fig. 2 Squamous cell carcinoma of the left sub- auricular region. (a) Planning of the surgical margins; (b) partial direct closure of the distal extremity of the primary defect and incision of the opposing rotation flap; (c) tip of the rotation flap moved into the defect; (d) final appearance of the repair.
it has been assessed that the primary defect is not suitable
for complete side-to-side closure. It allows the recovery of
1 Mellette JR Jr. Facial reconstruction in the elderly. J Geriatr
free tissue as a rotation flap that would otherwise be dis-
Dermatol 1995; 3: 286–297.
carded as a dog-ear. Cosmetic and functional results have
2 Schmidt DKT, Mellette JR Jr. The dog-ear rotation flap for the
been highly satisfactory in all cases, as an excellent match
repair of large surgical defects on the head and neck. Dermatol
in skin colour and texture has always been maintained
Surg 2001; 27: 908–910.
This surgical procedure has produced minimal tensionacross the wound edges, with less scarring and little or no
distortion of adjacent anatomic structures. Though
mainly applied on the head, the flap has been successfullyperformed on any anatomic location. According to our
Therapeutic use of mistletoe
experience the comet flap can be a valuable surgical
for CD30+ cutaneous
option for closure of round to oval defects of any size in
lymphoproliferative disorder/
dermatological surgery reconstruction. lymphomatoid papulosis Dermatology Unit, ‘A. Murri’ Hospital Via dei Colli,52 60035 Jesi – AN, Italy, *Corresponding author,
Lymphomatoid papulosis (LyP) is defined in the WHO
tel. +39 0731534145; fax +39 0731534035;
classification as a CD30+ cutaneous lymphoproliferative
lymphoma (CLPD) and is regarded as a condition of
JEADV 2007, 21, 536– 578 2006 European Academy of Dermatology and Venereology
uncertain malignant potential.1 The incidence of LyP in
ALCL were effective. As seen in our patient, relapse of LyP
children is relatively low compared to that in adults.2 It
skin lesions is common. The good response of the second
is correlated with malignant lymphomas in 5 to 20% of
relapse of LyP to MT is suggestive but could also represent
adult LyP patients.3,4,5 In children, an increased risk for the
the natural history of LyP. After the third cutaneous relapse
development of malignant lymphoma is observed.6,7 The
of LyP and the subsequent positive response to MT the
clinical course is often chronic. The most common treatments
therapeutic efficacy of MT in this patient seems evident.
for LyP are topical steroids, antibiotics, phototherapy and
In particular, the temporal association between the MT
low-dose methotrexate, all of which are associated with
injections and the response and the typical local reaction
an excellent prognosis, even for patients with anaplastic
to MT are indications of a connection in this case. MT is
widely used in Europe as an additional therapy for cancer
An 8-year-old boy presented with reddish nodules
patients10 and no adverse or long-term effects have been
(maximum of 7 cm in diameter) on his right forearm and
left leg. Immunohistochemical analysis identified a CD30+,large, T-cell type non-Hodgkin’s lymphoma of the skin.
G Seifert,*† C Tautz,‡ K Seeger,† G Henze,† A Laengler‡
Topical steroids were effective but 6 months later the patient
†Charité – Universitätsmedizin Berlin, Otto-Heubner-Centre for
developed axillary lymph-node swelling. Classifying the
Paediatric and Adolescent Medicine (OHC), Klinik für Pädiatrie
condition now as ALCL without signs of systemic involve-
mit Schwerpunkt Onkologie/Hämatologie, Mittelallee 6a,
ment, combination chemotherapy according to the German
Augustenburger Platz 1, 13353 Berlin, ‡Department of
ALCL trial (high-risk group)9 was given for 6 months. All
Paediatrics, Gemeinschaftskrankenhaus Herdecke, Germany,
nodules (cutaneous and lymphoid/axilla) resolved within
*Corresponding author, tel. +49 30 450 666087;
a few weeks. However, 2 months after cessation of chem-
fax +49 30 450 566946; E-mail: [email protected]
otherapy a new skin nodule on the left forearm appeared. No specific therapy was given. In the following 2 monthsthe patient developed two further solid and painful skin
lesions. We started subcutaneous therapy with Abnoba
1 Willemze R, Meijer CJ. Primary cutaneous CD30-positive
Viscum fraxini® (ABNOBA Heilmittel GmbH, Pforzheim,
lymphoproliferative disorders. Hematol Oncol Clin North Am
Germany) a mistletoe extract (MT). A schedule of two
2003; 17: 1319–1332.
