Long Term Care and the 2008 General Assembly
eral Assembly this year on SB 315; view of Medicaid home and communi-however, the House voted to adopt the
SB 42 continues the Select Joint Com-
this session. Although many issues adds additional responsibilities for
structuring, other important issues The Commission has been very in-
of the bills impacting long term care caid issues such as nursing home case
and senior housing and services that mix rates.
SB 302 covers a wide range of health SB 315 establishes a cap on Medicaid
beds in the state, but does not restrict
the addition of Medicare or private Health Facility Administrators
pay beds. Under the cap, Medicaid (nursing home administrators) Board
beds can be bought, sold, or moved; from 14 to 13 members by eliminating
however, there cannot be an increase the hospital administrator position.
in the total number of Medicaid beds The Board has had difficulty obtaining
reaches 95%. The current nursing The introduced version of the bill
home bed moratorium expires on called for reducing the board to 11
March 30, 2008. SB 315 is effective members.
HB 1172 also addresses a number of
rules to implement: (1) a screening tions. The bill requires, beginning July
1, 2008, and until June 30, 2009, that a
als seeking long term care services; (2)
NewsBriefs a process of prior approval for certain services agency obtain an employee's
individuals seeking admission to a limited criminal history not more than
H.O.P.E. March 2008 ~ Vol. 7, No. 3 5224 S. East Street Mission Inserts in this Issue Indianapolis, IN 46227 Phone: 317-472-0677 Fax: 317-472-0695
three business days after the date that an employee be-
quirements established in the regulations or the re-
gins to provide services. The bill also includes a provi-
quest for bids will receive a letter informing them of
sion that establishes criteria when a nursing home is
not required to provide CPR on a patient who is found
After the program begins, bidders that did not be-
dead and does not have a do not resuscitate order.
come contract suppliers generally cannot receive
Medicare payment for competitively bid items. How-
Medicare Announces Single Payment Amounts
ever, they may choose to continue in the Medicare
on Durable Medical
program as grandfathered suppliers for existing cus-
tomers if they supply certain rented items or oxygen
The Centers for Medicare & Medicaid Services (CMS)
or oxygen equipment to Medicare beneficiaries. Bid-
has completed the bid evaluation process and an-
ders that do not become contract suppliers for the first
nounced the single payment amounts for the first
round of bidding may bid in future rounds of compe-
round of the Medicare durable medical equipment,
prosthetics, orthotics, and supplies (DMEPOS) com-
petitive bidding program. The competitive bidding
The current Medicare fee schedule payment amounts
program will offer beneficiaries in the designated
will continue for beneficiaries who do not reside in
competitive bidding areas (CBAs) access to quality
the first round CBAs and for items that are not sub-
DMEPOS products and services with lower out-of-
ject to the Medicare DMEPOS Competitive Bidding
pocket costs. The only Indiana area affected is the
Program. The list of contract suppliers will be availa-
Cincinnati metro area in Indiana. The second round of
ble on the web page listed below when all contracts
bids will be starting soon and affect the Indianapolis
metro area and the Indiana portion of the Chicago met-
www.cms.hhs.gov/CompetitiveAcqforDMEPOS/
Under the program, the single payment amount will
ISDH Executive Board Rejects Aging-in-Place
become the Medicare allowed payment amount for the
competitive bidding items for beneficiaries who reside
The Indiana State Department of Health Executive
in the CBAs. Consistent with current CMS practice,
Board rejected a proposed rule that would have al-
Medicare will pay contract suppliers 80 percent of the
lowed residents of licensed residential care facilities
single payment amount for each competitively bid
that are a part of a comprehensive care facility to re-
item. The beneficiaries will be responsible for the re-
main in their unit when their needs exceeded those
maining 20 percent of the single payment amount.
As a result of the competitive bidding process, the amounts that Medicare will pay for the 10 product cat-
Quarterly Compliance Update: "Everyday
egories included in Round 1 of the DMEPOS Compet-
Compliance, Prevention & Response"
itive Bidding Program overall average 26% less than
Rebecca Bartle, R.N., Regulatory Affairs Director of-
Medicare's previous payment amounts. Savings for
HOPE, will lead this ½ Day Session on April 10th.
beneficiary out-of-pocket cost and Medicare range
This update will focus on Everyday Compliance, Preven-
from 14% on negative pressure wound therapy devices
tion & Response. The session will address specific inter-
and accessories up to as much as 43% on mail order
ventions for maintaining ongoing compliance, tactics for prevention of common citations, and manners of provid-
diabetic supplies. Beneficiaries in these CBAs will
er response when unfortunate events occur. The foun-
begin seeing savings on July 1, 2008. The single pay-
dation will be the Immediate Jeopardy citations since
ment amounts can be found on the CBIC website at:
September of 2007 as well as the most commonly cited
deficiencies and a look at the new ISDH CPR Guide-
CMS is notifying all bidders of their bid results. Win-
Attendees will leave this session with an acute aware-
ning bidders will be mailed contracts requiring their
ness of vulnerable areas of compliance but will also be
signatures. Qualifying bidders whose bids were not in
provided suggested manners of how to decrease the
the winning range may still receive a contract offer
facility's vulnerability through everyday practices and
from CMS if one of the winning bidders decides not to
become a contract supplier. Bidders whose bids were
The brochure with full details of the session is included
disqualified because their bids did not meet the re-
allowed in the current residential care rules. The
able (A/R) will be set up to recover the overpayment.
