Supplementation with fruit and vegetable concentrate
decreases plasma homocysteine levels in a dietary
Michele F. Panunzioa,*, Alessandra Pisanoa, Antonietta Antonicielloa,
Vincenzo Di Martinoa, Lucia Frisolia, Vincenzo Cipriania,
aSection of Human Nutrition, Department of Health, Local Healthcare Unit Foggia, Piazza Pavoncelli n. 11,
bAesculapius Laboratory, Viale Telesforo-71100 Foggia, Italy
cNational Council of Research–Pisa, Italy
Received 3 February 2003; received in revised form 8 June 2003; accepted 11 June 2003
Abstract
An elevated level of total plasma homocysteine (tHcy) is considered to be a predictor of the
mortality risk for all diseases. A high consumption of vegetables and citrus fruit, both good sourcesof folate, decreases the concentration of tHcy. We investigated if supplementation of concentratedfruit and vegetables is able to decrease tHcy concentrations. For this purpose, we used a product thatis presently on the market, made up of fruit and vegetable powders. 26 subjects participated in across-over design intervention trial. At the end of the study, each participant received 2 capsules offruit and 2 capsules of vegetables a day for 4 weeks and then acted his/her own control for another4 weeks. Daily extract intake decreased plasma tHcy from an expected mean Ϯ SD level of 12.71 Ϯ3.23 umol/L observed after the 28-day control period to 7.98 Ϯ 1.70 umol/L, a difference of 4.73 Ϯ1.153 (p Ͻ 0.001).
Elevated tHcy is a risk factor causally linked to chronic disease. The plasma tHcy concentration
was decreased as a result of taking a powdered fruit and vegetable extract on a daily basis. 2003Elsevier Inc. All rights reserved. Keywords: Homocysteine; Folate; Vegetables; Fruit; Italy
* Corresponding author. Tel.: ϩ39-881-732-933; fax: ϩ39-881-732-929. E-mail address: [email protected] (M.F. Panunzio).
0271-5317/03/$ – see front matter 2003 Elsevier Inc. All rights reserved. doi:10.1016/S0271-5317(03)00133-7
M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–12281. Introduction
An increase in the consumption of fruit and vegetables has a high impact on public health.
Many studies have shown that 6 to 8 portions of fruit and vegetables a day reduce the riskassociated with increased oxidative cellular stress Homocysteine is directly involvedin oxidative damage and is considered to be an independent risk factor for cardiovascular andkidney diseases, for vascular dementia and for Alzheimer disease Recently, it hasbeen considered to be predictive for risk of all-cause adult mortality
Hyperhomocysteinemia can be congenital or acquired. The causes of the congenital form
relate to deficiencies of the enzymic systems (N5,N10 methylene-tetrahydrofolate reductase,cystathionine--synthase, cobalamin reductase, methionine synthase); while acquired hy-peromocysteinemia can be nutritional (deficiencies of vitamin B6, folate and vitamin B12),pharmacological (intake of methotrexate, carbamazepin, phenytoin, isoniazid, L-dopa), en-docrine (hypothyroidism) or due to other pathologies (such as kidney failure and psoriasis)Approximately 80% of total plasma homocysteine is bound to albumin by adisulfide bridge. Unbound homocysteine species exist mainly as homocysteine-cysteine orhomocysteine-homocysteine (homocystine) disulfides. Only 1% of all circulating homocys-teine exists as truly free homocysteine. Total homocysteine (tHcy) describes the sum of allthese free and protein-bound biochemical homocysteine species In fruit andvegetables there is a good concentration of vitamins in the B group, such as B-6 and folicacid, although vitamin B-12 is not present. The efficacy of these vitamins, in non-vegetariansubjects, suggest that a nutritional intervention with fruit and vegetables is practicable andcan be successful. We have studied the hypothesis that supplementation with concentratedfruit and vegetables decreases tHcy levels. 2. Subjects and methods
The primary end point was plasma tHcy reduction at 4 weeks. Assuming a two-sided type
I error of 5 percent, we estimated that we would need 19 subjects for the study to have 95percent power to demonstrate a mean (ϮSD) plasma tHcy reduction that was 1.5 (Ϯ1.7)umol/L greater in the treated group than in the control group Given an anticipateddropout rate of 35 percent, we set the enrolment at 30 subjects.
Thirty healthy men and women (15 men and 15 women), aged 20-56 yrs were recruited.
