Kea the
alveolar PO2 for acute exposure is about 45 torr but this increases to about 53 torr if the subject is
fully acclimatized. For Chajnantor (altitude 5050 m) the numbers are about 39 and 47 torr,
respectively, and for the highest peak at altitude 5800 m, the values are about 35 and 43 torr,
respectively. It should be remembered that full acclimatization requires continuous residence at
4.2. Misconceptions about the Value of Acclimatization
Although as pointed out above, the hyperventilation of acclimatization ameliorates the
hypoxia of high altitude to some extent, it is very important to emphasize that the oxyge n levels
in the alveolar gas, arterial blood and body tissues are still very low. There seems to be a
misconception among some astronomers who argue that acclimatization to high altitude reverses
all of its deleterious effects. This is a dangerous error.
One way of emphasizing this is to compare the oxygen deprivation of astronomers at high
altitude with that seen in patients with severe lung disease. Figure 1 shows that the threshold for
administering continuous oxygen therapy to patients who have chronic obstructive pulmonary
disease (a very common condition including chronic bronchitis and emphysema) is a PO2 of 55
torr. Actually this is the arterial PO2 because the alveolar value is difficult to measure in the
presence of severe lung disease. In normal subjects at high altitude the arterial PO2 is about 2-5
torr below the alveolar value. However if we assume the best case, that is that the alveolar and
arterial PO2 are the same, some surprising results emerge from Figure 1. This shows that
astronomers who are fully acclimatized on the summit of Mauna Kea have an alveolar PO2 of
slightly less than the threshold for continuous oxygen therapy. In other words, if these people
had the same degree of oxygen deprivation at sea level caused by lung disease, they would be
entitled to continuous oxygen therapy under Medicare (U.S. federal health insurance program).
The same criterion is used by the N.H.S. in the U.K. Moreover extensive studies have now
shown that continuous oxygen therapy in these patients who have an arterial PO2 of less than 55
torr results in improvements in neuropsychological function measured when they are breathing
air12. This demonstration of the value of continuous oxygen therapy in patients with severe
hypoxia explains the large number of oxygen concentrators in patients’ homes. The studies also
emphasize the extent to which even fully acclimatized astronomers on the summit of Mauna Kea
are impaired by the oxygen deprivation. It makes little sense to argue that these people would not
Only a brief discussion of these is given here because they are fully covered in major
medical textbooks2 and smaller books designed for climbers and trekkers13,14.
5.1. Acute Mountain Sickness (AMS)
This is very common in people who go to altitudes over about 3000 m and is
characterized by headache, breathlessness, fatigue, insomnia, loss of appetite, nausea, dizziness
and palpitations. Most of the symptoms begin a few hours after ascent and disappear after two or
three days although the difficulties with sleeping often remain. No treatment is necessary
although aspirin, acetaminophen (Tylenol) or ibuprofen (Advil) may be useful for the headache.
Symptoms improve with rest and in occasional severe cases it may be necessary to descend.
Acetazolamide (Diamox) reduces the incidence of acute mountain sickness by stimulating
ventilation. The dose is 250 mg once or twice a day beginning on the morning of the ascent or
the day before. A small dose of acetazolamide such as 125 mg taken at night often improves
sleep. The drug has several side effects including increased urination, tingling of the fingers and
toes, and making carbonated beverages taste flat. It should only be taken if needed and is a
5.2. High-Altitude Pulmonary Edema (HAPE)
This is a serious illness in which fluid moves out of the pulmonary capillaries into the air
spaces of the lungs. The main symptom is increased shortness of breath and this frequently
becomes worse at night. A physician can hear crackling sounds in the lung by using a
stethoscope. The condition may progress to the point where the patient coughs up prink frothy
This is a medical emergency and necessitates removing the patient to lower altitude as
soon as possible. Oxygen should be given if this is available but descent is imperative.
Astronomers working at high altitude should adopt the “buddy” system so that someone is
always available to help a sick person. Another wise precaution is to have two vehicles always
available in case of mechanical difficulties.
