FERTILITY AND STERILITY VOL. 79, NO. 3, MARCH 2003Copyright 2003 American Society for Reproductive MedicinePublished by Elsevier Science Inc. Printed on acid-free paper in U.S.A. Luteal estradiol administration strengthens the relationship between day 3 follicle- stimulating hormone and inhibin B levels and ovarian follicular status Renato Fanchin, M.D.,a Joa˜o Sabino Cunha-Filho, M.D.,a Luca Maria Schona¨uer, M.D.,aClaudia Righini, M.D.,a Dominique de Ziegler, M.D.,b and Rene´ Frydman, M.D.a
Department of Obstetrics and Gynecology and Reproductive Medicine, Hoˆpital Antoine Be´cle`re, Clamart,FranceObjective: To investigate whether the prevention of early follicular growth by luteal E administration
improves the relationship between day 3 hormone measurements and the ovarian follicular status. Design: Prospective, cohort study. Setting: Assisted reproductive technology unit in Clamart, France. Patient(s): One hundred sixty-two infertile women. Intervention(s): Participants received oral 17-E , 4 mg/day, from day 20 to the next cycle day 1 (n ϭ 81)
or served as controls (n ϭ 81). Serum E , inhibin B, and FSH were measured during the 3 days after E
discontinuation (FD1, FD2, and FD3) in E -treated women and on cycle day 3 (CD3) in controls. Early antral
follicles were counted at ultrasound scans on FD3 and CD3. Main Outcome Measure(s): Hormonal-follicular correlations on FD3 and CD3. Result(s): As expected, after E withdrawal, inhibin B and FSH increased from FD1 to FD3 whereas E
decreased. Correlations between FSH and inhibin B and follicular counts were stronger on FD3 than on CD3. Conclusion(s): Luteal E administration notably strengthens the relationship between serum FSH and inhibin
B levels and the number of antral follicles on day 3. This approach may represent an alternative test of ovarian follicular status. (Fertil Steril 2003;79:585–9. 2003 by American Society for Reproductive Medicine.) Key Words: FSH, estradiol, ovarian reserve, controlled ovarian hyperstimulation
During the luteal-follicular transition, in-
During the ultimate phase of the menstrual
cycle, there is a progressive increase in FSH
early antral follicles modulate their own stim-
levels that parallels the corpus luteum demise
ulation by FSH. Given that reproductive aging
and starts up to 5 days before the onset of
is characterized by the quantitative depletion of
premenstrual exposure of early antral follicles
consequent reduction in peripheral inhibin B
to FSH may accelerate their development dur-
and E concentrations amplifies intercycle FSH
ing the first days of the follicular phase
secretion, which culminates 2 to 3 days after
Because larger follicles are likely to produce
sible that such a phenomenon interferes with
FSH secretion, thereby altering the predictabil-
widely used as markers of ovarian status and
ity of peripheral day 3 FSH and inhibin B
responsiveness to controlled ovarian hyper-
measurements on the ovarian follicular status.
dence indicates that these hormone measure-
Based on this contention, it is conceivable
ments, arbitrarily timed to the onset of menses,
that the suppression of FSH secretion during
offer only a pale reflection of women’s fecun-
the late luteal phase could avoid premature
development of early antral follicles and im-
prove the reliability of hormonal measurements. Indeed, the
previously described For inhibin B, the lower limit of
administration of physiological E doses during the luteal-
detection was 10 pg/mL, and the intraassay and interassay
follicular transition has been shown to effectively prevent
CV were Ͻ6% and Ͻ9%, respectively. Serum E was de-
intercycle FSH rise and, consequently, untimely follicular
termined by an automated multianalysis system using a
growth In addition, after E discontinuation, FSH
chemiluminescence technique (ACS-180, Bayer Diagnos-
levels increase rapidly and peak 3 days later Hence,
tics, Puteaux, France). For E , the lower limit of detection
we hypothesized that the control of early antral follicular
was 15 pg/mL, and intraassay and interassay CV were 8%
development by exogenous E would be instrumental in
and 9%, respectively. The specificity of the FSH, inhibin B,
strengthening correlations between FSH and inhibin B levels
and E assays was 100%, 99.5%, and 100%, respectively.