Exclusion criteria were: pregnancy, breast-feeding, gastrointestinal disorders, use of vitaminsand/or minerals, vegetarianism restricted caloric diets, regular intake of medicine, yeast orseaweed, malaria prophylactics or anti-convulsants in the 4 months prior to the study. On thebasis of these criteria, 26 subjects (12 men and 14 women) were considered eligible forparticipation in the trial. Written consent was requested from all participants for enrolmentin the study. The subjects under treatment took the fruit and vegetables concentrate twice aday for 4 weeks. No alimentary restrictions or changes in life-style were requested. M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
For the test, a product (Juice PlusTMϩ, manufactured by NSA International Inc., Fleet, UK
GU13 8UY) that is presently on the market and made up of fruit and vegetable powder wasused. The supplementation consisted in 2 capsules containing 1.7 grams of concentrated,powdered fruit extract (from apples, oranges, pineapples, blueberries, peaches and papaya)in the morning and 2 capsules containing 1.7 grams of concentrated, powdered vegetableextract (from carrots, parsley, beet-root, broccoli, black cauliflower, cabbage, spinach andtomato) in the evening, taken during meals.
The micronutrient concentrations declared on the label for 2 capsules of fruit are:
vitamin-C 90 mg, vitamin-E 15mg, vitamin B-1 0.4 mg, vitamin B-2 0.3 mg, vitamin B-6 2.0mg, niacin 7 mg and folic acid 100 mcg; for the vegetable ones: vitamin-C 50 mg, vitamin-E15 mg, vitamin B-1 0.6 mg, vitamin B-2 1.0 mg, vitamin B-6 1.5 mg, niacin 13 mg and folicacid 100 mcg, magnesium 45 mg and zinc 2.5 mg. The same product was examined inrelation to its constituents and its antioxidant power in a pilot study
The study was conducted according to a case-cross-over study design, with subjects
assigned at random to the treatment group and to the control group The cross-over,using subjects as their own controls enabled control of the possible confounding factors suchas sex, age, dietetic habits and smoking. The trial was divided into three time periods, eachone consisting of 28 days: the first treatment period, wash-out and the second treatmentperiod. During the 1st 27-day treatment period (days 0 to 27) the 13 subjects assigned toGroup 1 were supplemented daily with 2 capsules each of the powdered fruit and vegetableextract in the morning and evening, respectively, while the 13 subjects of Group 2 receivednothing. Following treatment period 1, both groups were subjected to a 28-day wash-outperiod (days 28 to 55). During the 2nd 27-day treatment period (days 56 to 82), Group 2received capsules of fruit and vegetable extract daily while Group 1 received nothing.
One plasma sample was collected of each participant on days 0, 14, 27, 56, 69 and 83, in
order to detect tHcy concentrations; another sample collected for determine serum folic acidlevels: on day 0 and on day 27 for group 1; on day 56 and on day 83 for group 2.
Dietary intake was estimated by means of food diary in which participants kept a record
of their daily food intake throughout the study period.
Levels of folic acid in serum were determined using the immunoenzymatic method
Colorimeter Enzymatic method was used to measure total cholesterol in serum Forhomocysteine, the analyses were carried out by an immunoenzymic methodology “Axishomocysteine EIA” in order to determine the presence of tHcy in plasma. The range ofmeasurement is 2-50 umol/L, the intra-assay coefficient of variation was Ͻ 5%, the inter-assay vc Ͻ 4%. In addition, an excellent correlation was found with the H.P.L.C. method
M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
In order to compare the changes which took place in tHcy and serum folic acid levels from
the starting point of both groups paired t-tests were used, for the analysis of the data theprogramme SPSS for Windows version 6.0.1 (SPSS Inc.,1989-1993) was utilized. P valuesϽ0.05 were considered moderately significant, Ͻ0,001 highly significant. Values in the textare means Ϯ SD. 3. Results
The characteristics of the participating subjects are shown in 12 men and 14
women with an average age of 35.6 years and a body mass of 24.2 participated. 10 subjectsregularly performed physical activities, 3 were smokers. The average level of cholesterol-emia was at 155.7 mg/dL. Most of the subjects normally consumed 1-2 portions of fruit andvegetables a day. The tHcy levels in plasma decreased throughout each period of treatmentbut not during the control periods of the study. In the results relative to supplemen-tation and its effect on tHcy in the subjects during the period of the trial are shown. tHcy
M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
Table 1Characteristics of subjects that participated in the study
levels decreased significantly in both groups. In group 1 the decreased was 4.1 (Ϯ 2.06)umol/L from day 0 (starting day of consumption of product) to day 27 (end of treatment); forgroup 2, tHcy decreased by 5.03 (Ϯ 1.39) from day 56 (beginning of consumption) to day83 (end of treatment), whereas plasma tHcy changed little during control periods for bothgroups. In the results of plasma tHcy levels are shown for subjects during both ofthe case cross-over periods of the study. During treatment periods when subjects took thepowdered extract plasma tHcy steadily decreased, by 2.34 (Ϯ 2.82) umol/L half-way throughand by 4.73 (Ϯ 1.53) umol/L by the 27th day of supplementation compared to controls.