5.3. High-Altitude Cerebral Edema (HACE)
This is a serious but fortunately rare condition where fluid leaks out of capillaries into the
brain tissue. It often begins like acute mountain sickness but progresses to loss of balance,
difficulties with walking, clouding of consciousness, irrational behavior and coma. The patient
should be immediately removed to low altitude and given oxygen if this is available. The
incidence of AMS, HAPE and HACE all increase as the altitude is raised.
6. Use of Supplementary Oxygen at High Altitude
As we have seen, all the medical effects of high altitude are caused by the low partial
pressure of oxygen in the inspired air. It should therefore come as no surprise tha t the best way to
counter the oxygen deprivation of high altitude is to add oxygen to the inspired air. There have
been important technological advances in the last few years that have improved our ability to do
this, the most significant being oxygen enrichment of rooms in which astronomers work.
It appears that among a small minority of astronomers there remains a prejudice against
the use of supplementary oxygen. The common objections are that: 1) it is not necessary and “I
can function perfectly well without it;” 2) it is technically too complicated and expensive to
install; and 3) it is dangerous because of the fire hazard. None of these objections is valid. On the
first, there is ample evidence that at altitudes of 5000 m and above, mental and physical
performance are impaired. This is not so obvious at the lower altitude of 4200 m, and it is not
easy to document for the reasons given earlier. However there is a wealth of evidence that people
lose mental efficiency at that altitude, they make more errors, and they fatigue more rapidly. All
these problems can be greatly helped by oxygen enrichment. The second objection that oxygen
enrichment is technically difficult and expensive has been disproved by field trials over the last
few years, one of the most convincing being that of the Caltech Cosmic Background Imager.
Finally the fire hazard has been analyzed in great detail and simply does not exist if appropriate
precautions are taken (see later). Here it should be emphasized that although the atmosphere is
being oxygen-enriched, the resulting PO2 is still much lower than the sea level value, and the fire
6.1. Oxygen Enrichment of Room Air
Oxygen enrichment of room air was suggested almost twenty years ago by Cudaback3 in
connection with telescope facilities on Mauna Kea but was never implemented. Since then there
have been substantial technical advances. The subject been discussed at length elsewhere15 and
so only the main points will be covered here. The simplest way to introduce it is to describe a
typical room used by astronomers from the California Institute of Technology for their Cosmic
Background Imager at an altitude of 5050 m in north Chile.
The control room and laboratory each consist of a standard shipping container (7 ft × 7 ft
× 40 ft) which are lined with insulation which is sufficient to maintain a 40ºC temperature
difference with a 1 kW heater, and provided with lighting and electrical outlets. The living
quarters are similarly outfitted, but of half the length. The room is entered through a double door
that forms an airlock. Ventilation is by means of a pipe that extends from the door end to the far
end of the room, and there is an exit port near the door. Fresh air is drawn into the ventilation
duct by a variable electric fan. Oxygen is injected from the concentrators into a separate duct
which extends the length of the room and has multiple outlets. The oxygen concentrators are
located outside the room but in a protected compartment inside the container. The principle of
the concentrators is that when air is pumped into a tube of synthetic zeolite at high pressure,
nitrogen is preferentially adsorbed and the effluent gas has an oxygen concentration of 90-95%.
After a short period the zeolite is unable to adsorb more nitrogen and the high pressure air is
switched to a second tube while the first tube is purged of nitrogen using air at normal pressure.
The only moving parts in the oxygen concentrator are a piston pump and the switching valve. A
typical model is the AirSep New Life Elite (AirSep Corp., Buffalo, NY) which provides 5 l.min-1
of 90-95% oxygen but similar devices are available from other manufacturers. These oxygen
concentrators are used by the thousands in private homes to provide oxygen for patients with
severe lung disease and are robust, self-contained, and require only 350 watts of electrical power.