measured on day 3 and the ovarian follicular status. Ultrasound Monitoring
Both on FD3 and on CD3, ultrasounds scans of the
MATERIALS AND METHODS
ovaries were performed with a 4.5–7.2 MHz multifrequencytransvaginal probe (Siemens Elegra, Siemens S.A.S., Saint-
Patients
Denis, France) by one single operator (C.R.) at approxi-
We prospectively studied 162 infertile women, 27 to 44
mately 9:00 AM. The objective of these examinations was to
years of age who met the following inclusion criteria: 1)
count the total number of early antral follicles (2 to 8 mm in
regular, ovulatory menstrual cycles every 25 to 35 days; 2)
diameter) in both ovaries. The operator was unaware of both
both ovaries present; 3) no current or past diseases affecting
treatment schedule and hormonal results. In an attempt to
ovaries or gonadotropin or sex steroid secretion, clearance,
optimize recognition of ovarian follicles, the ultrasound
or excretion; 4) body mass indexes ranging from 18 to 25
scanner used was equipped with a tissue harmonic imaging
kg/m2; 5) no current hormone therapy; and 6) adequate
system Tissue harmonic imaging is based on ultrasound
visualization of ovaries in transvaginal ultrasound scans.
signal frequency changes during propagation through the
Infertility was unexplained (69%), or due to sperm (21%) or
target media. This change is called a harmonic and is essen-
mild tubal (9%) abnormalities. An informed consent was
tially a doubling of the original frequency. Hence, the re-
obtained from all women and this investigation received the
turning high frequency signal has to only travel one direction
approval of our internal institutional review board.
(return to the probe), which enhances signal penetration,
Study Protocol
reduces near field noise and image haze, and provides in-
Participants either received luteal E treatment or served
as controls. Women included in the E -treated group (n ϭ
Statistics
81) were given oral micronized 17-E (4 mg/day; Pro-
The measure of central tendency used for continuous
vame`s, Cassenne Laboratories, Puteaux, France) in the
variables was the mean and the measure of variability was
evening at 8:00 PM, from day 20 until day 1 of the next cycle.
the standard error of the mean. Longitudinal hormonal
To document the hormonal profile following E discontinu-
changes were assessed by analysis of variance with repeated
ation, serum FSH, inhibin B, and E levels were measured on
measures or paired Student’s t-test when appropriate. Rela-
the 3 subsequent days referred to as functional days (FD):
tionship between two different continuous variables were
FD1, FD2, and FD3, respectively. On FD3, early antral
assessed by correlation. The Fisher r to z test was used to
follicles were counted at ultrasound scans. Women included
determine if correlation coefficients (r) were different from
in the control group (n ϭ 81) did not receive any treatment
zero. Comparison of strength of correlations was performed
during the luteal phase and had similar hormonal and ultra-
using the Hotelling’s t-test which assesses the differ-
sonographic measurements on the third day of the subse-
ence between coefficients of correlation for correlated sam-
quent cycle, referred to as cycle day (CD) 3. Women in both
ples. PϽ.05 was considered statistically significant.
groups were asked to compute the length of the menstrualcycle studied. Hormonal Measurements
All blood samples were obtained by venipuncture, per-
Overall Data
formed at approximately 8:00 AM, and serum was separated
As expected by design, E -treated and control groups
and frozen in aliquots at Ϫ20°C for subsequent centralized
were strictly comparable in regard to mean women’s ages
analysis. Serum FSH levels were determined by an auto-
(33.9 Ϯ 0.4 vs. 33.6 Ϯ 0.5 years, respectively), frequency
mated multianalysis system using a chemiluminescence
distributions of causes of infertility (unexplained, 68% and
technique (ACS-180, Bayer Diagnostics, Puteaux, France).
