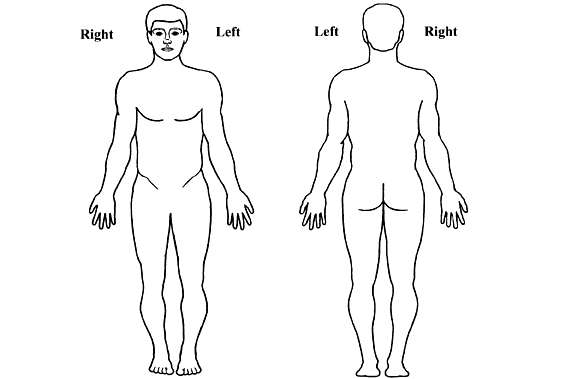
NEW PATIENT PAIN/SPINE INTAKE FORM Referring Physician: Date of Birth: Primary Care Physician: Are you right or left handed? What is the main problem that brings you here today (you may check more than one)? Which area of pain is the worst? On the drawings below, please shade the area where you currently experience pain. PAIN HISTORY When did the pain start (month/day/year)? How did the pain start? Have you ever been involved in any legal proceedings related to this health matter?
Do you have any other legal issues? Have you had any previous major pain issues? What is the quality of your pain/symptoms? Since the pain/condition began has it:
On a scale from 0 to 10 (where 10 is the worst possible pain) how would you describe the intensity of your pain:
Average level of pain over the last month: Current level of pain:
At your worst, what is your pain level: At your best your pain is: Do you have any of the following associated symptoms?
RELIEVING AND AGGRAVATING FACTORS Check off the following boxes depending on how the position affects your pain: DecreaseIncrease No Change OTHER THERAPIES FOR PAIN Please check all of the treatment you have tried for this pain condition and indicate whether the treatment provided you with any relief. Treatment No Relief Moderate Relief Excellent Relief MEDICATIONS YOU HAVE TAKEN IN THE PAST FOR PAIN OR MOOD Using the list below, please indicate the prescription medication(s) that you have tried in the past. If you have not taken these medications, you can skip this section. Opioids Antiinflammatories (NSAIDs) Muscle Relaxants Antidepressants Antianxiety Agents Other Agents ALLERGIES Are you allergic to latex? Are you allergic to IV Contrast? Do you have any other allergies? MEDICAL HISTORY Current/Past medical problems:
Other Conditions: 1. Prior spine surgeries: Prior major surgerie not spine related: 1. All Current Medications & Supplements/Herbs (name, dose, frequency) 1. Do any of your family members (blood relatives) have any of these diseases?
Marital status: Have you experienced significant stress in the past year? What is your living situation?(family, friends alone, etc.) If you have children, what are their ages? What is your current work status? What is the highest grade you completed or degree you received? Tobacco Use Alcohol Use Other Drug Use Caffeinated Drinks REVIEW OF SYMPTOMS (Please mark all of the following that apply to you)
chart June 2012.qxp:Layout 1 4/11/11 14:43 Page 2 PRECAUTIONS Doxycycline can rarely cause photosensitivity in patients taking it at doses for malaria prophylaxis, however it is normal y mild and can be minimised by using a high factor sunscreen. Doxycycline should be avoided in patients with porphyria and Mefloquine should be avoided in patients with hypersensitivity to quinine and in pat
Elfenau Park Jahresprogramm 2014 Jan 1.Konzert März 8.Konzert Do 02.01. / 10.30 Uhr und 12 Uhr Sa 01.03. / So 02.03. / 17 Uhr Neujahrskonzert Bacewicz / J.S. Bach / Kreisler / Beethoven Musici Volanti Salonorchester Mátyás Bartha Violine Piotr Plawner Violine Giovanni Barbato Violine Isabella Klim Violoncello Orlando Theuler Violoncello

 NEW PATIENT PAIN/SPINE INTAKE FORM
NEW PATIENT PAIN/SPINE INTAKE FORM