facility, the resident or their legal representative,
Following review of the RA, providers who disagree
and the resident’s physician would have had to
with any adjustment amounts may request an adminis-
agree and the facility would have had to ensure that
trative review by writing to the following address:
The Board expressed grave concerns with resident
safety, how these situations would be surveyed,
and the burdens and pressures on physicians under
such a system. Terry Whitson, Assistant Health
In the request explain why you disagree with the ad-
Commissioner, presented the Board with a sum-
justment amount and include copies of all pertinent
mary of comments received and issues raised at the
documentation. Detailed information about the admin-
public hearing, as well as comments provided to
istrative review process is available in the Indiana
him privately by individuals who did not want to
Health Coverage Programs (IHCP) Provider Manual.
oppose the rule publicly “because of perceived or
actual pressure to support the rule” from their or-
AARP Appoints New State Director
AARP Indiana has announced the appointment of June
Mass Adjustment of Medicare Part A
Lyle as state director. Lyle joined AARP in 2002 as
Crossover Claims
associate state director for public policy, and has
EDS will process a mass adjustment of Medicare
served as interim state director since September 2007.
Part A crossover claims with dates of service from
Prior to joining AARP, she was an attorney in private
October 1, 2001 through March 26, 2002. During
practice specializing in consumer, utility, and environ-
this time an emergency rule was in effect that
capped Medicaid reimbursement of crossover As state policy director, Lyle led AARP Indiana’s leg-
claims at the Medicaid allowable rate. The State
islative advocacy efforts, working with staff and vol-
was sued and prevented from implementing this
unteers to pass key legislation to improve the lives of
emergency rule as well as three others. On appeal,
Hoosiers 50+. Significant victories included laws on
the court found in favor of the State and sent the
prescription drug assistance, predatory mortgage lend-
case back to the trial court for a determination of
ing, home and community based health care services,
the amount the State was owed in restitution from
and security freeze/identity theft. Lyle directs a state
providers (See IFSSA v. Amhealth et al, 790
office staff of six people, who serve the interests of
more than 880,000 Hoosier members of AARP.
The lawsuit involved the nursing facility industry’s
challenge of four emergency rules that, in aggre-
gate, reduced Medicaid reimbursement. As a result
State Senator David Ford Dies
of a settlement with the plaintiffs, only Medicare
Four-term lawmaker David C. Ford (R-Hartford City)
Part A crossover claims will be adjusted and re-
has died. Ford died on March 5th at his home from
complications related to pancreatic cancer. Senator
The adjustments will begin appearing on the March
Ford was 59. He had been receiving hospice care and
18, 2008 remittance advice (RA). These claims
chemotherapy following hospitalization for what ap-
will have an ICN number starting with 56, which
peared to be flu-like symptoms in mid January, but
reflects a mass-adjusted claim. An accounts receiv-
had kept closely atop Statehouse events this legislative session via telephone and computer, Senate President Pro Tem David C. Long (R-Fort Wayne) said.
Billing Roundtable—April 22
Senator Ford was tapped in 2007 by Long to serve as
The next meeting of the HOPE/IAHSA Billing
Assistant Majority Floor Leader and chair of the Sen-
Roundtable has been set for April 22 from 10:00 a.m to noon at the IAHSA Office. All are welcome.
ate Committee on Economic Development and Tech-
To RSVP, contact Becky Carter at 317-733-2380 or
nology. In addition, Senator Ford was an active mem-
[email protected]
ber of the Judiciary, Tax and Fiscal Policy, and Educa-
HOPE BOARD OF DIRECTORS
Senate District 19, which Ford represented since 1994,
Blake Jackson, Chairman
includes all or parts of Adams, Allen, Blackford,
Grant and Wells counties. Senator Ford was a legisla-
Robert S. Decker, President
tor very interested in the needs and concerns of Indi-
Charles Bowman, Secretary Association Alerts Older Adults About Telemarketing Calls James Burkhart, Treasurer
Less-than-honest telemarketers are calling older adults
John W. Bartle
and persons with disabilities to sell their Medicare Ad-
vantage plans. With less than a week to go before the
March 31 enrollment deadline, "there will be multiple
Daniel Houston
opportunities for-less-than-honest individuals to offer
products and services that may not be Medicare ap-
proved, or individuals who will say they are Medicare
representatives,” according to Melissa Durr, Chief Ex-
Stuart B. Reed
ecutive Officer of the Indiana Association of Area
And the recipients of those calls are feeling the pres-sure. “This is not uncommon as we experienced simi-lar events last year,” Durr said. “In the past week, we
have been alerted to two cases of possible fraud in
Shred or tear into small pieces all mail solicita-
East Central Indiana.” Durr says that Medicare does
tions, bank records or any other discarded docu-
not make home visits or unsolicited phone calls. She
ments that contain identifying personal infor-
offered a variety of ways to protect, detect and report
Be aware of scams; if you’re told you just won a
“If someone contacts you and pressures you to buy,
If it sounds too good to be true, it probably is.
hang up your phone or close your door,” Durr said.