injections per week was initiated, starting with a dose of
2 Zirbel GM, Gellis SE, Kadin ME, Esterly NB. Lymphomatoid
20 mg in the first week, but choosing the subsequent exact
papulosis in children. J Am Acad Dermatol 1995; 33: 741–
dosages with a view to obtaining a marked local reaction
with mild fever and local swelling. MT was injected sub-
3 Wang HH, Myers T, Lach LJ, Hsieh CC, Kadin ME.
cutaneously close to the largest lesions. One day following
Increased risk of lymphoid and nonlymphoid malignancies
the first local injection of MT, a fever of 38 °C was observed,
in patients with lymphomatoid papulosis. Cancer 1999; 86:
plus local swelling and redness. The skin nodules started to
decrease and MT injections into all lesions were continued.
4 Beljaards RC, Willemze R. The prognosis of patients with
Within the following 2 weeks the skin lesions resolved. After
lymphomatoid papulosis associated with malignant
regression of all local symptoms, subcutaneous MT therapy
lymphomas. Br J Dermatol 1992; 126: 596–602.
with two injections of 0.2 mg per week was continued.
5 Fink-Puches R, Chott A, Ardigo M et al. The spectrum of
Two months later, the patient developed two new small
cutaneous lymphomas in patients less than 20 years of age. Pediatr Dermatol 2004; 21: 525–533.
nodules that responded within a few days to an increased
6 Nijsten T, Curiel-Lewandrowski C, Kadin ME.
dose of MT. During 2 years of follow-up therapy with MT
Lymphomatoid papulosis in children: a retrospective cohort
the boy remained without clinical signs of either LvP or
study of 35 cases. Arch Dermatol 2004; 140: 306–312.
ALCL. After 2 years, MT therapy was stopped. Unfortu-
7 Kadin ME, Carpenter C. Systemic and primary cutaneous
nately, 3 weeks after cessation of MT therapy the patient
anaplastic large cell lymphomas. Semin Hematol 2003; 40:
developed a relapse, displaying generalized reactivation of
the cutaneous LyP with typical nodules (maximum 1 cm
8 Reiter A, Schrappe M, Tiemann M et al. Successful treatment
in diameter) all over the body. Subcutaneous and local
strategy for Ki-1 anaplastic large-cell lymphoma of
intralesional MT therapy was resumed and the cutaneous
childhood: a prospective analysis of 62 patients enrolled in
LyP regressed completely within 2 weeks without additional
three consecutive Berlin-Frankfurt-Munster group studies.
J Clin Oncol 1994; 12: 899–908.
It is known that CD30+ CLPDs have an overall excellent
9 Kienle GS, Berrino F, Bussing A, Portalupi E, Rosenzweig S,
outcome.8 In our patient, initial topical MT therapy of LyP
Kiene H. Mistletoe in cancer – a systematic review on
and subsequent systemic combination chemotherapy of
controlled clinical trials. Eur J Med Res 2003; 8: 109–119. JEADV 2007, 21, 536– 578 2006 European Academy of Dermatology and Venereology
10 Augustin M, Bock PR, Hanisch J, Karasmann M, Schneider
B. Safety and efficacy of the long-term adjuvant treatment of primary intermediate- to high-risk malignant melanoma (UICC/AJCC stage II and III) with a standardized fermented European mistletoe (Viscum album L.) extract. Results from a multicenter, comparative, epidemiological cohort study in Germany and Switzerland. Arzneimittelforschung 2005; 55: 38–49. Scleredema adultorum associated with type 2 diabetes mellitus: a fig. 1 Induration of the skin of the face, neck, trunk and upper arms. report of three cases
Scleredema adultorum is a rare disease of unknownaetiology that can be associated with type 2 diabetesmellitus. Therapeutic options are limited, but successfultreatment with ultraviolet A1 (UVA-1) or antibiotics hasbeen described.