70%; sperm abnormalities, 22% and 21%; mild tubal alter-
Intraassay and interassay coefficients of variation (CV) were,
ation, 9% and 9%, respectively), and early antral follicular
respectively, 3% and 5%, and the lower limit of detection
counts (10.1 Ϯ 0.7 follicles on FD3 and 10.6 Ϯ 0.6 follicles
was 0.1 mIU/mL for FSH. Serum inhibin B was determined
on CD3). In addition, the number of early antral follicles and
by double antibody ELISA (Serotec, Varilhes, France) as
women’s ages showed similar negative correlations in E -
Fanchin et al.
treated as in control groups (r ϭ Ϫ0.41, PϽ.0001 and r ϭ
Ϫ0.39, PϽ.0001, respectively). The mean length of the
preceding cycle was not altered by luteal E administration
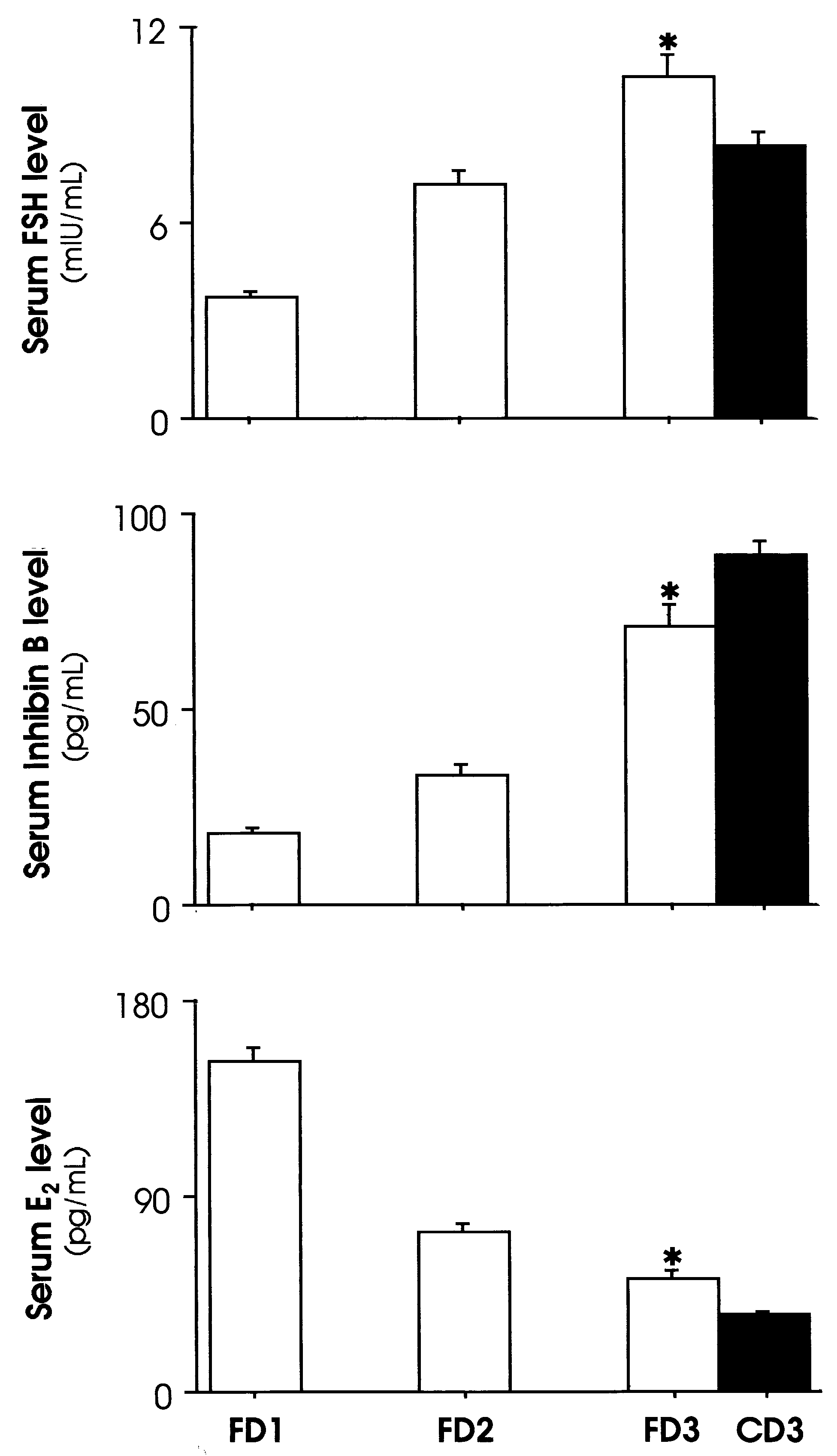
Serum FSH (top panel), inhibin B (middle panel), and E
and remained similar in both groups (28.1 Ϯ 0.2 versus
(bottom panel) profiles during the first 3 days after E discon-
28.2 Ϯ 0.2 days, respectively). However, the subsequent
tinuation (FD1, FD2, and FD3) in the E -treated group. Both
menstrual cycles lasted slightly, but significantly, longer in
the progressive elevation in FSH and inhibin B levels, as wellas the decrease in E levels, from FD1 to FD3 were statisti-
the E -treated women (29.1 Ϯ 0.2 days) than in the controls
cally significant (open bars, PϽ.0001). Hormone levels on
FD3 were significantly different as compared to controls(CD3, closed bars, *PϽ.0001).
The hormonal dynamics after exogenous E discontinua-
tion in the E -treated group as well as the comparison of
hormone levels between FD3 and CD3 are depicted in Serum FSH levels were low at 3.8 Ϯ 0.2 mIU/mL onthe first day of E withdrawal (FD1) and increased progres-