Questions about the viability of products or services
Durr recommends that if you suspect someone is try-
being offered for sale can be explored on your own.
ing to coerce or steal information, you should contact
Making sure you understand what you are buying,
your local Area Agency on Aging at 1-800-986-3505.
what is covered, what the cost of a product or service is, and how to cancel if you change your mind are all important questions the salesperson should be able to
2008 Wage Survey
answer. If they can’t, then you should probably de-
Durr offered additional tips that will help older adults
sisted living members. The survey is in an electronic
and persons with disabilities detect and prevent them-
format and members who choose to participate may
enter their own data, confidentially, at their conven-
ience. Each eligible member will receive a mailed noti-
Never sign anything you don’t understand; have an
fication of the process, log-in and password, and due
date. Because of federal law interpretation, a strict
participation deadline will be enforced. All participants
Stay socially active; isolation increases your risk
will receive a complimentary copy of the survey re-
sults. Our intent is to begin the participation process
Don’t give out your credit card or bank account
by early April. Watch for more information via mail and
numbers over the telephone or Internet unless you
MedPAC Considers Recommendations to
stration program using recovery audit contractors
(RACs) in California, Florida and New York in 2007. Change SNF Payment System
The Medicare Payment Advisory Commission
The RAC demonstration program, created by the
(MedPAC) issued its official March 2008 Medicare pay-
Medicare Prescription Drug, Improvement, and
ment policy report to Congress. MedPAC is an inde-
Modernization Act of 2003 (MMA), is designed to
pendent federal body that advises the U.S. Congress
find and correct improper Medicare payments paid
on issues affecting the Medicare program. MedPac is
to health care providers participating in fee-for-
recommending a revised system that would include
service Medicare. One of the areas that they have
improved payment components for "non therapy ancil-
been overturning is the 3-day qualifying stays for
laries" (mostly drugs), therapies, and an outlier pay-
Medicare payment in LTC, although 85% of the
collections have come from inpatient hospitals.
According to MedPAC, aggregate Medicare margins for
Approximately 96 percent of the improper payments
freestanding SNFs were above 10% for the last six
identified by the RACs in 2007 were overpayments
years. In 2006, the aggregate margin was 13.1%. Med-
collected from health care providers; the remaining
icare margins are estimated to reach 11.4% in 2008.
4 percent were underpayments repaid to health
The report suggests that SNF payments are more than
care providers. The demonstration program began
adequate to accommodate anticipated cost growth so
in California, Florida and New York in 2005 and
MedPAC is recommending that the Congress eliminate
expanded into Massachusetts, South Carolina, and
the update to payment rates for SNF services for fiscal
Arizona in 2007. The first three states are those
states with the largest number of Medicare claims.
MedPAC recommends that the Congress establish a Expansion into Indiana is slated for March of
quality incentive payment policy for SNFs in Medicare
2008.
to tie payments to patient outcomes. MedPAC identi-
fied the rates of community discharge and potentially
avoidable re-hospitalization as two important goals for
http://www.cms.hhs.gov/apps/media/press_releases
SNF patients in developing a quality incentive payment
policy. Using re-hospitalization rates as one perfor-
mance measure “represents a step toward having mul-
Home Health Spending Growth
tiple providers and settings mutually accountable for
The Centers for Medicare & Medicaid Services
lowering the number of potentially avoidable re-
(CMS) reports that home health care continues to
be the fastest-growing component of all personal
health care spending. Spending increased 9.9 per-
The 30-page SNF section can be accessed at:
cent in 2006. There are currently about 8,500 home
www.medpac.gov/chapters/Mar08_Ch02d.pdf.
health agencies in the United States and 7.6 million
people receive home health care each year.
CMS Clarifies Inpatient Part A Billing for No- Payment Claims
A new article from the Centers for Medicare and Medi-
Seniors & Federal Rebate Checks
caid Services (CMS) explains the circumstances under
Social Security beneficiaries who have not filed a
which a skilled nursing facility must submit a no-pay
federal tax return may be eligible for a federal tax
bill. Facilities must submit a bill for a beneficiary who
rebate check if they file a 2007 tax form. The pay-
has started a spell of illness under the Part A benefit for
ments of at least $300 for individuals or at least
every month of the related stay even though no bene-
$600 for married couples filing a joint tax return are
fits may be payable. In addition, facilities must submit
part of the economic stimulus package recently
no-payment bills for beneficiaries who have previously
passed by the Congress and signed into law by
received Medicare-covered skilled care and subse-
quently dropped to a non-covered level of service but
continue to reside in a Medicare-certified area of the
To qualify for a payment, a recipient’s 2007 Social
facility. The CMS article reflects no changes in existing
Security benefits combined with certain benefits
policy, but simply clarifies Chapter 6 of the Medicare
paid by the Department of Veterans Affairs and/or
Claims Processing Manual, SNF Inpatient Part A Bill-
other earned wages in that year must total at least
$3,000. Supplemental Security Income (SSI) does
http://www.cms.hhs.gov/MLNMattersArticles/download
not count as qualifying income for the stimulus pay-
ment. To receive the stimulus payment, recipients
must file a 2007 IRS Form 1040 (long form) or Form
CMS Program Identifies $371.5 Million in Im-
1040A (short form) by the filing deadline of April 15,
proper Medicare Payments in Three States
2008. All the recipient has to do is to file a 2007 tax return and the IRS will do the rest; they do not need
The Centers for Medicare & Medicaid Services (CMS)
to contact the IRS or fill out any other special forms.