The cost of each unit is about $1,000. A typical room at the CBI with two occupants requires
four of these units in parallel to raise the oxygen concentration of the room air from 21 to 27%. It
is also possible to supply oxygen from liquid oxygen tanks but the running costs are about ten
The ventilation level of the room is maintained at the minimum acceptable level to reduce
the amount of oxygen that has to be generated. We use the ASHRAE (American Society of
Heating, Refrigerating, and Air Conditioning Engineers) 1975 standard which is 8.5 m3.h-1 per
person. The carbon dioxide concentration in the room is monitored and kept at or below 0.3%
(the concentration in air is about 0.03%). Substantially higher concentrations of CO2 in the room
can be present without causing a health hazard, or without the occupants being aware of them,
but the CO2 level is a useful index of the adequacy of ventilation. The oxygen concentration of
An oxygen concentration of 27% in the room was chosen to reduce the equivalent
altitude to 3200 m. (The equivalent altitude is that which provides the same inspired PO2 for a
person who is breathing air.) Since the astronomers are living at San Pedro de Atacama (altitude
2440 m) and therefore will be acclimatized to this altitude, the increase in altitude to 3200 m is
easily tolerated. It would be possible to raise the oxygen concentration of the room to about 32%
without the fire hazard exceeding that of sea level air, but there is little point in doing this. The
costs of oxygen enrichment in this facility are small. The four oxygen concentrators require only
1400 watts of power, a minor drain in the context of a sophisticated telescope facility.
Sometimes the question comes up as to whether someone leaving an oxygen-enriched room and
going into ambient air will feel dizzy, faint, or suffer in some other way. The answer is that
people are completely unaware of either entering or leaving the oxygen-enriched environment
Additional information should be given about the possible fire hazard since this issue is
frequently raised. The fire hazard in oxygen-enriched atmospheres has been analyzed in detail by
the National Fire Protection Association16. They concluded that an atmosphere of increased
burning rate for various materials including paper and fabrics is one that contains a percentage of
oxygen greater than 23.5/P0.5, where P is the total pressure as a fraction of the sea level pressure.
Based on extensive experimental studies it can be shown that an oxygen concentration of 27% at
an altitude of 5050 m gives a burning rate that is approximately 70% of the sea level value17. The
primary reason is that although oxygen has been added to the atmosphere, the PO2 is still far
below that of air at sea level. Note that the PN2 also has an effect on burning rate because of its
quenching action. Even so, common sense dictates that there should be no cigarette smoking or
use of flammable gases and liquids in the oxygen-enriched room. Also volatile liquids require
special handling because there is some evidence that they may ignite more easily at high altitude,
and their vapors may spread more readily than at sea level. As long as these limitations are borne
in mind they should not cause any great inconvenience.
Extensive studies on oxygen enrichment of room air have been carried out at the
University of California White Mountain Research Station (altitude 3800 m). They have shown
that some aspects of neurophysiological function will be improved at an altitude of 5000 m with
27% oxygen enrichment18. A series of studies have also been carried out on the effects of oxygen
enrichment on sleep and all these have shown substantial benefits19,20. But probably the most
convincing evidence of the value of oxygen enrichment at 5050 m comes from the experience of
the astronomers in the CBI project. Their experience has been summarized as follows:
The CBI was designed and constructed on the Caltech campus and tested there
for a year before disassembly and shipping to Chile in August 1999. The same
group was responsible for the reassembly on Chajnantor. For the first 10 days of
telescope assembly we did not have oxygen and we tired quickly under even
modest physical labor, and suffered from cold in the ~15 m.sec-1 and ~-5ºC
conditions. Our fingers soon became numb, making construction work difficult.
After an 8 hour shift at 5050 m we were completely exhausted and slept for ~12
hours. On day 11 we were for the first time able to use our portable oxygen units,
and two senior group members began using supplemental oxygen and their
efficiency improved remarkably. Physiologically the contrast with the preceding
10 days was striking - it was possible to work normally; heavy lifting and carrying
were much easier, and the problems with cold were much diminished. It was now
possible to work without gloves for significant periods before fingers were too
numb to continue, and fingers regained feeling much more rapidly than without
An interesting psychological factor was that, in spite of the extensive
discussions of the use of oxygen the group had had and the planning for the use of
oxygen prior to moving to Chile, once we were engaged in the construction in
Chile there was significant resistance to the use of oxygen from group members
who felt that they would do better to get acclimatized. A few days of working
alongside those using oxygen quickly disabused them of this misconception.