Folic acid serum levels were for group 1: 4.1 (Ϯ 0.6) nmol/L on day 0 and 10.7 (Ϯ 1.1)
nmol/L on day 27 (P value Ͻ 0.001); for group 2: 4.2 (Ϯ 0.4) nmol/L on day 56 and 11.3(Ϯ 2.4) nmol/L on day 83 (P value Ͻ 0.001).
Table 2Effects of supplementation with concentrated fruit and vegetables on tHcy in subjects, during the period ofthe trial
Values are mean Ϯ SD. Values in cursive (italics) refer to the period of control, those in normal print refer to
Baseline: for subjects of group 1 ϭ day 0; for subjects of group 2 ϭ day 56. Student’s t-test: *P Ͻ 0.05; **P Ͻ 0.001. M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
Table 3Concentrations of plasma tHcy in the cross-over treatment periods
Values are mean Ϯ SD. 1 ϭ subjects treated: day 0 for group 1 and day 56 for group 2; subjects not treated: day 0 for group 2 and day
2 ϭ subjects treated: day 13 for group 1 and day 69 for group 2; subjects not treated: day 13 for group 2 and
3 ϭ subjects treated: day 27 for group 1 and day 83 for group 2; subjects not treated: day 27 for group 2 and
Significance level of P: NS ϭ not significant; * P Ͻ 0.005; **P Ͻ 0.001. 4. Discussion
This controlled dietary intervention study demonstrated that the daily consumption of 2
capsules of concentrated fruit and 2 capsules of concentrated vegetables has significantlydecreased plasma tHcy levels in 26 subjects whose normal fruit and vegetable consumptionis low. THcy levels decreased from an average of 12.71 (Ϯ3.23) during the control periodto 7.98 (Ϯ1.70) during the treatment period. Subjects, were asked not to change theirlifestyle, and each participant acted as his/her own control.
Many studies have demonstrated that providing folic acid or food rich in folate improved
folate status and at the same time decreased tHcy. Brouwer et al. (1999) discovered anaccentuated reduction in tHcy concentration after being given vegetables and citrus fruitHowever, the quantity of vegetables and citrus fruit provided every day (350 g. ofvegetables, 1 citrus fruit and 200ml. of citrus juice, reaching a level of dietary folate equalto 560 g/day) was higher than levels that may expected to be consumed in a generalpopulation. In our study the level of folate supplied by the capsules was 200 ug/day whichresulted in a steady, significant decrease of tHcy, reflected by a moderate decrease half-waythrough the treatment period that continued to decline through the last day of treatment. Theaverage values and changes in plasma tHcy in both periods observe in this study are inagreement with results of other studies, where supplemental folic acid or 5,10-MTHF wasused The decrease in tHcy values, with a difference of means of 4.73 (Ϯ1.53)umol/L, occurred with all 26 participants of the study.
In conclusion, we have shown that daily intake of supplements of powdered fruit and
vegetables extracts in capsular form significantly decreased plasma levels of tHcy in healthysubjects, just as the interruption of intake allowed tHcy return to pre-supplementation levels. A homocysteine lowering effect may be only part of the health benefit associated withconsuming fruit and vegetable extracts on a daily basis. In the other study, the same productdecreased DNA damage in the peripheral lymphocytes of an elderly population
Further studies are in course to demonstrate if the decrease of tHcy is associated with a
decrease of the risk of pathologies in which it is implicated. However, already the results of
M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
the first studies are encouraging. For example, in a prospective study of 4.4 years, Petersonet al. found that after Hcy-lowering treatment with vitamin supplementation, the rate ofprogression of carotid plaque formation before and after supplementation was significantlyreduced If this were to be confirmed by other research it would mark a decisive moveforwards in the nutritional prevention of disease. Acknowledgments
The authors thank the volunteers for their participation and the “Scardi Group” for having
References
[1] Heber D, Bowerman S. Applying science to changing dietary patterns. J Nutr 2001;131:3078S– 81S. [2] Messina M, Lampe JW, Birt DF, Appel LJ, Pivonka E, Berry B, Jacobs DR. Reductionism and the
narrowing nutrition perspective: time for reevaluation and emphasis on food synergy. J Am Diet Assoc2001;101:1416 –1419.