has announced that $371.5 million in improper Medi-
The IRS will automatically calculate and send the
care payments has been collected from or repaid to
payment. This payment will not affect recipients’
health care providers and suppliers as part of a demon-
Social Security benefits and they will not have to
pay taxes on it next year. The IRS will begin mailing checks in
For assistance with appeals or with an application, check
early May. (WAHSA E-News, 3-6-08)
http://www.in.gov/idoi/shiip/ for information about health insur-
ance counseling in Indiana operated by the Department of Insur-
Study Suggests Medicaid-Sponsored Home Care Reduces Nursing Home Use
A recently released study of Medicaid-financed nursing home use
Private Medicare Plans’ Cost Questioned
over 18 months in 2001 and 2002 finds that in states such as Ore-
A New York Times article discusses a recent Congressional
gon that have extensive community based long-term care ser-
study which showed that private Medicare plans often cost ben-
vices, Medicaid-covered nursing home stays were shorter than
eficiaries more than the traditional government-run Medicare
the national average. The numbers suggest that where seniors
program. Although many private plans advertise extra benefits
have alternatives, their nursing home stays are more likely to be
and low costs the study showed that many people in private
for acute care following a hospitalization or for a shorter period at
plans face higher costs for home health care, nursing homes
and some hospital stays. About one-fifth of the 44 million Medi-
care beneficiaries – 9 million people – are in private plans,
The study reports that over half of enrollees beginning Medicaid-
financed nursing home spells were already residing in nursing
homes when Medicaid began financing part of their stay, with 29
The Government Accountability Office found that “48 percent of
percent obtaining coverage within six months, 5 percent between
Medicare Advantage beneficiaries were in plans that had an out-
six and 12 months, 7 percent between one and two years, and 9
of-pocket maximum.” T he limits typically ranged from $2,750 to
$4,600 a year and averaged about $3,500. But, the report said,
certain costs are not counted toward the out-of-pocket limits
The report confirms the continuing trend that most nursing home
established by some insurers. Thus, it said, among Medicare
residents are among the older old. The average of nursing home
plans with out-of-pocket limits, 29 percent exclude the cost of
resident who entered in 2002 was 76 years of age, with 32 per-
some cancer drugs, 23 percent exclude the cost of somemental
cent each being between the ages 75 and 84 and 85 and older.
health services and 21 percent exclude home health care ex-
Twenty percent were under age 65 and 16 percent between ages
http://aspe.hhs.gov/daltcp/reports/2008/mfNHserves.htm.
The accountability office found that private Medicare plans
“allocate about 87 percent of total revenue ($683 of $783 per
member per month) to medical expenses; approximately 9 per-
Some Medicare Beneficiaries Will Lose Part D Low
cent ($71) to nonmedical expenses, including administration,
Income Subsidy on April 1
marketing and sales; and approximately 4 percent ($30) to the
The Social Security Administration (SSA) has begun mailing "SSA
plans’ margin, sometimes called the plans’ profit.” (New York
Medicare Prescription Drug Assistance Notice of Termination"
letters to some beneficiaries who are currently receiving the low-
income subsidy (LIS) or "Extra Help." The letters are being sent
Study: Many Assisted-living Residents Under-Treated
to beneficiaries who did not provide SSA with information it re-
The majority of elderly people in assisted-living or residential
quested to determine their continuing eligibility for the LIS.
care facilities are not receiving all of the medications they need
for four common conditions, according to new study findings, a
Beneficiaries who do not act immediately upon receiving the letter
Reuters report stated. To investigate whether the elderly were
to request an appeal will no longer receive the LIS to pay for Part
facing problems due to a lack of needed medications, Dr. Philip
D premiums and cost-sharing effective April 1.
D. Sloane of the University of North Carolina in Chapel Hill re-
Beneficiaries who believe they are, or even might still be, eligible
viewed the medical records of 2,014 people 65 years of age or
for the LIS should contact SSA within 10 days of receiving their
older, Reuters reported. All study participants were residents of
letter to request an appeal. If they do so, they can continue receiv-
assisted-living or residential care facilities.
ing LIS until their appeal has been decided, regardless of whether
Sloane and his colleagues found that among people with a his-
it is decided in their favor. Call SSA at 1-800-SSA-1213 (1-800-
tory of heart attack, more than 60 percent were not taking aspi-
rin, and three-quarters were not receiving beta-blockers, com-
In addition to taking action to file an appeal, beneficiaries should
monly used to prevent repeat attacks. And, among people with
the bone-thinning disease osteoporosis more than 60 percent
They can reapply for LIS, even if they are not currently eligi-
were not taking calcium supplements, and more than half were
ble, if their circumstances change, making them eligible once
given no treatment at all, the Reuters report noted.
again. Beneficiaries who do not appeal must wait until April 1
More than 60 percent of subjects with congestive heart failure
to reapply. Otherwise, the applications will be considered
were not receiving an angiotensin-converting enzyme inhibitor --
duplicates and will not be processed by SSA. Applications
a common drug for this condition -- and more than one-third of
can be made by calling SSA at the above number or by filing
stroke patients were not given drugs to prevent future blood
on-line at http://www.ssa.gov/prescriptionhelp/.
clots. "The absence of potentially beneficial treatments in such
Their current drug plan will contact them to let them know
high percentages of residents of these facilities raises the spec-
how much their premium will be, starting April 1, without the
ter of an important quality problem in the care of older patients,"
Dr. Jerry H. Gurwitz told Reuters. (Advance for Health Infor-
They will have a 3-month special enrollment period, starting
April 1, to enroll in a different drug plan, if they choose not to remain in the one in which they are currently enrolled.