sively on FD2 (7.2 Ϯ 0.4 mIU/mL) and FD3 (10.5 Ϯ 0.6mIU/mL) (PϽ.0001). It is noticeable that FSH levels weresignificantly higher on FD3 than on CD3 (8.3 Ϯ 0.4 mIU/mL, PϽ.0006). Similarly to FSH, serum inhibin B levelswere low on FD1 (18.6 Ϯ 1.1 pg/mL) and increased pro-gressively from FD2 to FD3 (33.2 Ϯ 2.9 and 71.2 Ϯ 5.6pg/mL, respectively) (PϽ.0001). Yet serum inhibin B levelson FD3 were lower than inhibin B levels on CD3 (90.0 Ϯ 3.6pg/mL, PϽ.006). Further, E administration maintained se-
rum E at levels comparable to those observed during the late
follicular phase of the menstrual cycle as measured on FD1(152.7 Ϯ 5.9 pg/mL). After oral treatment was discontinued,serum E levels decreased progressively (73.6 Ϯ 4.2 and
52.2 Ϯ 3.2 pg/mL, on FD2 and FD3, respectively)(PϽ.0001). Serum E levels were higher on FD3 than on
CD3 (34.3 Ϯ 2.3 pg/mL, PϽ.0001), presumably as a resultof exogenous and endogenous contributions. Follicular and Hormonal Relationships
The strength of the correlations between serum hormone
levels on FD3 (E -treated group) and on CD3 (control group)
and early antral follicular counts are summarized in Table 1. Serum FSH levels showed a stronger negative correlationwith the number of early antral follicles on FD3 (r ϭ Ϫ0.44,PϽ.0001) than on CD3 (r ϭ Ϫ0.23, PϽ0.04). Comparisonof strength of correlations indicated that this difference wasstatistically significant (PϽ.02). Similarly, the correlationbetween serum inhibin B levels and early antral follicularcounts was stronger (PϽ.001) on FD3 (r ϭ 0.59, PϽ.0001)than on CD3 (r ϭ 0.24, P Ͻ.03). In contrast, serum E levels
failed to correlate with early antral follicular counts on eitherFD3 or CD3. Furthermore, serum FSH and inhibin B were
Fanchin. FSH and inhibin B elevation timed by E . Fertil Steril 2003.