Astronomical projects planning to work at high altitude should be aware of the
inherent resistance to the use of oxygen, and the “macho ” view that it is not
necessary. Unfortunately it is not easy when not on supplemental oxygen to assess
one’s own performance unless doing heavy physical work alongside someone
who is using supplemental oxygen. Our experience led us to lay down strict rules
regarding the use of oxygen on the project which were that no work should be
done on the telescope, the power plant, in the machine shop or with power tools
without the use of oxygen. Each member of the group has his or her own portable
oxygen unit. We also always carry these units with us driving to and from the site
in case of need while driving, which does happen occasionally.
After 3 weeks the site facilities were ready for use with enriched oxygen in the
control building, the laboratory and two living quarters, and from that time on the
difficulties of working at altitude were greatly reduced. Having oxygen-enriched
sleeping quarters has proven important for observing with the CBI - in general we
do not spend long periods at the site, but on occasion astronomers have spent 4-5
days continuously at the site with no ill effects. In addition our drivers generally
sleep at the site while the astronomers are observing, and they get a good sleep in
the oxygenated containers, thus ensuring that they are rested and alert for the
There were a number of physiological effects due to working at high altitude
which were noticed by members of the CBI group. These depended on the amount
of time which was spent at high altitude as well as on the wind chill. It would be
hard to over emphasize just how much the use of oxygen helps in coping with
both the wind an cold at high altitude. Conditions which become intolerable in
~15-20 minutes without supplemental oxygen can be tolerated for some hours
with the use of supplemental oxygen. This has been experienced many times in
The most common physiological effects of high altitude are breathlessness,
irritability, headaches, nausea and poor judgment. We quickly realized that
heightened irritability was a factor and that in instances of disagreement the
discussion should be deferred. In addition, lack of judgment was a significant
factor. Although irritability was much reduced and judgment much improved in
the oxygenated containers, we decided early on to take a cautious approach and
defer discussion of controversial topics until we returned to our base in San
Pedro; and we also learned to check the most critical decisions with staff in San
Some people have voiced concerns that one might feel at a disadvantage if
one moves directly from an oxygen-enriched room to the outside and also that
acclimatization might be significantly slower if one uses supplemental oxygen. At
the CBI we do this frequently, of course, and we have not experienced any
A number of minor symptoms of working at altitude were also experienced by
some members of the group. Some of these symptoms were related to
1) Loss of appetite. This depended strongly on the amount of time spent at high altitude.
2) Loss of body weight. This was related to (1) and was so severe in some cases that
people with a usual body weight of 150 lb to 170 lb lost 15 lb to 20 lb of body weight.
3) Bright flashing arcs of light in the peripheral vision when blinking, possibly due to
dehydration of the vitreous humor, which led to the retina being stretched. This was
cured by drinking 6-8 glasses of water each day.
4) Fingernails separating from the skin further down the nail than usual and the tops of
nails becoming very white. Finger ends tended to crack and split and take longer than
usual to heal. This was only a problem for people spending a lot of time at high
altitude and working in very cold conditions.
5) Constipation. This was a serious problem for some group members.
Table III shows the results of oxygen enrichment at various sites of interest to
astronomers. At the lowest site, the Barcroft Facility of the White Mountain Research Station
where much of the early work on oxygen enrichment was carried out, the altitude is only 3800 m
and the oxygen concentration in the room is 24%. This gives an equivalent altitude of 2800 m
and an alveolar PO2 of about 68 torr. The table shows how the oxygen concentration is increased
for higher altitudes. For example, at Chajnantor (altitude 5050 m) the oxygen concentration used
by the Cosmic Background Imager group is 27% giving an equivalent altitude of about 3200 m.