Diabetes Presents Growing Problem for
In an accompanying editorial, Mitchell J. Schwa-
Nursing Homes
ber, MD, MSc, and Yehuda Carmeli, MD, MPH, of
the Tel Aviv Medical Center, Israel, write: "The owned and operated
Diabetes is "enormously prevalent" in nursing homes.
solution is not to categorically deny antibiotics to providers of health care,
One out of every four residents over the age of 65 is
the severely demented elderly, or even to impose housing, and assistance
diagnosed with the disease, according to a new report
limits on their use or their spectrum as a matter of
from the Institute for the Future of Aging Services.
policy. We must, however, begin to consider every
Researchers analyzed the 2004 National Nursing decision to use antibiotics in this population as we
Home Survey, which includes data representing 1.32
would decisions regarding other treatment modali-
million nursing home residents over age 65. Among
ties, including resuscitation and major surgery. That
the findings: Non-white residents were twice as likely
is, we must ask whether the interests of the patient
to have diabetes as white residents; diabetic residents
are being served by using antibiotics. We must fur-
were younger than their non-diabetic counterparts; ther ask whether the use of antibiotics in each spe-
and the prevalence of diabetes in U.S. nursing homes
cific patient justifies the risk placed on others by
was higher in 2004 compared to previous years. IFAS
their use. (Nursing Homes eNewsletter)
is the applied research arm of the American Associa-
tion of Homes and Services for the Aging.
Medical Organizations Issue New Guide-
Those afflicted with the disease are at a greater risk
line on Drugs to Treat Dementia
for developing other conditions that can affect their
Further research urgently needed to address gaps in
quality of life and care needs, according to research-
knowledge about the clinical effectiveness of phar-
ers. Among the examples shown in the report, diabet-
macologic management of dementia. A committee
ics are more likely to take more medication and arrive
representing the American College of Physicians
at a nursing home with pre-existing circulatory prob-
(ACP) and the American Academy of Family Phy-
lems. Diabetics are also 56% more likely to have a
sicians (AAFP) found no convincing evidence
demonstrating that one therapeutic treatment for
The research was published in the February 2008 is-
dementia is more effective than another.
sue of Diabetes Care. To view the report, please go to
The committee reviewed dementia literature for
outcomes such as cognition, global function, behav-
ior/mood, and quality of life/activities of daily liv-
Study Raises Concern over Antibiotic Use in
ing. The committee found that high-quality scien-
Nursing Home Dementia Residents
tific evidence was limited and so developed cau-
Antibiotics appear to be frequently prescribed to indi-
tious recommendations on current pharmacologic
viduals with advanced dementia in nursing homes, treatment of dementia: especially in the two weeks before death, according to
Clinicians should base the decision to try thera-
a report in the February 25 issue of Archives of Inter-
py with the FDA approved drugs for dementia
nal Medicine. "This extensive use of antimicrobials
on an individualized assessment of the patient.
and pattern of antimicrobial management in advanced
Clinicians should base the choice of drugs on
dementia raises concerns not only with respect to in-
tolerability, adverse effect profile, ease of use,
dividual treatment burden near the end of life but also
with respect to the development and spread of antimi-
Further research is urgently needed to address
crobial resistance in the nursing home setting," the
gaps in knowledge about the clinical effective-
ness of pharmacologic management of demen-
"The proportion of residents taking antimicrobials was seven times greater in the last two weeks of life
Currently five drugs are approved by the FDA for
compared with six to eight weeks before death," the
dementia: four acetylcholinesterase inhibitors
authors write. Thirty of the 72 courses (41.7%) in the
[donepezil (Aricept), galantamine (Razadyne,
last two weeks of life were administered intravenous-
Reminyl, Nivalin), rivastigmine (Exelon), and ta-
ly rather than by mouth, a method that may be un-
crine], and one neuropeptide-modifying agent
comfortable for residents with advanced dementia. [memantine (Namenda)]. These drugs do not cure The results support "the development of programs dementia (there is no cure at this time) or repair and guidelines designed to reduce the use of antimi-
brain damage. They may improve symptoms or
crobial agents in advanced dementia."
“Doctors, patients, and family caregivers desperately want
• 46% for pain management
information on how to treat this disease,” said Amir Qaseem,
• 30% for pressure ulcers
MD, PhD, MHA, senior medical associate in the Clinical Pro-
• 40% for physical restraints
grams and Quality of Care Department at ACP. “It is disheart-
In addition to improving quality measures, nursing home
ening to find out that all we have to work with is these five
leadership collected data and evaluated their certified nursing
drugs, and the evidence on these is scant. Consider that in 50
assistant (CNA) turnover with tools and education provided
years, one in 45 Americans will suffer from Alzheimer’s dis-
by the QIO. The leadership reviewed human resource poli-
ease. This is a huge problem.” (Nursing Homes/LTCM
cies, hiring practices, orientation practices, and mentoring
opportunities. Through this evaluation and organizational
changes, the CNA turnover made a 13% relative improve-
Medwatch - Fentanyl Transdermal Patches: Recall
ment from baseline in 2006 to re-measurement in 2007.