correlated to each other only in patients who were pretreatedwith E (r ϭ Ϫ0.30, PϽ.0007 vs. r ϭ Ϫ0.07, PϾ.05). This
measurements performed on cycle day 3. The objective of E2
difference was statistically significant (PϽ.02).
administration was to control the timing of FSH elevationduring the luteal-follicular transition to prevent premature
DISCUSSION
follicular development and, therefore, optimize hormonal-
The results of the present investigation indicate that the
magnitude of FSH and inhibin B elevation timed by luteal E
Indeed, previous data have demonstrated that, during the
administration is better correlated to the ovarian follicular
late luteal phase of the menstrual cycle, spontaneous demise
status than conventional, uncontrolled FSH and inhibin B
of the corpus luteum leads to a progressive FSH rise that
FERTILITY & STERILITY
starts approximately 5 days before menses and reach
that observed after profound FSH suppression by GnRH
serum levels Ͼ7 mIU/mL 3 days before the onset of men-
agonist administration and subsequent FSH treatment as
strual bleeding On account of the enhanced sensitivity of
reported previously This strengthens the hypothesis
early antral follicles to FSH during the late luteal phase
that similar follicular status may be obtained after FSH
it is presumable that luteal FSH secretion hastens the
suppression by exogenous E as compared to pituitary de-
pace of follicular development In addition, this phe-
nomenon has been reported as being more striking in women
In addition, it is noteworthy that serum inhibin B levels
who display some degree of follicular exhaustion and de-
were lower on FD3 as compared to CD3. Given that inhibin
clined fecundity Our data confirmed that administration
secretion also depends on follicular sizes it is
of physiological E doses during the late luteal phase effec-
possible that early antral follicles were smaller in E -treated
tively maintained FSH secretion at low levels (3.8 Ϯ 0.2
patients as compared with controls. In line with this, men-
mIU/mL on FD1), which is in keeping with results reported
strual cycles lasted longer in women who were pretreated
with E , possibly due to a longer growth course of smaller
As expected, a dramatic FSH elevation occurred during
antral follicles to ovulation. An analogous phenomenon has
the 3 subsequent days after E withdrawal. Interestingly,
been observed in E -treated monkeys Unfortunately,
serum FSH levels were significantly higher on FD3 than on
the design of the present study did not include antral follic-
CD3. Some elements led us to infer that these differences
ular size measurements, which prevents us from making any
were neither phenomenological nor due to patient heteroge-
conclusion on this point. This issue is currently being inves-
neities. Indeed, our experimental design required population
selection, randomization, and blinded measurements; also,
Furthermore, no evidence of increasing E production as
clinical and ultrasonographic attributes of patients were re-
a result of endogenous FSH stimulus was observed in the
markably similar in both groups. Taken together, these meth-
E -treated group. In response to FSH, E secretion by the
odological characteristics minimized as far as possible the
early antral follicles is scarce and variable, probably due to
likelihood that individual discrepancies accounted for the
the incipient aromatase activity in early antral follicles
observed hormonal differences. Moreover, these results cor-
In agreement, serum E levels correlated with the
roborate previous experiments conducted in rhesus monkeys,
number of early antral follicles on neither FD3 nor CD3,
in which removal of E administration during the follicular
which challenges the reliability of day 3 E measurements
phase led to larger FSH release as compared to untreated
for prognosticating antral follicular reserve. Yet endogenous
E secretion by antral follicles participates in the regulation
Hence, it is conceivable that FSH level differences be-
of FSH levels. Hence, the lack of mutual FSH and inhibin B
tween FD3 and CD3 result from luteal E administration