At the highest altitude of 5800 m, the oxygen concentration is 30% also giving an equivalent
altitude of 3200 m. The values for alveolar PO2 with oxygen enrichment are also shown on
The maximum safe oxygen concentrations at the four altitudes are also shown in Table
III. Note that in every case it would be possible to safely increase the oxygen concentration and
thus reduce the equivalent altitude. However there is little to be gained by reducing the
equivalent altitudes any further because these are easily tolerated. The chosen values represent a
good compromise between a comfortable altitude, the cost of providing oxygen, and the possible
It is important to recognize that each situation of high altitude astronomical observations
is unique, and therefore the use of oxygen must be adapted to the particular needs and
applications of the project. In general, it would be better if astronomers did not have to work at
the telescope site, and if a small staff could carry out the vital operations which require physical
presence at the site. In such situations, the staff would benefit from the same type of facilities as
have been set up for the CBI, and supplemental oxygen should certainly be made available.
6.2. Portable Oxygen
Of course oxygen enrichment of room air as described above can only be used in closed
spaces. Frequently staff have to work on equipment outside closed spaces and portable oxygen
can be valuable here. A small portable oxygen cylinder is used and the oxygen is delivered via
cannulas that are placed just inside the nostrils. Admittedly this is more cumbersome than
oxygen enrichment of room air where the astronomer is not aware of the fact that he or she is
using supplemental oxygen. The experience at the CBI has been that while portable oxygen is
not as convenient, it is essential, and the awkwardness of carrying an oxygen cylinder is well
worth it. In constricted spaces, the cylinder and controller can generally be placed close enough
to the work area to allow the continued use of oxygen, thus greatly increasing both comfort and
efficiency. However portable oxygen is used by thousands of patients with severe lung disease
and is certainly feasible. The equipment includes an economizer that senses the pressure in the
cannulas so that when this falls slightly at the beginning of inspiration, a pulse of oxygen is
delivered. Again the experience of the astronomers at the CBI is that portable oxygen greatly
There are good scientific reasons to site telescopes at altitudes of 5000 m and above, but
these altitudes can seriously impair human mental and physical performance and quality of sleep.
However the introduction of oxygen concentrators which allow oxygen enrichment of the air in
the rooms where the astronomers wo rk or sleep makes high-altitude astronomy feasible. The
technique is not expensive, and because it increases the efficiency of the astronomers, the benefit
in relation to cost is substantial. As indicated above, the only running cost of oxygenating a
module at the CBI is that of providing 1400 watts of electrical power. Moving from an oxygen-
enriched environment to ambient air at high altitude causes no serious problems. A common
misconception within the astronomy community is that acclimatization to high altitude removes
the deleterious effects of oxygen deprivation, but this is a fallacy. Oxygen enrichment of room
air has been used by the California Institute of Technology Cosmic Background Imager at an
altitude of 5050 m for four years with considerable success. The technique could also be used at
more modest altitudes such as that of Mauna Kea (4200 m) with consequent improvements in
This work was supported by NIH grant RO1 HL 60698.
1. T. F. Hornbein, & R. B. Schoene, High Altitude: An Exploration of Human Adaptation
2. M. P. Ward, J. S. Milledge, & J. B. West, High Altitude Medicine and Physiology, 3rd ed.
3. D. M. Cudaback, PASP, 96, 463, 1984.
4. P. J. G. Forster, PASP, 96, 478, 1984.
5. W. L. Putnam, & C. S. Houston, Mercury, 24, 32, 1995.
6. P. J. Napier, & J. B. West, MMA Memo No 162, <http://www.mma.nrao.edu/memos/html-
memos/alma162/memo162.html>, Oct. 10, 1996.
7. J. B. West, F. L. Powell, & A. M. Luks, MMA Memo No 192,
<http://www.mma.nrao.edu/memos/html- memos/alma191/memo191.html>, 1997.