Due To Gel Leak That May Lead To Respiratory Depression and Overdose Few Studies Explore MRSA Prevention Strategies
Actavis Inc. announced a nationwide recall of certain lots of
for Nursing Homes
Fentanyl transdermal system CII Patches sold in the United
Methicillin-resistant Staphylococcus aureus (MRSA) is mak-
States and labeled with an Abrika or Actavis label. The prod-
ing news as a dangerous, sometimes fatal disease, for hospi-
uct may have a fold-over defect which can cause the patch to
tal patients, and in recent cases, students. MRSA is also a
leak and expose patients or caregivers directly to the fentanyl
major source of illness acquired in nursing homes, yet few
gel. Exposure to fentanyl gel may lead to serious adverse studies have looked at how to prevent its spread among elder-
events, including respiratory depression and possible over-
ly residents, according to a new review. Close living proxim-
dose, which may be fatal. The lots covered by this recall in-
ity, multiple medications, pressure sores, and catheters all
clude doses of 25, 50, 75, and 100 mcg/hr and are listed in the
make nursing homes ideal for breeding and spreading
firm's press release. See the complete MedWatch 2008 safety
MRSA; however, nursing homes appear to have been
summary, including a link to the firm's press release, at: shortchanged in the medical literature on prevention, despite
www.fda.gov/medwatch/safety/2008/safety08.htm#Fentanyl
studies repeatedly reporting that residents are at higher risk.
Significant Improvement Shown in Quality
"Much of the research effort around MRSA to date has fo-
Improvement Goals
cused primarily on hospitals," said Carmel Hughes, lead re-
view author. Hughes, a professor of primary care pharmacy
In an effort to improve the quality of care for Indiana nursing
at Queen's University Belfast in Northern Ireland, and col-
home residents, Health Care Excel (HCE), the Indiana Medi-
leagues searched for randomized and controlled clinical trials
care Quality Improvement Organization (QIO), provided edu-
that focused on infection control interventions in nursing
cation and technical assistance to 84 nursing homes as part of
the national Nursing Home Quality Initiative (NHQI).
Hughes said introducing effective interventions in hospitals
Data were collected during an 18-month period, from January
might be easier because hospitals have isolation facilities and
2006 through June 2007. By directly involving nursing home
greater access to infection control expertise. Infection control
staff in the redesign of care delivery through a person-centered
training is not routinely available in nursing homes, she add-
approach, and provision of data to monitor progress over time,
ed. "It is likely that an intervention for MRSA in nursing
the 84 participating nursing homes were able to make signifi-
homes will consist of screening recently admitted residents to
the nursing homes, hand washing, and high standards of
cleaning and decontamination," Hughes said. "It will be im-
Goal 1: Decrease the percent of residents who experience portant for some staff members to make infection control a
priority and that this is communicated to all other staff." Rig-
Goal 2: Decrease the percent of residents who have pressure
orous testing in the nursing home environment and detailed
notes about such interventions will help ensure that they are
Goal 3: Decrease the percent of residents who were physically
The review appears in the 2008 Issue 1 of The Cochrane Li-
As a result of working closely with nursing home providers
brary, a publication of The Cochrane Collaboration, an inter-
through on-site visits, conducting regional workshops and tel-
national organization that evaluates medical research( Nurs-
econferences, and bringing nationally known, long term care
experts to statewide meetings, nursing homes collectively pro-duced the following Relative Improvement Rates.
CDC Website is a One-Stop Site for Flu Information:
http://www.cdc.gov/flu/ Everything you need to know is in one place!
Immediate Jeopardy Citations Released
meet the needs of its residents, in that protimes
During a March 14th meeting with the long term care as-
and International Normalized Ratios (PT/INR)
sociations, the Indiana State Department of Health re-
(measurements of clotting times) for residents
leased narrative summaries for six Immediate Jeopardy
on Coumadin (blood thinner) were not obtained
citations which occurred at five facilities during the month
according to physician’s orders for 3 of 3 resi-
dents on Coumadin in the total sample of 13,
and 2 of 3 residents on Coumadin in the supple-
mental sample of 15. This resulted in clotting
The facility failed to ensure the heating ventilation
times being too long with potential for serious
equipment was in proper working order, in that
injury, and 1 resident actively bleeding and be-
when a resident complained of the lack of heat in
ing hospitalized and transfused with fresh fro-
his room, the facility staff provided the use of an
electric space heater rather than repair the heat-
ing unit. The use of the electric space heater pre-
sented the potential to cause resident burn/injury
The facility failed to initiate cardiopulmonary
resuscitation (CPR) for a resident with a signed
advance directive that indicated the resident chose to have efforts made to prolong his life.
The facility failed to provide care and services for
This affected 1 of 1 resident reviewed who had
2 of 7 sampled residents who had significant de-
expired at the facility in the sample of 11. The
cline in their condition when the resident displayed
facility also failed to ensure 5 of 67 residents
vomiting, followed by increased respiratory rate
currently residing in the facility had physician’s
and decreased responsiveness, care and treat-
orders which matched their chosen advance
ment were not provided in a timely manner, result-
ing in the resident’s delayed transfer to the hospi-
tal and death. And, when another resident dis-
Bed Rail Entrapment (From the ISDH
played increased unrelieved pain in the leg after a
Newsletter)
fall and the facility received an X-ray report show-
There recently was a tragic death of a resident in an
ing a fracture, the resident was not assessed and
Indiana nursing home involving bed rail entrapment.
Facilities need to be checking the bed rails being used
for residents. Please be especially observant of the
rails on any of the beds in the facility that have more
The facility failed to follow their established poli-
than 4 3/4 inches between the bars. Please review the
cies and procedures for Wander Guard placement
guidance provided from CMS on F323 and from the
which resulted in an elopement from the secured
FDA website for information about entrapment in hos-
dementia unit by a cognitively impaired resident
with a known history of elopement risks. This
elopement occurred as a result of the nursing staff’s failure to replace a Wander Guard bracelet. The resident was returned to the facility by the police.