correlation in the untreated group is consistent with the
through a number of mechanisms. First, the overall reduced
varying E production by antral follicles displaying hetero-
inhibin B and E secretion by small early antral follicles is
likely to insufficiently suppress FSH secretion. Indeed, our
The central observation of the present study was the more
results indicated that inhibin B levels were very low on the
strict correlation between the magnitude of FSH and inhibin
day after E withdrawal (FD1) and reached lower levels on
B rise timed by E administration and the number of early
FD3 than on CD3. Second, whereas FD3 corresponded pre-
antral follicles as compared to controls. This indicates that
cisely to the third day of FSH elevation in E -treated pa-
the control of follicular exposure to FSH by E administra-
tients, the timing of FSH elevation could not be directed in
tion may refine the analysis of hormonal-follicular relation-
controls. Hence, on CD3, serum FSH levels may have been
ships, commonly timed to the onset of menses, and improve
influenced by the stage of follicular growth in untreated
their clinical usefulness. Indeed, it is conceivable that the
women. Finally, the putative negative feedback effect of
putative prognostic value of early antral follicular counts
prolonged E treatment on GnRH pulse characteristics
on women’s fertility and responsiveness to controlled
and/or on pituitary gonadotropin secretion could have
ovarian hyperstimulation may be further improved by con-
elicited a select favoritism of FSH beta expression in E -
treated patients. However, this issue deserves further clari-
In conclusion, the intercycle FSH and inhibin B rise timed
by E administration represents an interesting, alternative
Serum E and inhibin B profiles from FD1 to FD3 in
strategy to assess ovarian follicular status. The observed
E -treated group markedly differed from each other.
improvement of hormonal-follicular correlations may be ex-
Whereas inhibin B levels dramatically increased in response
plained by a possible modification of early follicular growth
to FSH stimulation, E levels fell progressively from FD1 to
and steroidogenesis due to decreased premenstrual FSH se-
FD3 as a result of the interrupted exogenous contribution.
cretion. Additional investigation is needed to assess possible
Incidentally, the pace of inhibin B increase after E with-
consequences of luteal E administration on the early antral
drawal observed in the present study is remarkably similar to
follicle characteristics during the early follicular phase. More
Fanchin et al.
studies including a large number of cases are also required to
13. Groome NP, Illingworth PJ, O’Brien M, Pai R, Rodger FE, Mather JP,
et al. Measurement of dimeric inhibin B throughout the human men-
confirm the hypothesis that the magnitude of FSH and in-
strual cycle. J Clin Endocrinol Metab 1996;81:1401–5.
hibin B increases after E withdrawal can improve the pre-
14. Magoffin DA, Jakimiuk AJ. Inhibin A, inhibin B and activin A in the
follicular fluid of regularly cycling women. Hum Reprod 1997;12:
dictive value of hormonal measurements performed during
the early follicular phase for assessing women’s fertility
15. Baird DT, Fraser IS. Blood production and ovarian secretion rates of
estradiol-17 beta and estrone in women throughout the menstrual cycle.
J Clin Endocrinol Metab 1974;38:1009 –17.
16. Zeleznik AJ. Premature elevation of systemic estradiol reduces serum
References
levels of follicle-stimulating hormone and lengthens the follicular phaseof the menstrual cycle in rhesus monkeys. Endocrinology 1981;109:
1. Welt CK, Martin KA, Taylor AE, Lambert-Messerlian GM, Crowley
WF Jr, Smith JA, et al. Frequency modulation of follicle-stimulating
17. de Ziegler D, Jaaskelainen AS, Brioschi PA, Fanchin R, Bulletti C.
hormone (FSH) during the luteal-follicular transition: evidence for FSH
Synchronization of endogenous and exogenous FSH stimuli in con-
control of inhibin B in normal women. J Clin Endocrinol Metab
trolled ovarian hyperstimulation (COH). Hum Reprod 1998;13:561–4.