[3] Trobs M, Renner T, Scherer G, Heller WD, Geiss HC, Wolfram G, Haas GM, Schwandt P. Nutrition,
Antioxidants, and Risk Factor Profile of Nonsmokers, Passive Smokers and Smokers of the PreventionEducation Program (PEP) in Nuremberg, Germany. Prev Med 2002;34:600 – 607.
[4] Hermann W. The importance of hyperomocysteinemia as a risk factor for deseases: an overview. Clin Chem
[5] Sasaki T, Watanabe M, Nagai Y, Hoshi T, Takasawa M, Nukata M, Taguchi A, Kitagawa K, Kinoshita N,
Matsumoto M. Association of Plasma Homocysteine Concentration With Atherosclerotic Carotid Plaquesand Lacunar Infarction. Stroke 2002;33:1493–1496.
[6] Sanchez Bayle M. Homocysteine as a cardiovascular risk factor. An Esp Pediatr 2002;56:399 – 401. [7] Ducloux D, Motte G, Massy ZA. Hyperhomocyst(e)inemia as a risk factor after renal transplantation. Ann
[8] Myers KA. Elevated homocysteine: a new marker for dementia? CMAJ 2002;166:1068. [9] Nilsson K, Gustafson L, Hultberg B. Relation between Plasma Homocysteine and Alzheimer’s Disease.
Dement Geriatr Cogn Disord 2002;14:7–12.
[10] Malinow R M. Plasma concentrations of total homocysteine predict mortality risk. Am J Clin Nutr
[11] Vollset SE, Refsum H, Tverdal A, Nygård O, Nordrehaug JE, Tell GS, Ueland PM. Plasma total homo-
cysteine and cardiovascular and noncardiovascular mortality: the Hordaland Homocysteine Study. Am JClin Nutr 2001;74:130 –136.
[12] Clarke R, Woodehouse P, Ulvik A, et al. Variability and determinants of total homocysteine concentrations
in plasma. Clin Chem 1998;44:102–107.
[13] Garg UC, Zheng Z-J, Folsom AR, et al. Short-term, and long-term variability of plasma homocysteine
measurement. Clin Chem 1997;43:141–145.
[14] Moustapha A, Robinson K. Homocysteine: An emerging age-related cardiovascular risk factor. Geriatrics,
[15] Selhub J. Homocysteine metabolism. Annu Rev Nutr 1999;19:217–246. [16] Finkelstein JD. The metabolism of homocysteine: pathways and regulation. Eur J Pediatr 1998;157:S40 –
[17] Jacobsen DW. Biochemistry and Metabolism. In: Robinson K, editor. Homocysteine and Vascular Diseases.
Kluwer Academic Publishers, 2000:p. 16 –34. M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
[18] Brouwer IA, van Dusseldorp M, West CE, Meyboom S, Thomas CMG, Duran M, van het Hof KH, Eskes
TKAB, Hautvast JGAJ, Steegers-Theunissen RPM. Dietary folate from vegetables and citrus fruit decreasesplasma homocysteine concentrations in humans in a dietary controlled trial. J Nutr 1999;129:1135–1139.
[19] Choen J. Statistical power analysis for the behavioural sciences. New York: Academic Press, 1977. [20] Wise JA, Morin RJ, Sanderson R, Blum K. Changes in plasma carotenoid, alpha-tocopherol, and lipid
peroxide levels in response to supplementation with concentrated fruit and vegetable extracts: a pilot study. Curr Ther Research 1996;57:3–19.
[21] McNeely MDD. Folic Acid assay. In: Kaplan LA, Pesce AJ, editors. Clinical Chemistry. St. Louis: CV
[22] McNamara JR, Leary ET, Ceriotti F, Boersma-Cobbaert CM, Cole TG, Hassemer DJ, et al. Point: status of
lipid and lipoprotein standardization. Clin Chem 1997;43:1306 –10.