The facility failed to provide adequate monitoring for residents on Coumadin (blood thinner), in that they failed to monitor protimes and international
normalized ratios (PT/INR) (measurement of clot-
ting times), for 3 of 3 sampled residents on
Coumadin, in the sample of 13, and 2 of 3 supple-
Regardless of the purpose for use, bed rails (also re-
mental sample residents on Coumadin in the sup-
ferred to as "side rails," "bed side rails," and "safety
plemental sample of 15, as ordered by the physi-
rails") and other bed accessories (e.g., transfer bar,
cian, and ensure abnormal PT/INRs were reported
bed enclosures), while assisting with transfer and posi-
to the physician and acted upon, This resulted in
tioning, can increase resident safety risk. Bed rails
clotting times being too long with potential for seri-
include rails of various sizes (e.g., full length rails, half
ous injury, and 1 of the sampled residents on
rails, quarter rails) that may be positioned in various
Coumadin actively bleeding and being hospital-
locations on the bed. In 1995, the FDA issued a Safety
ized and transfused with fresh frozen plasma to
Alert entitled "Entrapment Hazards with Hospital Bed
Residents most at risk for entrapment are those who
The facility failed to obtain laboratory services to
are frail or elderly or those who have conditions such
as agitation, delirium, confusion, pain, uncontrolled body move-
120 mm (4 3/4 inches), representing head breadth.
ment, hypoxia, fecal impaction, acute urinary retention, etc. that
ISDH Addresses QMA Inservice Verification
may cause them to move about the bed or try to exit from the bed.
All qualified medication aides (QMAs) must submit the "Qualified
The timeliness of toileting, appropriateness of positioning, and
Medication Aide Record of Annual Inservice Training" form as
other care-related activities can contribute to the risk of entrap-
part of their certification renewal process. Each form is reviewed
for both the required inservice education topics and mandatory
six hours. During the review process additional information may
Entrapment may occur when a resident is caught between the
be needed to clarify the inservice information.
mattress and bed rail or in the bed rail itself. Technical issues,
The ISDH has discovered a few cases where the information
such as the proper sizing of mattresses, fit and integrity of bed
submitted on the inservice form was falsified. This includes situ-
rails or other design elements (e.g., wide spaces between bars in
ations such as the QMA did not attend the inservice or the in-
the bed rails) can also affect the risk of resident entrapment.
structor's signature was not the instructor's actual signature.
US Dept. of Health and Human Services, Food and Drug Admin-
istration (August 23 1995). FDA Safety Alert: Entrapment Haz-
If there is some question about the information on the form, the
ISDH will initiate an investigation. The ISDH takes falsification of
records very seriously and will take enforcement action if records
US Dept. of Health and Human Services, Food and Drug Admin-
are falsified. If falsification of found, the QMA's certification will
istration, Hospital Bed Safety Workgroup. (April 2003), Clinical
be revoked. If the QMA is also a CNA that certification will also
Guidance for the Assessment and Implementation of Bed Rails In
Hospitals, Long Term Care Facilities, and Home Care Settings.
Retrieved November 11, 2005 from http://www.fda.gov/cdrh/beds/.
State Releases New Guidance on CPR
For some time the Indiana Department of Health has been
Dimensional Limits for Identified Entrapment Zones 1-4
pressed to review the practice of citing facilities, often with Imme-
[The following is an excerpt from the Hospital Bed System Dimen-
diate Jeopardy, for failing to perform CPR on an individual who
sional and Assessment Guidance to Reduce Entrapment - Guid-
has expired and for whom CPR would be futile and inappropri-
ance for Industry and FDA Staff (Issued March 10, 2006)]
ate. There may be times when a resident expires unexpectedly
during his or her sleep and is not discovered until a period of
FDA is recommending dimensional limits for zones 1 through 4 at
time after death. Cardio-Pulmonary Resuscitation is an aggres-
this time because we believe the majority of the entrapments re-
sive medical procedure that should not be employed when there
ported to FDA have occurred in these zones. We based these
is no possibility of recovering a life. Under this guidance, the fa-
recommended limits upon the body parts entrapped in these indi-
cility must develop a policy, which is approved by the medical
vidual zones identified through adverse event reports and entrap-
director, to guide staff on when an exception to CPR would be
ment scenarios described in the reports. A summary table (Table
3) of the hospital bed dimensional limit recommendations appears
If the facility does not have a policy and the resident does not
have a DNR order, then the surveyor will expect CPR to be per-
The Hospital Bed Safety Workgroup developed and validated test
formed until CPR is deemed not necessary by the physician.
methods to measure and assess gaps or openings in zones 1-4 of
hospital bed systems, reprinted in Appendix F. As a member of
Subsequently, ISDH was asked to clarify whether this policy ap-
the Hospital Bed Safety Workgroup, the Federal Drug Administra-
plies to licensed residential care facilities.