18. Thomas JD, Rubin DN. Tissue harmonic imaging: why does it work?
2. Mais V, Cetel NS, Muse KN, Quigley ME, Reid RL, Yen SS. Hor-
J Am Soc Echocardiogr 1998;11:803–8.
monal dynamics during luteal-follicular transition. J Clin Endocrinol
19. Hotelling H. The selection of variates for use in prediction with some
comments on the problem of nuisance parameters. Ann Math Stat
3. Gougeon A. Regulation of ovarian follicular development in primates:
facts and hypotheses. Endocr Rev 1996;17:121–55.
20. McNatty KP, Hillier SG, van den Boogaard AM, Trimbos-Kemper TC,
4. Reuss ML, Kline J, Santos R, Levin B, Timor-Tritsch I. Age and the
Reichert LE Jr, van Hall EV. Follicular development during the luteal
ovarian follicle pool assessed with transvaginal ultrasonography. Am J
phase of the human menstrual cycle. J Clin Endocrinol Metab 1983;
5. Roseff SJ, Bangah ML, Kettel LM, Vale W, Rivier J, Burger HG, et al.
21. le Nestour E, Marraoui J, Lahlou N, Roger M, de Ziegler D, Bouchard
Dynamic changes in circulating inhibin levels during the luteal-follic-
P. Role of estradiol in the rise in follicle-stimulating hormone levels
ular transition of the human menstrual cycle. J Clin Endocrinol Metab
during the luteal-follicular transition. J Clin Endocrinol Metab 1993;
6. Scott RT, Toner JP, Muasher SJ, Oehninger S, Robinson S, Rosenwaks
22. Clarke IJ. GnRH and ovarian hormone feedback. Oxf Rev Reprod Biol
Z. Follicle-stimulating hormone levels on cycle day 3 are predictive of
in vitro fertilization outcome. Fertil Steril 1989;51:651–4.
23. Mercer JE, Clements JA, Funder JW, Clarke IJ. Regulation of follicle-
7. Seifer DB, Lambert-Messerlian G, Hogan JW, Gardiner AC, Blazar
stimulating hormone beta and common alpha-subunit messenger ribo-
AS, Berk CA. Day 3 serum inhibin-B is predictive of assisted repro-
nucleic acid by gonadotropin-releasing hormone and estrogen in the
ductive technologies outcome. Fertil Steril 1997;67:110 –4.
sheep pituitary. Neuroendocrinology 1989;50:321–6.
8. Bancsi LF, Huijs AM, den Ouden CT, Broekmans FJ, Looman CW,
24. Eldar-Geva T, Robertson DM, Cahir N, Groome N, Gabbe MP, Ma-
Blankenstein MA, et al. Basal follicle-stimulating hormone levels are of
clachlan V, et al. Relationship between serum inhibin A and B and
limited value in predicting ongoing pregnancy rates after in vitro
ovarian follicle development after a daily fixed dose administration of
fertilization. Fertil Steril 2000;73:552–7.
recombinant follicle-stimulating hormone. J Clin Endocrinol Metab
9. van Montfrans JM, Hoek A, van Hooff MH, de Koning CH, Tonch N,
Lambalk CB. Predictive value of basal follicle-stimulating hormone
25. Erickson GF, Hsueh AJ, Quigley ME, Rebar RW, Yen SS. Functional
concentrations in a general subfertility population. Fertil Steril 2000;
studies of aromatase activity in human granulosa cells from normal and
polycystic ovaries. J Clin Endocrinol Metab 1979;49:514 –9.