[23] Candito M, Causse E, Couderc R, Demuth K, Drai J, Gachon AM, Garcia I, Gerhardt MF, Philippe-
Bourgeois C, Quillard M, Read MH, Sauvant MP, Ducros V. Determination of total plasma homocysteine:preanalytical parameters, method comparison and interchangeability. Ann Biol Clin 2002;60:317–319.
[24] Brouwer IA, van Dusseldorp M, Thomas CMG, Duran M, Hautvast JGAJ, Eskes TKAB, Steegers-
Theunissen RPM Low-dose folic acid supplementation decreases plasma homocysteine: A randomised trial. Am J Clin Nutr 1999;69:99 –104.
[25] Jacob RA, Wu M-M, Henning SM, Swenseid ME. Homocysteine increases as folate decreases in plasma of
healthy men during short-term dietary folate and methyl group restriction. J Nutr 1984;124:1072– 80.
[26] O’Keef CA, Bailey LB, Thomas EA, Hofler SA, Davis BA, Cerda JJ, Gregory JF. III Controlled dietary
folate affects folate status in nonpregnant women. J Nutr 1995;125:2717–25.
[27] Ward M, McNulty H, McPartlin J, Strain JJ, Weir DG, Scott JM. Plasma homocysteine, a risk factor for
cardiovascular disease, is lowered by physiological doses of folic acid. Q J Med 1997;90:519 –24.
[28] Smith MJ, Inserra PF, Watson RR, Wise JA, O’Neil KL. Supplementation with fruit and vegetables extracts
may decrease DNA damage in the peripheral lymphocytes of an elderly population. Nutr Res 1999;19:1507–18.
[29] Peterson JC, Spence DJ. Vitamins and progression of atherosclerosis in hyper-homocysteinemia. Lancet
Sildenafil Inhibits Altitude-induced Hypoxemia and Pulmonary Hypertension Jean-Paul Richalet, Pierre Gratadour, Paul Robach, Isabelle Pham, Miche`le De´chaux, Aude Joncquiert-Latarjet, Pascal Mollard, Julien Brugniaux, and Je´re´my Cornolo Laboratoire Re´ponses cellulaires et fonctionnelles a` l’hypoxie, Universite´ Paris 13, Bobigny; Service de Physiologie et Explorations Fonctionnel
Background Briefing For those who care about the human future. All the confused talk and violence: what does it mean? Dr. Al Sears; Quote: ". Will this change? To understand why activities such The pharmaceutical giant Wyeth is being sued over its as mentioned above are allowed, even encouraged, synthetic hormone drugs Premarin and Prempro. They first learn basic logic. The c