tion (FDA) participated in the development and validation of these
test methods. FDA recommends these test methods as an ac-
The CPR policy is based on an appropriate facility policy for im-
ceptable approach for assessing hospital bed gap sizes in accord-
plementing CPR. The basis of a facility policy would be an appro-
ance with the dimensional limitations described below. The test
priate assessment of the resident. A physician or nursing assess-
methods and tool used to conduct these tests are available
ment would be expected as part of the facility policy criteria in
through the Hospital Bed Safety Workgroup (see Appendix B). If
an alternate approach is used to assess gap sizes, FDA recom-
mends that the dimensional limits used in any alternative ap-
The concern of ISDH was whether the residential care facility
proach be at least as stringent as the ones described below.
would have the necessary physician or nursing staff present at
the facility needed to perform the assessment. Residential care
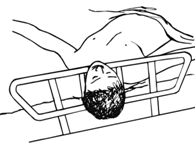
Zone 1 is any open space within the perimeter of the rail. Open-
facilities are not necessarily required to have nursing staff on site
ings in the rail should be small enough to prevent the head from
at all times [410 IAC 16.2-5-1.4(b)]. If the residential care facility
entering. A loosened bar or rail can change the size of the space.
does not have nursing staff on site, there will not be a qualified
The Hospital Bed Safety Workgroup and International Electrotech-
individual to assess the resident pursuant to the policy. In that
nical Commission (IEC) recommend that the space be less than
case the facility is likely obligated to initiate CPR unless there is a do not resuscitate order. If there is a nurse on site who can make the necessary assessment and the facility has a CPR poli-
Becky Bartle’s next Quarterly Compliance Update is on
cy, the ISDH CPR policy would be applicable to residential care
Look for the brochure included with this newsletter.
Sommer Barnard Attorneys Advantage Billing & Commercial Food Systems Consultants, Inc. Century Marble Co., inc. Bradley & Associates, CPA Gordon Food Service Messer Construction Crowe Chizek & Company Silverchair Learning Systems Harmon & Hanlon, LTD Meyer Najem Construction SafeCare Electronics Health Management Advisors Advantage Billing & Consultants, Inc. PMC Healthcare P/R Mortgage & Investment Corp. Consultants, Inc. AmeriCare Consulting Group Senior Living Investment Brokerage, Inc. Thomas Healthcare Courtney & Associates Consulting, P.C. Neace Lukens Networx gp Plante & Moran Clinical Group Harrison & Moberly Insight Drug Abuse Testing Krieg DeVault LLP Conor-Patrick Insurance Services Healthcare Services Group Cornerstone Pharmacy McKesson Corporation Diamond Insurance New Day Pharmacy Corporation Midwest Insurance Group, Inc. PRN Pharmaceutical Services Med-Mizer William Brothers LTC Pharmacy Spiris, Inc. Medline Healthcare Company Citizen’s Mechanical Services Healthcare Therapy Services Professional Medical & Surgical Supply, Inc. PeopleFirst Rehabilitation Advanced Medical Supply Preferred Podiatry Group TwinMed, LLC All Med Medical Supply Samaritan Alliance Kreg Therapeutics Direct Supply, Inc. Select Rehabilitation, Inc. Medical Supplies/Billing Services McKesson Corporation First Choice Medical Supply
CLOZARIL: Starting a Patient 1. Call the CLOZARIL National Registry (CNR) to obtain a rechallenge number and to confirm that you and your pharmacy are registered. 2 . Obtain a baseline WBC with ANC from patient. If within normal limits, WBC ≥ 3500/ mm3, ANC ≥ 2000/ mm3, prescribe CLOZARIL tablets. 3. Submit WBC and ANC information to the registered pharmacy. 4. Please be pre
 Long Term Care and the 2008 General Assembly
eral Assembly this year on SB 315; view of Medicaid home and communi-however, the House voted to adopt the
SB 42 continues the Select Joint Com-
Long Term Care and the 2008 General Assembly
eral Assembly this year on SB 315; view of Medicaid home and communi-however, the House voted to adopt the
SB 42 continues the Select Joint Com- MedPAC Considers Recommendations to
MedPAC Considers Recommendations to  pay taxes on it next year. The IRS will begin mailing checks in
For assistance with appeals or with an application, check
early May. (WAHSA E-News, 3-6-08)
http://www.in.gov/idoi/shiip/ for information about health insur-
ance counseling in Indiana operated by the Department of Insur-
Study Suggests Medicaid-Sponsored Home Care
pay taxes on it next year. The IRS will begin mailing checks in
For assistance with appeals or with an application, check
early May. (WAHSA E-News, 3-6-08)
http://www.in.gov/idoi/shiip/ for information about health insur-
ance counseling in Indiana operated by the Department of Insur-
Study Suggests Medicaid-Sponsored Home Care  Diabetes Presents Growing Problem for
Diabetes Presents Growing Problem for  “Doctors, patients, and family caregivers desperately want
• 46% for pain management
“Doctors, patients, and family caregivers desperately want
• 46% for pain management 
 Immediate Jeopardy Citations Released
Immediate Jeopardy Citations Released  as agitation, delirium, confusion, pain, uncontrolled body move-
120 mm (4 3/4 inches), representing head breadth.
ment, hypoxia, fecal impaction, acute urinary retention, etc. that
ISDH Addresses QMA Inservice Verification
as agitation, delirium, confusion, pain, uncontrolled body move-
120 mm (4 3/4 inches), representing head breadth.
ment, hypoxia, fecal impaction, acute urinary retention, etc. that
ISDH Addresses QMA Inservice Verification  Sommer Barnard Attorneys
Sommer Barnard Attorneys  Conor-Patrick Insurance Services
Conor-Patrick Insurance Services