8. ICAO, Manual of the ICAO Standard Atmosphere (Int. Civil Aviation Org., Montreal,
9. J. Barcroft, et al., Phil Trans R Soc Lond Ser B, 211, 351, 1923.
10. V. M. Sharma, M. S. Malhotra, & A. S. Baskaran, Erg, 18, 511, 1975.
11. H. Rahn, & A. B. Otis, AJP, 157, 445, 1949.
12. Nocturnal Oxygen Therapy Trial Group, Ann Int Med, 93, 391, 1980.
13. P. H. Hackett, Mountain Sickness (American Alpine Club, New York), 1978.
14. A. J. Pollard, & D. R. Murdoch, The High Altitude Medicine Handbook, 3rd ed. (Radcliffe
15. J. B. West, High Alt Med Biol, 3, 223, 2002.
16. National Fire Protection Association, Standard for Hypobaric Facilities, 1999 Edition,
NFPA 99B (National Fire Protection Association, Quincy, MA), 1999.
17. J. B. West, Aviat Space Environ Med, 68, 159, 1997.
18. A. Gerard, et al., High Alt Med Biol, 1, 51, 2000.
19. A. M. Luks, et al., Resp Phys, 113, 247, 1998.
20. M. K. McElroy, et al., High Alt Med Biol, 1, 197, 2000.
21. R. A. McFarland, in: (ed.)M. K. Yousef, S. M. Horvath, & R. W. Bullard (eds.),
Physiological Adaptations: Desert and Mountain (Academic Press, New York), 1972,
Alveolar PO2 values for people at high altitude who are acutely exposed (no
acclimatization) or fully acclimatized. The data for these two lines come from
Rahn and Otis11. Note that all the values are far below the normal sea level value
of 100 torr. The lower broken line at a PO2 of 55 torr indicates the value below
which patients with severe lung disease at sea level are entitled to continuous
oxygen therapy under Medicare or the N.H.S. (This is actually the arterial PO2
which in normal subjects is 2-3 torr below the alveolar value and the diagram
shows the best case.) Note that an astronomer on the summit of Mauna Kea who
is completely acclimatized, a process that takes about 10 days, will nevertheless
have a PO2 below the value which entitles him or her to continuous oxygen
therapy at sea level if he has lung disease. Typical alveolar PO2 values for oxygen
enrichment are also shown according to the oxygen concentrations shown in
Table III. The inspired PO2 is shown by the uppermost broken line. COPD,
chronic obstructive pulmonary disease; PaO2, partia l pressure of O2 in arterial
Inspired partial pressure of oxygen (PO2) at various altitudes
Mental ability expressed as a fraction of ability at sea level for unacclimatized
Attention Short Term Arithmetic Decision Making
Effects of oxygen enrichment at various high altitude sites
Pretreatment for Nerve Agent Exposure Chapter 6 PRETREATMENT FOR NERVE AGENT EXPOSURE MICHAEL A. DUNN, M.D., FACP*; BRENNIE E. HACKLEY, JR., PH.D.†; AND FREDERICK R. SIDELL, M.D.‡ INTRODUCTION AGING OF NERVE AGENT–BOUND ACETYLCHOLINESTERASE PYRIDOSTIGMINE, A PERIPHERALLY ACTING CARBAMATE COMPOUND Efficacy Safety Wartime Use Improved Delivery CENTRALLY ACTING NERVE AGENT
The Medical Flexible Spending Account is used for tax-deductible health care expenses not paid by insurance for yourself, your spouse and anyone you claim as a dependent on your federal income tax return. On this page, we provide a partial list of eligible expenses you may be reimbursed for through your Medical Flexible Spending Account (FSA) as well as a list of ineligible expenses. Page 2 i
 Inspired partial pressure of oxygen (PO2) at various altitudes
Mental ability expressed as a fraction of ability at sea level for unacclimatized
Attention Short Term Arithmetic Decision Making
Effects of oxygen enrichment at various high altitude sites
Inspired partial pressure of oxygen (PO2) at various altitudes
Mental ability expressed as a fraction of ability at sea level for unacclimatized
Attention Short Term Arithmetic Decision Making
Effects of oxygen enrichment at various high altitude sites