 Supplementation with fruit and vegetable concentrate
decreases plasma homocysteine levels in a dietary
Michele F. Panunzioa,*, Alessandra Pisanoa, Antonietta Antonicielloa,
Vincenzo Di Martinoa, Lucia Frisolia, Vincenzo Cipriania,
aSection of Human Nutrition, Department of Health, Local Healthcare Unit Foggia, Piazza Pavoncelli n. 11,
bAesculapius Laboratory, Viale Telesforo-71100 Foggia, Italy
cNational Council of Research–Pisa, Italy
Received 3 February 2003; received in revised form 8 June 2003; accepted 11 June 2003
Abstract
Supplementation with fruit and vegetable concentrate
decreases plasma homocysteine levels in a dietary
Michele F. Panunzioa,*, Alessandra Pisanoa, Antonietta Antonicielloa,
Vincenzo Di Martinoa, Lucia Frisolia, Vincenzo Cipriania,
aSection of Human Nutrition, Department of Health, Local Healthcare Unit Foggia, Piazza Pavoncelli n. 11,
bAesculapius Laboratory, Viale Telesforo-71100 Foggia, Italy
cNational Council of Research–Pisa, Italy
Received 3 February 2003; received in revised form 8 June 2003; accepted 11 June 2003
Abstract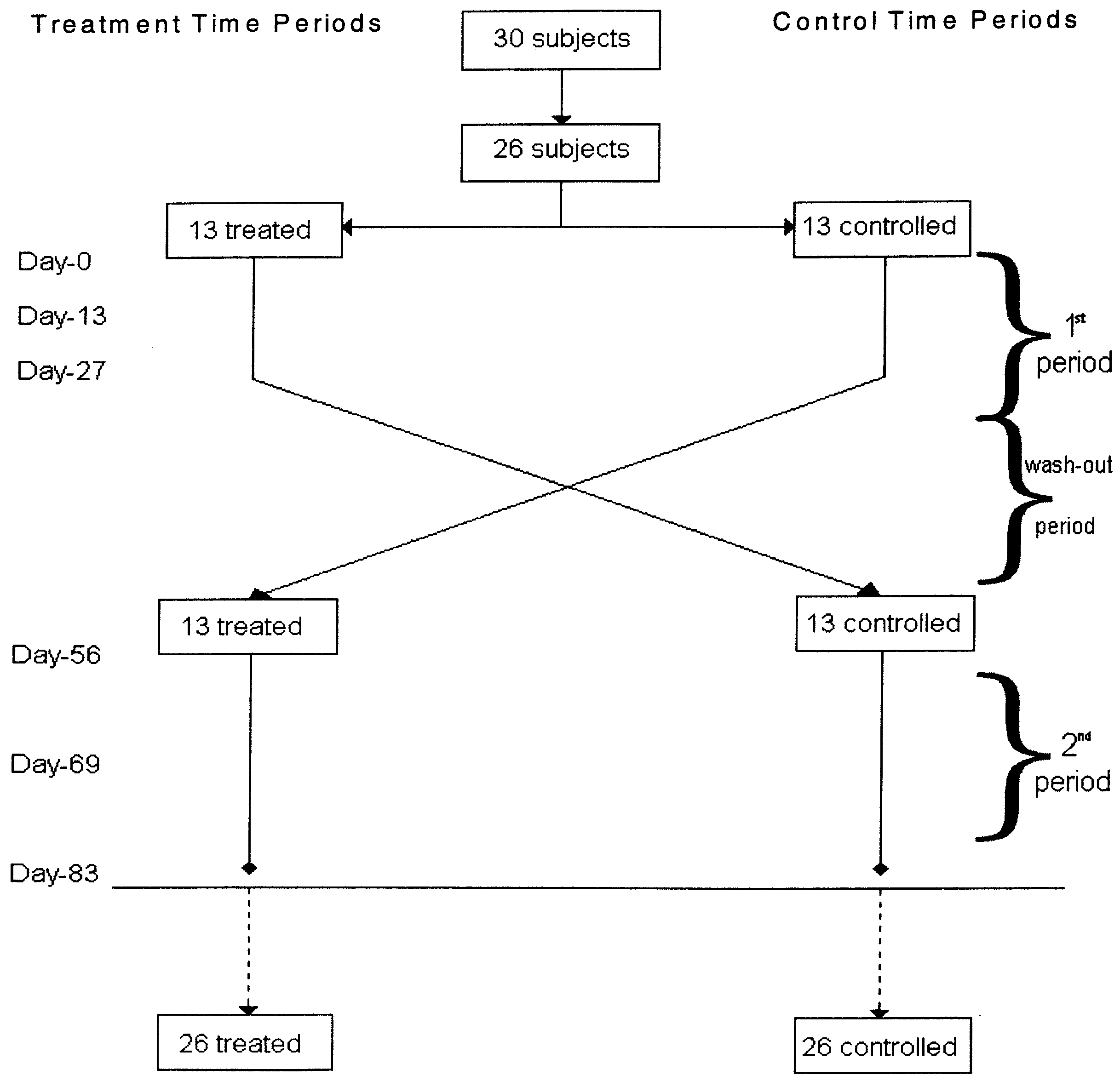 M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
In order to compare the changes which took place in tHcy and serum folic acid levels from
the starting point of both groups paired t-tests were used, for the analysis of the data theprogramme SPSS for Windows version 6.0.1 (SPSS Inc.,1989-1993) was utilized. P valuesϽ0.05 were considered moderately significant, Ͻ0,001 highly significant. Values in the textare means Ϯ SD.
M. F. Panunzio et al. / Nutrition Research 23 (2003) 1221–1228
In order to compare the changes which took place in tHcy and serum folic acid levels from
the starting point of both groups paired t-tests were used, for the analysis of the data theprogramme SPSS for Windows version 6.0.1 (SPSS Inc.,1989-1993) was utilized. P valuesϽ0.05 were considered moderately significant, Ͻ0,001 highly significant. Values in the textare means Ϯ SD.