10. Corson SL, Gutmann J, Batzer FR, Wallace H, Klein N, Soules MR.
26. Chikazawa K, Araki S, Tamada T. Morphological and endocrinological
Inhibin-B as a test of ovarian reserve for infertile women. Hum Reprod
studies on follicular development during the human menstrual cycle.
J Clin Endocrinol Metab 1986;62:305–13.
11. Hall JE, Welt CK, Cramer DW. Inhibin A and inhibin B reflect ovarian
27. Chang MY, Chiang CH, Hsieh TT, Soong YK, Hsu KH. Use of the
function in assisted reproduction but are less useful at predicting
antral follicle count to predict the outcome of assisted reproductive
outcome. Hum Reprod 1999;14:409 –15.
technologies. Fertil Steril 1998;69:505–10.
12. Klein NA, Battaglia DE, Fujimoto VY, Davis GS, Bremner WJ, Soules
28. Bancsi LF, Broekmans FJ, Eijkemans MJ, de Jong FH, Habbema JD, te
MR. Reproductive aging: accelerated ovarian follicular development
Velde ER. Predictors of poor ovarian response in in vitro fertilization:
associated with a monotropic follicle-stimulating hormone rise in nor-
a prospective study comparing basal markers of ovarian reserve. Fertil
mal older women. J Clin Endocrinol Metab 1996;81:1038 –45. FERTILITY & STERILITY
Sicurezza in casa Oltre ad alcune precauzioni ovvie, riguardo ad esempio i fili elettrici, vi sono alcune altre cose da controllare: -SEDIE RECLINABILI: spesso utilizzate come posti sotto cui nascondersi o schiacciare un pisolino. I gatti che restano impigliati nel meccanismo di apertura o chiusura possono venire seriamente feriti od uccisi. -LAVATRICI O ASCIUGABIANCHERIA: i piccoli spazi c
Work in Progress Published monthly by Michele Crawford Work in Progress is an electronic newsletter intended to assist individuals seeking optimum well-being. Mail to ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Work in Progress May 2006 Volume I Issue III Feature Article: Part One: Questioning the Treatment of Anxiety ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Please feel free to forward

 treated as in control groups (r ϭ Ϫ0.41, PϽ.0001 and r ϭ
Ϫ0.39, PϽ.0001, respectively). The mean length of the
preceding cycle was not altered by luteal E administration
Serum FSH (top panel), inhibin B (middle panel), and E
and remained similar in both groups (28.1 Ϯ 0.2 versus
(bottom panel) profiles during the first 3 days after E discon-
28.2 Ϯ 0.2 days, respectively). However, the subsequent
tinuation (FD1, FD2, and FD3) in the E -treated group. Both
menstrual cycles lasted slightly, but significantly, longer in
the progressive elevation in FSH and inhibin B levels, as wellas the decrease in E levels, from FD1 to FD3 were statisti-
the E -treated women (29.1 Ϯ 0.2 days) than in the controls
cally significant (open bars, PϽ.0001). Hormone levels on
FD3 were significantly different as compared to controls(CD3, closed bars, *PϽ.0001).
treated as in control groups (r ϭ Ϫ0.41, PϽ.0001 and r ϭ
Ϫ0.39, PϽ.0001, respectively). The mean length of the
preceding cycle was not altered by luteal E administration
Serum FSH (top panel), inhibin B (middle panel), and E
and remained similar in both groups (28.1 Ϯ 0.2 versus
(bottom panel) profiles during the first 3 days after E discon-
28.2 Ϯ 0.2 days, respectively). However, the subsequent
tinuation (FD1, FD2, and FD3) in the E -treated group. Both
menstrual cycles lasted slightly, but significantly, longer in
the progressive elevation in FSH and inhibin B levels, as wellas the decrease in E levels, from FD1 to FD3 were statisti-
the E -treated women (29.1 Ϯ 0.2 days) than in the controls
cally significant (open bars, PϽ.0001). Hormone levels on
FD3 were significantly different as compared to controls(CD3, closed bars, *PϽ.0001).