Here, we report three cases of type 2 diabetes-associated
The first patient, a 55-year-old Caucasian man presented
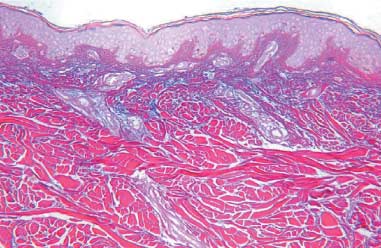
with a 2-year history of thickening of the skin resultingin reduced mobility of the neck and shoulders, withoutsystemic manifestations. He was treated with systemicpsoralen and UVA (PUVA) followed by UVA-1 therapy,without success, 2 years ago. fig. 2 Histopathology: thickening of collagen bundles with interposed
The patient was again treated with UVA-1 (90 J/cm2) five
mucin (magnification ×100; staining with colloidal iron).
times per week and by physiotherapy, resulting in softeningof the skin and enhanced mobility within 4 weeks ofinitiation of treatment.
Histopathology was typical for scleredema, with mucin
The second patient, a 57-year-old Caucasian woman
interposed between thickened collagen bundles, which
had a 20-year history of thickening of the skin of the nape
was shown by colloidal iron staining (fig. 2).4,8,9 The same
of the neck, trunk, upper arms, back and dorsal thighs.
histological findings were detected in specimens from the
Mobility of the neck and shoulders was decreased. She
other two patients. Because of the short history of her dis-
was treated with UVA-1 several times without success.
ease the patient was treated with intravenous penicillin
The patient was retreated with UVA-1 50 J/cm2 on the
(3 × 5 million U/day) for 2 weeks despite the absence of
whole body and additional 40 J/cm2 on the nape of the
clinical signs of infection. Two months later the patient
neck and back. She suffered from sinusitis which was
presented with remarkable improvement. Softening of
treated with intravenous clindamycin (3 × 600 mg/day)
the skin as well as increased mobility (especially of facial
for 2 weeks because she was allergic to penicillin. The
muscles and arms) had taken place; therefore, a scheduled
patient responded slightly with decrease of skin rigidity
within 4 weeks after initiation of treatment.
Scleredema adultorum is a rare disease of unknown
The third patient, a 58-year-old Arab woman presented
aetiology, which was first described by Buschke in 1900.1
with thickening of the skin resulting in reduced mobility
It is characterized by non-pitting induration of the skin,
of her mimic muscles, neck and shoulders starting only
with no defined boundary between normal and diseased
about 2 months prior to admission to our clinic. Facial
skin and symmetric induration of the face, neck and nape.
involvement resulted in a mask-like expression of the face
This can spread to the upper trunk and upper arms, or,
(fig. 1). Mobility of arms and neck was also significantly
more rarely, to other body regions. Moreover, multiple
reduced. The patient denied any previous infection.
organs can be involved with respective complications. Skin
, 536– 578 2006 European Academy of Der
file:///C|/Documents%20and%20Settings/Administrator/Desktop/UILFPL%202.0/contratti/CCNLsprivInt2bien.htm COMUNICATO UNITARIO Il 4 luglio si è svolto il previsto incontro richiesto dalle OO.SS. Sindacali CGIL CISL UIL del Comparto Sanità con l’ARIS l’AIOP e la Fondazione Don Gnocchi – onlus – sulla corretta applicazione di alcune norme contrattuali riferite soprattutto al seco
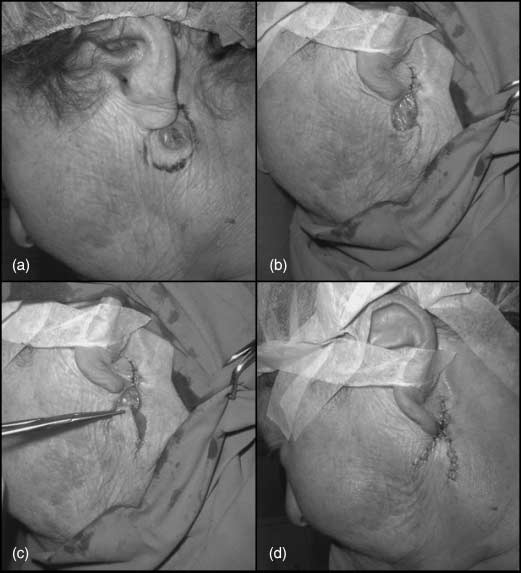 fig. 2 Squamous cell carcinoma of the left sub-
fig. 2 Squamous cell carcinoma of the left sub-
 10 Augustin M, Bock PR, Hanisch J, Karasmann M, Schneider
B. Safety and efficacy of the long-term adjuvant treatment
10 Augustin M, Bock PR, Hanisch J, Karasmann M, Schneider
B. Safety and efficacy of the long-term adjuvant treatment